Transcription
2016 Issue 2ON THEBRINKJamie Bakkum-Gamez, M.D.,is on a course to changewomen’s health careHope for young patientsGame changerMajor milestone
CONTENTS2016Issue 2FEATURESConnecting disparate investigators 24Mayo Clinic advances incancer diagnosis, treatmentand prevention Mayo Clinic Cancer Center reportYoung Investigators Research SymposiumBalfour Award forMeritorious Research 262 Endometrial cancer testing breakthrough Pediatric Brain Tumor ClinicWisit Cheungpasitporn, M.D.810 Colorectal cancer screening game changer Breast cancer vaccine milestone20 Prostate cancer imaging development16Kendall Award forMeritorious Research 28Jacqueline Limberg, Ph.D.Know your Board of Directors 3022MAYO UPDATE 31 Zika virus vaccine developmentNew executive dean for educationNew nanotechnology research lab in FloridaNew Department of Clinical GenomicsFlorida neurogeneticist receives Potamkin Prizefor ResearchCEO honored for research advocacyOne-of-a-kind 3T compact MRI scannerAlumni Association Board member awardsObituariesNeurologist awarded John Dystel Prizefor MS Research
Letter fromthe secretarytreasurerWe’ve all been touched by cancer — a parent, a friend, aspouse or partner, a colleague, a child or oneself. Whilethe diagnosis is still accompanied by fear, there are manyreasons to be hopeful. This issue of Mayo Clinic Alumniincludes stories about advances in cancer prevention,diagnosis and treatment at Mayo Clinic, affectingchildren, women and men. You’ll see language suchas on the brink, game changer and major milestone.In 1977 Charles Moertel, M.D., then-director ofMayo Clinic Cancer Center, provided a spirited state-ofcancer-care report for the alumni magazine. We use thatas the springboard for a current look at cancer care atMayo Clinic. One key area in which we’ve progressedin the 39 years between these reports is in translatingknowledge from our research into patient care.Case in point, our researchers have developed anewly commercialized noninvasive colorectal cancerscreening tool, and are developing the first-everscreening tool for endometrial cancer — hopefullyto be commercialized within two years. We’re alsoconducting vaccine trials for breast cancer and areestimating we’ll have vaccines to prevent severalcancers within 10 years. And for our youngest patients,we’re on a path to have a better treatment for highgrade brain tumors in four to five years.Peter C. Amadio, M.D. Secretary-Treasurer, Mayo Clinic Alumni Association Lloyd A. and Barbara A. Amundson Professor of OrthopedicsIndeed, research informs our patient care across theboard. You’ll see this focus is alive and well in the storiesabout the Young Investigators Research Symposium andthe Balfour and Kendall awards for meritorious research.In the next issue of this magazine, we’ll report onthe International Meeting in Whistler, British Columbia,Canada. Be sure to mark your calendar for the nextBiennial Meeting (back cover), which is only a littlemore than a year away. In October 2017 we’ll gather inFlorida — in Jacksonville for the CME program andPonte Vedra Beach for lodging and socializing. I hopeto see you there.ABOUT THE COVER Jamie Bakkum-Gamez, M.D (OBG ’06,2016 Issue 2ON THEBRINKJamie Bakkum-Gamez, M.D.,is on a course to changewomen’s health careHope for young patientsGame changerMajor milestoneGYNO ’09), Division of Gynecologic Surgery at Mayo Clinic in Rochester,has developed a minimally invasive testing modality to detect endometrialcancer by sensitive molecular testing. This innovation will be the firstscreening or early-detection test for endometrial cancer.Issue 2 20161
Mayo Clinic Cancer CenterTHE PROGNOSISIS GOODChThirty-nine years later, I doubt anyone still needs tobe convinced that this statement is true. The U.S. Newsand World Report 2015 2016 rankings list MayoClinic at number three on its list of besthospitals for adult cancer care.The Mayo Clinic Cancer Centerhas grown and matured in manyways since Dr. Moertel wrote hisreport. In 1977 Mayo Clinic saw21,000 cancer patients. In 2013we saw 122,000 cancer patientsat Mayo Clinic. In 1977, 196 MayoClinic staff had a “major or totalcommitment to cancer.” Today morer lesMthan1,100 Mayo Clinic physicians,oer t e l,care providers and researchers play a roleM.D.in caring for our cancer patients.a2MAYO CLINIC ALUMNIertDiasio,M.D.RoIn 1977 Charles Moertel, M.D. (I ‘58), director of whatwas then called the Mayo Comprehensive CancerCenter, gave a report on the current state of the center.In conclusion, he said:“ I hope I have convinced you that the primarypurpose of the Center is to bring the best possiblecancer care to today’s cancer patient and totomorrow’s cancer patient; that the Center is amechanism for enriching the practice of a largeproportion of our staff through integration ofbasic research, clinical research, and clinicalpractice; that the Center is a fiscally soundoperation that provides no threat to us, todayor tomorrow; and that a strong ComprehensiveTo read Dr. Moertel’sCancer Center will help ensure the continued1977 overview, visitalumniassociation.identity of Mayo Clinic as among the finestmayo.edu.tertiary care centers anywhere.”bby Robert Diasio, M.D.,Director, Mayo Clinic Cancer CenterWilliam J. and Charles H. Mayo ProfessorA leading-edge research centerThe Mayo Clinic Cancer Center is ranked sixth amongcomprehensive cancer centers in the amount offunding received from the National Cancer Institute(NCI). After the most recent NCI competitive grantrenewal in 2013, the Mayo Clinic Cancer Centerearned the NCI’s highest ranking — exceptional —and received 28.6 million in funding over five years.Today we also receive more than 109.7 million incompetitive peer review grants that support cancerresearch, including the NCI’s highly sought-afterSpecialized Programs of Research Excellence (SPORE)grants. SPORE grants support projects intended toproduce new approaches to the prevention, earlydetection, diagnosis and treatment of cancer. TheMayo Clinic Cancer Center has five NCI SPORE grantsand one SPORE grant that is shared with anotherinstitution. These grants support research in braincancer, breast cancer, multiple myeloma, ovariancancer, pancreatic cancer and lymphoma.
We’ve become a leader in translating knowledgegained from cancer research into better patient care.We have 10 major cancer research programs thattranslate scientific discoveries in the laboratory intoleading-edge treatments and therapies for patients:Cancer Immunology and ImmunotherapyCancer Prevention and ControlCell BiologyDevelopmental TherapeuticsGastrointestinal CancerGene and Virus TherapyGenetic Epidemiology and Risk AssessmentHematologic MalignanciesNeuro-oncologyWomen’s CancerMore than 330 Mayo Clinic Cancer Center memberresearchers and about 250 allied health staff contributeto our research initiatives. These efforts are bolstered byresearch support services that provide access to cuttingedge technology and methodology, scientific consultation,reliability, cost-effectiveness and quality control.These resources help to provide our patients withaccess to hundreds of clinical trials led by Mayo Clinicphysicians and scientists. Even more trials are availablethrough cooperative research agreements with theNCI and clinical trial study groups.THEN21,000MAYO CLINIC CANCER PATIENTS122,000NOWThe NationalCancer Institute (NCI)awarded the Mayo ClinicCancer Center itshighest ranking:EXCEPTIONALIssue 2 20163
.ran eence str s a inpe )cimen(gnciotncali f i c o l opFluaamoreme it y inoscesloirnt mtbnaicrograph illustrates cein s tomicnegethat c a n d r iv4MAYO CLINIC ALUMNIWe play a leadership role in the nation’s clinicaltrial study groups and receive NCI funding to serveas one of 30 Lead Academic Participating Sites in theNCI National Clinical Trials Network, the Statisticsand Data Center for the Alliance for Clinical Trialsin Oncology, and the Alliance NCI CommunityOncology Research Program Research. Our othernational research initiatives include: Leading the NCI-funded LymphomaEpidemiology of Outcomes Cohort Study, whichwill enroll 12,000 patients with non-Hodgkinlymphoma and follow them to learn more abouttheir long-term prognosis and survivorship Serving as the administrative and research basefor the Cancer Prevention Network, a clinicaltrial study group Conducting phase I clinical trials of new anticancer agents or combinations of agents as partof an NCI Experimental Therapeutics ClinicalTrials Network grant Serving as the base for the Pancreatic CancerGenetic Epidemiology Consortium, a group ofNCI-funded individuals searching for the geneticunderpinnings of pancreatic cancer Hosting the Research Coordinating Center forAcademic and Community Cancer Research United
Research-driven, patient-centered careDr. Moertel called for “the wave of the future in cancermanagement [to] bring the fruits of the basic sciencelaboratory to the bedside of the patient.” Thirty-nineyears later our cancer research transforms our cancerpractice on a daily basis.In 2014 researchers at the Mayo Clinic CancerCenter proved they had developed an effectivenew method of screening for colorectal cancer thatuses stool DNA (page 16). Called Cologuard, thescreening test was developed to provide a new choicein colorectal cancer screening. Research shows thatpatients who are offered alternatives are more likelyto comply with screening. Cologuard is mailed topatients at home and requires only a stool sample. It iseasy to use, inexpensive, and requires no bowel prep,medication or dietary restrictions. Colonoscopy, themost widely used screening method, is expensiveand requires bowel prep, sedation and time off work.Cologuard may help remove some of the barriers thatprevent people from getting screened.In 2015 Mayo Clinic researchers demonstratedthat it was possible to detect endometrial cancerusing tumor DNA picked up by ordinary tampons(page 8). The new approach specifically examinesDNA samples from vaginal secretions for thepresence of chemical “off” switches — known asmethylation — that can disable genes that normallykeep cancer in check. The finding is a critical steptoward a convenient and effective screening test forendometrial cancer, the most common gynecologicmalignancy in the United States.1,100Mayo Clinicphysicians, careproviders andresearchers care forour cancerpatientsMay 2015MinnesotaProton BeamTherapy ProgramMarch 2016ArizonaWe collaborate closely with the Mayo Clinic Centerfor Individualized Medicine to use genetics to moreeffectively and precisely diagnose, treat, predict andprevent cancer. Some highlights from our advancesin targeted and precision medicine over the pastyear include: A team of Mayo Clinic researchers announcedthat it had succeeded in identifying the sourceof cancer in patients’ gastrointestinal tracts byanalyzing DNA markers from tumors. The resultsopen the possibility that physicians could one dayscreen for cancer anywhere in the body with anoninvasive blood test or stool sample. Herceptin has been touted as a wonder drug forwomen with HER2-positive breast cancer, anaggressive form of the disease that is fueled byexcess production of the HER2 protein. However,not all of these patients respond to the drug,and many who do respond eventually acquireresistance. A team of researchers led by MayoClinic found a promising way to circumvent thisobstacle. They identified a small site in the HER2protein that enables it to form a molecular switchthat sets off a cascade of events that turn normalcells cancerous. The researchers showed thatdisrupting this site can stem the growth of breastcancer cells even more effectively than drugscurrently used in the clinic.Issue 2 20165
r izoer,Anti,MertnnneCerCes ot aerCeM ayo C lin i ccanMayo Clinic Ca ncWe embrace new technology to provide the bestpossible cancer treatment for our patients. The MayoClinic Cancer Center launched a Proton Beam TherapyProgram on our Minnesota campus in May 2015 andon our Arizona campus in March 2016. The radiationbeam used in proton beam therapy targets only thetumor, better sparing surrounding healthy tissuefrom harm. Proton beam therapy is used to treat manykinds of cancers located deep within the body andclose to critical organs and body structures, especiallyin children and young adults.We’re constantly looking to expand our reach inadvancing the science and practice of cancer care. In2014 the Mayo Clinic Cancer Center became a memberof the National Comprehensive Cancer Network(NCCN), a not-for-profit alliance of leading cancercenters dedicated to improving the quality, effectivenessand efficiency of care for cancer patients. Forty-sevenMayo Clinic representatives now serve on 47 differentNCCN Guidelines Panels. Together with other NCCNmember institutions, we’re working to continuouslyadvance our national expertise in cancer care.na A team of researchers, including scientists fromthe Translational Genomics Research Institute(TGen) and Mayo Clinic, reported that analyzingcirculating tumor DNA can track how a patient’scancer evolves and responds to treatment. Thistype of blood test, known as a liquid biopsy, isless invasive, less costly and less risky thanconventional tissue biopsies, which essentially areminor surgeries. Obtaining liquid biopsies couldoccur more frequently too, providing physicianswith up-to-date information about how a patient’scancer might be changing and helping in theselection of the best possible treatments to combat it.Mayo Clini cCancerCeer,ntFlo– Robert Diasio, M.D.6MAYO CLINIC ALUMNIr i daWe’ve made incredible progress in thealmost four decades since Dr. Moertelwrote his report.”
The prognosis is good —with increased research fundingWe’ve made incredible progress in the almost fourdecades since Dr. Moertel wrote his report. Sincethen, advances in biomedical research have helped usbetter understand the collection of diseases we callcancer. We now know that genetic mutations causemost cancers — knowledge that has launched the eraof precision medicine. According to the AmericanAssociation of Cancer Research (AACR), as of July 31,2015, there were 52 different therapeutics targetingspecific molecules involved in cancer. Precisiontherapy and immunotherapy have been firmlyestablished as the future of cancer care.More people diagnosed with cancer now survivethe diagnosis. In 1975 the five-year relative survivalrate for all cancers combined was 49 percent. By 2010it had risen to 68 percent. From 2002 to 2011 overallcancer death rates declined by 1.8 percent per yearfor U.S. men, by 1.4 percent per year for U.S. womenand by 2.1 percent per year for 0 19 year olds.Despite such progress, cancer remains a weightydiagnosis. It is estimated that 8.9 million people willdie from some form of cancer in 2015 — 589,430 ofthose people in the United States. Cancer still accountsfor one in four deaths in the United States and one inseven deaths worldwide. Cancer is the number-onecause of disease-related death among U.S. children.And the number of cancer diagnoses is expected togrow — from 1,658,370 U.S. cancer cases in 2015, to2,387,304 in 2035 (AACR Cancer Progress Report 2015).Sadly, our continued progress in understandingand treating cancer remains at risk. Budgets for theNational Institutes of Health (NIH) and NCI have notkept pace with inflation. Direct cuts in 2011 and 2013further eroded budgets. The AACR reports that since2004 the NIH has lost approximately 25 percent of itsability to fund lifesaving biomedical research.If we are to secure continued progress in the fightagainst cancer, we must urge Congress to increasefunding for the NIH and the NCI.As the Mayo Clinic Cancer Center looks to thefuture, our vision echoes that of Dr. Moertel — tocontinue to build and strengthen an integrated cancerpractice across all Mayo Clinic sites, departments,service lines and care delivery platforms. A practicethat provides an unparalleled health care experienceto our patients.Remembering our primary value as an institution —the needs of the patient come first — will ensureMayo’s continued status as one of the finest cancercenters in the world.Issue 2 20167
ON THE BRINKFirst-ever screening test for endometrial cancerJamie Bakkum-Gamez, M.D. (OBG ’06, GYNO ’09),is on a course to change women’s health care.Her work could yield results similar to that ofGeorgios Papanikolaou, M.D., inventor of the Paptest used around the world to detect and preventcervical cancer and other diseases of the femalereproductive system.Dr. Bakkum-Gamez, Division of GynecologicSurgery at Mayo Clinic in Rochester, is working on thedevelopment of a minimally invasive testing modality— a tampon — to detect endometrial cancer bysensitive molecular testing (DNA methylation). Thiswill be the first screening or early-detection test forendometrial cancer.“The Pap test changed the lives of millions ofwomen, and a screening test for endometrial cancercould do the same,” she says. “Our goal has alwaysbeen to improve the outcomes for women at risk forendometrial cancer — to prevent cancer or at leastdetect it earlier. Ultimately we want to save lives.”Support externally, internally andfrom women around the countryDr. Bakkum-Gamez’s research has been funded bythe National Cancer Institute and Mayo Clinic, whichrecently awarded her team a Transform the PracticeTeam Award to push the work toward a commerciallyavailable clinical test within two years.Women from around the U.S. have contactedMayo Clinic to participate in the ongoing clinical trial.“We’ve had immense support for this project,including Mayo’s Department of Research, whichrecognizes this aspect of women’s health as importantand deserving of support and research,” saysDr. Bakkum-Gamez. “Our work has only been possibledue to a multidisciplinary team with expertise fromLaboratory Medicine and Pathology, ExperimentalPathology, and OB/GYN providers across the enterprise,including nurse practitioners and physician assistants.”With baby boomers now in the age risk category forendometrial cancer, the number of women diagnosedeach year is increasing, as is the mortality rate. Blackwomen have lower incidence than Caucasian womenbut have a higher mortality rate, likely attributable toaccess to medical care.“We’re working on an epidemiologic study tovalidate risk predictors and determine when womenshould be screened,” says Dr. Bakkum-Gamez.“Because our test is a first, we don’t have existingguidelines to steer us.”This is a low-cost, easy-to-access screening test thatcould address racial and socioeconomic disparities inmortality from endometrial cancer.”– Jamie Bakkum-Gamez, M.D.8MAYO CLINIC ALUMNI
Jamie Bakkum-Gamez, M.D.Learning from Cologuard experienceDr. Bakkum-Gamez points out that the simplicity of thetampon test will be similar to Cologuard for colorectalcancer — a prescribed, self-administered mail-in test(page 16). These features may help to overcome accessto-care barriers. “A low-cost, easy-to-access screeningtest could address racial and socioeconomic disparitiesin mortality from endometrial cancer.”Her team continues to work on fine-tuning thegene panel, with help from David Ahlquist, M.D., whodeveloped Cologuard, and his team in the Division ofGastroenterology and Hepatology.“Dr. Ahlquist is collaborating with us to make surewe’re being as comprehensive as possible and notmissing a potential signature gene,” says Dr. BakkumGamez. “We’re learning from his Cologuard experienceand expertise.”Easier way to obtain specimens for analysisIn addition to early detection of endometrial cancer, thetest also promises to improve the patient experience.“Women can have signs of endometrial cancer that turnout to be caused by a polyp or dysfunctional uterinebleeding,” she says. “Currently, they may have to havean endometrial biopsy to rule out cancer. Our test willprovide a way to obtain specimens for analysis morecomfortably.“This is an exciting time in women’s health aswe’re on the brink of introducing a life-changingtest for cancer.”Issue 2 20169
HOPE FORYOUNG PATIENTSPediatric Brain Tumor ClinicAddyson Cordes, now almost 5 years old, wasdiagnosed at age 13 months with an atypicalteratoid/rhaboid tumor (AT/RT), a rare andaggressive malignant brain tumor. Neurosurgery,chemotherapy and proton beam therapy followed, allbefore she was 3. She has needed additional Mayo Clinicservices including physical medicine and rehabilitation,audiology, ophthalmology and endocrinology dueto side effects of her treatment. She’ll continue to bemonitored throughout her life.Addyson has benefited from Mayo’s Pediatric BrainTumor Clinic, which was established right around thetime she was born.Neuro-oncology-led teamAddyson’s parents, Michele Zidlicky and NathanCordes, of Wanamingo, Minnesota, have had a centralAmul ya10MAYO CLINIC ALUMNINageswa ra Rao, M.B.B.S.contact for and coordination of all of their daughter’scare at Mayo Clinic. Before the Pediatric Brain TumorClinic was created, patients’ parents worked with theneuro-oncologist, neurosurgeon, radiation oncologistand other specialty services separately.“Prior to having this integrated approach, parentsreceived information in a less connected way, whichmade their decision-making more difficult,” saysAmulya Nageswara Rao, M.B.B.S. (PDHO ’10), a neurooncologist and director of the Pediatric Brain TumorClinic. “Now we bring together all of the experts, ledby the neuro-oncologist, who serves as the primaryphysician. We explain what the months and yearsahead will look like and what the challenges will be.This makes the family’s journey easier.”Zidlicky says everyone involved in her daughter’scare has been wonderful, but Dr. Nageswara Rao hasbeen an important point person. “When Addy was onthe rehab floor, Dr. Rao came to talk to us just to learnmore about us, what we do for work and fun, and whatour concerns were. She understood we were scared thatour most precious gift would be taken away from us.She and everyone on the team talk to us in a way wecan understand — not using medical terms.”Clinic’s genesisDr. Nageswara Rao had a vision to establish the clinicwhen she was a pediatric hematology/oncology fellowat Mayo Clinic in 2007.“I’d wanted to work with kids since medical school,”she says. “I chose Mayo Clinic for my fellowship becauseof its reputation for the team approach to medicine.
Addyson Cordeshas benefited fromcoordinated carein the PediatricBrain Tumor Clinic.
I began to establish the relationships I’d need for acomprehensive clinic. As I started to work in oncology,I realized our work goes beyond cures. These youngpatients endure the long-term effects of cancer and itstreatment. Our work must involve making sure they alsohave the best adulthood possible and helping with allaspects of the care they need throughout their lives.”To establish the clinic she envisioned, Dr. NageswaraRao wanted additional training and experience. Shepursued a subsequent fellowship in pediatric neurooncology at Children’s National Medical Center inWashington, D.C., training with Roger Packer, M.D.,a well-known figure in pediatric brain tumors.“I planned to learn a good care practice model,return to Mayo to establish a pediatric brain tumorclinic, and bring together the right team to providepatients and their families with comprehensive,integrated care,” she says.Proton beam therapy —powerful advance forpediatric tumor treatmentMayo Clinic’s Proton Beam Therapy Program Rochestercampus opened a year ago. The program on the Arizonacampus opened this spring. To date in Rochester, almostone-fourth of patients treated with proton beam therapyhave been children.Because of their increased sensitivity to the effectsof radiation, children may particularly benefit from protonbeam therapy’s precision. Mayo Clinic uses intensitymodulated proton beam therapy with pencil beam scanning,closely targeting tumors and sparing healthy tissue.“Although reducing unnecessary radiation is beneficialfor many cancer patients, children with cancer stand tobenefit the most from proton beam therapy,” says NadiaLaack, M.D. (RADO ’06), a pediatric radiation oncologist atMayo Clinic in Rochester. “Proton radiotherapy reduces thelow-dose radiation exposure that is seen with conventionalradiation. Because their organs are still developing, childrencan have significant long-term harm from even low dosesof radiation including growth problems, hearing and visionloss, radiation-induced cancers and heart disease.”12MAYO CLINIC ALUMNIClinic realizedDr. Nageswara Rao returned to Mayo Clinic in 2011 andoutlined the comprehensive team model for the clinic.“These types of tumors are challenging andcomplex, and require an integrated team approach tohelp with decision-making,” she says. “As the newcomprehensive clinic was formed, we agreed that ourexperts would come together and determine a courseof action that we would discuss with the family to helpthem make decisions. Every division that would beinvolved in caring for these patients was immediatelysupportive and shared a vision to help these children.”In addition to neuro-oncology, neurosurgery,radiation oncology and neurology, patients oftenneed care from endocrinology, neuropathology,neuroradiology, neuropsychology, audiology, andphysical medicine and rehabilitation.Today the Mayo Clinic Pediatric Brain Tumor Clinicdiagnoses 60 to 70 new patients a year and treatsmany recurrent tumors. Treatment advances includecomputer-assisted brain surgery, brain-mappingtechniques, intraoperative MRI, awake brain surgery,proton beam therapy, and chemotherapy ranging from aphase I clinical trial to bone marrow transplantation.Dr. Nageswara Rao, with the support of Mayo Clinicneuropathologist Caterina Giannini, M.D., Ph.D.(N ’89, APATH ’94, NPATH ’96), has been building arobust research component into the clinic, includingestablishing tumor banks and national and international
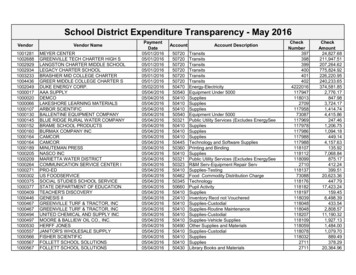
The brain trust of the Pediatric Brain Tumor Clinic includes(from left) Gesina Keating, M.D. (MED ’91, PDN ’96),neurology; David Daniels, M.D., Ph.D. (PRES ’08, NS ’13),neurosurgery; Amulya Nageswara Rao, M.D., neurooncology; and Nadia Laack, M.D., radiation oncology.Issue 2 201613
collaborations. One of these is for diffuse intrinsic pontinegliomas (DIPGs) — fatal brain tumors with no cure.She also developed national and internationalpartnerships for clinical trials. In 2015 Mayo Clinicstarted a new phase I clinical trial in pediatric cancer(page 15).“All of these specialties have expertise in differentaspects of diagnosis and treatment of kids with braintumors,” says Dr. Nageswara Rao. “We try to achieve acure and ensure the best functional and neurocognitiveoutcomes for each child.”Addyson’s caseAddyson Cordes was no exception. She recently markedthree years since completing treatment. “She’s stable buthas to be watched,” says Zidlicky. “We return to Mayoregularly for scans.”Zidlicky says the family’s outlook is markedlydifferent from when her daughter was diagnosed. It waspredicted Addyson would not live past 2 years old, inpart because of the aggressive nature of the tumor andthe effects treatment would have on someone so young.“When Addy was diagnosed, we faced having onlya few months left with her,” says Zidlicky. “Dr. Rao toldus it wasn’t an easily treatable cancer, and it had alreadyspread to the spinal fluid and spinal cord. She said it wasthe fourth AT/RT case Mayo had seen, and the otherchildren hadn’t survived. She was honest with us fromthe start about how bad it was and what to expect.”Addyson had surgery followed by rehabilitationtherapy at Mayo Clinic to regain function. Although she’dbegun walking at 9 months old, she lost that function asa result of surgery and had to start over. It took a full yearof rehabilitation before she could stand by herself again.She had seven rounds of inpatient chemotherapyas part of a clinical trial. The last three rounds includedhigh-dose stem cell chemotherapy (autologous bonemarrow transplant). One of the chemotherapy drugsaffected her hearing and required her to be fitted withtwo hearing aids.When she was 18 months old, Addyson had protonbeam therapy in Houston. (Mayo Clinic’s Proton BeamTherapy Program opened in 2015.) A scan after thetreatment concluded showed the cancer was no longerin Addy’s spinal fluid.“When Addy finished treatment, Dr. Rao said, ‘She’sdoing well. It’s time to go live your life,’” says Zidlicky.“We’re living life now and just want to enjoy Addy andexperience things she hasn’t experienced. The furtherwe get from cancer, the better the chances are. We knowAddy can get her cancer back or secondary cancer, butwe take it a day at a time and live it to the fullest.“Mayo Clinic saved her life. They’re like ourfamily. It’s obvious they support us and want ourdaughter to succeed.”Dr. Nageswara Rao says Addy’s survival may be dueto several factors — her Mayo team’s evolving expertisein brain tumors, her participation in a clinical trial andher own good fortune in overcoming many obstacles.Preschooler Addy can’t grasp with her right hand andwears an ankle brace for support. Despite these challenges,Zidlicky describes her daughter as a social butterfly.That’s music to Dr. Nageswara Rao’s ears. “This workhas changed my attitude about life. The things that werebig no longer are. I focus on how happy the child is today.“I get a lot from these patients. They face challengesa regular child doesn’t go through. I see familiesreprioritize their lives. I see them laugh and play. Theirbattles are much greater than mine. I feel privileged andlucky to be on their journeys.”Nathan Cordes and Michele Zidlickyof Wanamingo, Minnesota, aregrateful to Mayo Clinic for daughterAddyson’s brain tumor care.14MAYO CLINIC ALUMNI
Phase I clinical trial inpediatric cancer focuseson virus-based therapyMayo Clinic has begun a new phase Iclinical trial in pediatric cancer, and itfocuses on a virus-based therapy.The trial is testing th
The Mayo Clinic Cancer Center has grown and matured in many . ways since Dr. Moertel wrote his report. In 1977 Mayo Clinic saw 21,000 cancer patients. In 2013 we saw 122,000 cancer patients at Mayo Clinic. In 1977, 196 Mayo Clinic staff had a "major or total commitment to cancer." Today more than 1,100 Mayo Clinic physicians,