Transcription
NEW DELIVER Y MODELSAligning Care Delivery toEmerging Payment ModelsBoards can employ a “maturity framework”to help their organizations evolveBY THE AMERICAN HOSPITAL ASSOCIATIONHEditor’s note: Excerpted from “Evolving Care Models,” a Market Insights report fromthe AHA Center for Health Innovation that provides an overview of the successes andchallenges providers have experienced in aligning care delivery models with alternative payment models, and that provides lessons for those in the midst of this transition.As payers shift financial risk to providers through more advanced payment models,trustees will need to help their organizations build new capabilities for succeedingunder these payment arrangements. 2019 American Hospital Associationospitals and health systemsacross the country areredesigning care deliveryto improve quality and outcomes,enhance the patient experience,reduce costs and, ultimately,produce better population health.They are testing and implementingnew care models to focus onprevention and better coordinatecare across the many sites of carethat touch patients.The payment landscape forhealth care services has evolvedto support providers’ transition tonew care delivery models. Overthe past 10 years, payers havetransitioned a growing portion ofpayments made to providers fromtraditional fee-for-service to alternative payment models (APMs). Also,commonly referred to as valuebased payment models, APMsincent providers for quality andvalue, rather than volume.The AHA Center for HealthInnovation based this report on information and insights from a numberof sources, including interviews withhospital and health system leadersand other health care experts,surveys of hospitals and healthsystems, and a number of healthcare reports and research articles.www.aha.org October 2019 1
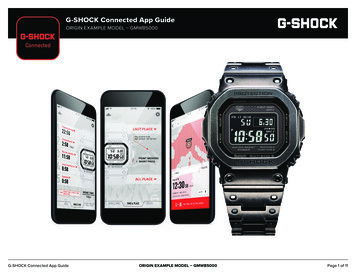
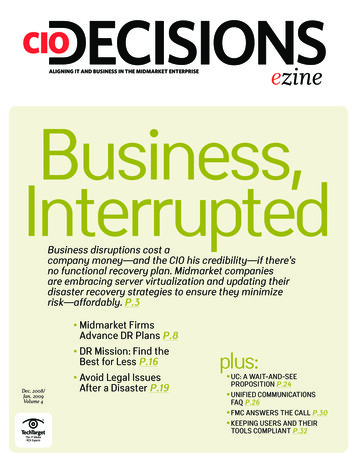
NEW D ELIVERY MO D ELSEvolution in Care Delivery ModelsAmong other key points, the report’s collaboratorshave observed that: APMs vary in the degree of financial riskthey transfer to providers, but most providerstoday still assume relatively low levels of risk. Thisapproach provides stability to providers as theybuild up the required capabilities for taking onhigher levels of risk. APMs have gained traction in recent years,driven in large part by government payers. Activityacross commercial payers varies geographicallybut is also accelerating. In certain cases, publicand private payers are working together — atboth the national and state levels — to alignpayment models. Providers are juggling the challenge ofdeveloping the capacity to operate successfullyin shared-risk payment models, while still caringfor significant numbers of patients in fee-for-service arrangements. 2019 American Hospital AssociationFour Most Common Alternative CareDelivery ModelsVarious service-delivery and payment modelsthat aim to achieve better care for patients,smarter spending and healthier communities arestill evolving and being tested. Health systemsare implementing and refining a wide array ofcare delivery models. Alternative approacheshave clustered around four specific models:accountable care organizations (ACOs), medicalhomes, integrated service lines (bundledpayment programs) and provider-sponsoredhealth plans, see chart on page 3.According to the report, health systems withoutprevious experience in alternative care deliverymodels chose to adopt one of the most commoncare models for the first time, and those withexperience were adopting new processes and/ortechnologies to make the models more effective.www.aha.org October 2019 2
NEW D ELIVERY MO D ELS8The Four Most Common Alternative Care Delivery ModelsEach model — while not exhaustive — represents the most common alternative care delivery frameworks in the field and observed in the literature. Eachmodel includes a real-world example and emerging insights.1ACCOUNTABLE CAREORGANIZATIONNetworks of health care providers jointly responsible for improving patient outcomes and reducingspending for an attributed patient population. Mayinvolve a range of provider configurations, such asphysician groups, behavioral health organizations,hospitals and health systems.DESCRIPTION: Caravan Health works with rural and independent health systems to build ACOsunder the MSSP.KEY INSIGHTS: After reviewing several yearsof MSSP data, Caravan recognized a critical challenge: ACOs in a shared savings/shared risk modelneed sufficient scale to minimize random spendingfluctuations in their attributed population. In 2019,the organization launched a national virtual Medicare ACO to aggregate attributed Medicare livesacross rural health systems. While many individual rural ACOs had between 5,000 and 10,000 lives,the new ACO has 225,000. Caravan has set up caremodel requirements participants must adopt, an intensive training program to help health systems buildnecessary capacity, and a robust data analytics platform in which participants can compare their performance against regional partners and the nationalACO. Caravan ultimately shares savings back withACO participants based on a methodology that includes patient attribution and quality performance.Such an approach offers a way for smaller, rural providers to attain the scale needed to perform wellunder APMs. As Lynn Barr, Caravan’s CEO, says, thegoal is to “standardize an effective model that willget results and create a platform for change.”RESULTS: Caravan’s national rural ACO is in itsfirst year. However, other Caravan-affiliated ACOsto date have substantially improved their qualityscores compared with baseline and generated savings more than 60 percent higher than the nationalaverage for MSSP ACOs. 2019 American Hospital Association2MEDICALHOMEModel of reorganizing primary care delivery. Under amedical home, an integrated care team — often encompassing a primary care provider, nurses, care managersand others — provides patients with whole-person,coordinated and accessible care. Some organizations pursue accreditation by an outside body (e.g., National Committee for Quality Assurance (NCQA) patient-centered,medical home certification), while others incorporate keyfeatures of the model without formal accreditation.DESCRIPTION: Summa Health in northeast Ohioprovides an integrated, team-based approach to primary care based on the principle “tasks for staff, decisions for physicians.” Primary care physicians focuson difficult diagnostic dilemmas and building relationships with patients, while nurses, pharmacists andother team members take on clinical and administrative functions of the medical home model directed toward helping patients achieve better health outcomes.KEY INSIGHTS: James Dom Dera, M.D., SummaHealth’s patient-centered medical home (PCMH) director, points to substantial evidence that robust primarycare is the key to better population health and lowertotal cost of care, and believes primary care spending will represent a larger percentage of total healthspending in the future. The best primary care deliveryapproaches, Dom Dera says, will build on the medical home model and incorporate increased virtual visits, patient education and links to social determinantsof health. Dom Dera believes population-based payments can best finance such an approach; however, incentives must be aligned across primary and specialtycare providers for the model to work effectively.RESULTS: Due to improved care transitions, Summa Health’s 2017 30-day readmission rate dropped tothe lowest level in seven years. Additionally, 77 percent of Summa’s primary care practices are PCMH-certified by NCQA, a large increase from the prior year.3INTEGRATEDSERVICE LINESHospitals and health systems are organizedaround integrated service lines — basedon specific disease states and/or careepisodes (e.g., cancer, heart and vascular,neuroscience, etc.) — across medicalspecialties and the continuum of care. Theapproach differs from a traditional hospitalorganizational structure organized by medical discipline (e.g., surgery, radiology, etc.).Integrated service lines are well positionedto negotiate bundled payments with payersfor specific episodes of care.DESCRIPTION: Mount Sinai HealthSystem (MSHS) in New York has offered ajoint replacement, bundled payment program to patients with certain commercialinsurance since 2016. Under the model, acare guide visits patients in the hospital,coordinates the transition home, manages outpatient and home-based, post-surgical care and arranges transportation to appointments.KEY INSIGHTS: Niyum Gandhi, chiefpopulation officer at MSHS, says the approach requires a different mindset. “Thisisn’t just a joint replacement program, it’sa mobility program. Specifically, the program’s ultimate goal isn’t the surgery —the goal is pain-free walking, and there’smore to that outcome than just the surgicalprocedure.”RESULTS: Since the start of the program, the percentage of program participants using the emergency departmentduring the episode of care dropped from 26percent to 3 percent.4PROVIDER-SPONSOREDHEALTH PLANSHealth plans that are financially sponsored oracquired by hospitals, physician groups or healthsystems. Providers often take responsibility fortotal cost of care for the health plan’s enrollees andaccept some degree of financial risk from the plan.While the health plan receives a capitated paymentfor its enrolled population, it does not always payproviders on a capitated basis.DESCRIPTION: Sharp HealthCare is an integrateddelivery system in San Diego County that includesa provider-sponsored health plan. Sharp offers arobust, continuum-based care management program.The system receives approximately 30 percent of itsrevenue on a capitated basis (a significant portioncomes from its health plan). Sharp is affiliated with afoundation-model medical group (Sharp Rees-SteelyMedical Group) and an aligned independent practiceassociation (Sharp Community Medical Group), andalso works with a large number of independentphysicians.KEY INSIGHTS: Executive Vice President DanGross says adapting care management programs tomeet the needs of individuals with specific chronicdiseases is critical to effectively managing populationhealth. One of the biggest challenges, Gross says,is aligning physician compensation with the healthsystem’s payer contracts, especially given varyingdegrees of physician affiliation with the system.RESULTS: The system receives consistentlyhigh ratings and awards on quality, efficiency andpatient-centered care, including awards from theLeapfrog group and Planetree. Sharp’s health plan isalso the highest member-rated health plan in California and has an NCQA accreditation of excellent.LEARN MORE Visit AHA.org/centerwww.aha.org October 2019 3
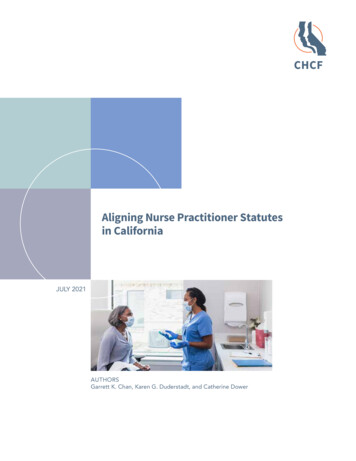
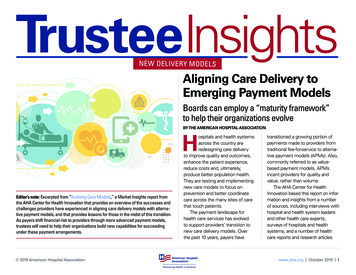
NEW D ELIVERY MO D ELSMaturity Framework for APMsWhile government payers have sparked a paradigm shift during the past decade around how topay for health care, they have allowed for a transition, granting providers time to build new capabilities without significant exposure to downsiderisk. Many health systems now find themselveswith one foot in more traditional fee-for-servicepayment systems and the other in alternativereimbursement models. They want to transformtheir care models, but struggle to finance therequired changes to their networks, processesand support systems. 2019 American Hospital AssociationBoards can help their organizations evolvetoward value-based payment models byemploying a “maturity framework” in discussionswith their leadership team, see pages 5-6.Each organization can use the maturity framework to assess its current capabilities to determine the best type of value-based care for theorganization. All providers need to rethink wherethey are on the risk continuum, where they willbe in the future and whether they have the infrastructure systems needed to manage risk.www.aha.org October 2019 4
NEW D ELIVERY MO D ELS12Maturity Framework for New Care Models/Risk-sharing ArrangementsHospitals are in the midst of navigating significant changes in how they operate and deliver care. Each organization can use the maturity framework to assess itscurrent capabilities to determine the best type of value-based care for the organization. All providers need to rethink where they are on the risk continuum, wherethey will be in the future and whether they have the infrastructure systems needed to manage risk.M AT U R I T Y L E V E LCAPABILITYBASIC NETWORK Significant gaps in assetsCare Continuumand ProviderNetworkManagementacross care continuum (outpatient —inpatient — post-acute) AFFILIATION REQUIREMENTS Limited criteriafor affiliation QUALITY IMPROVEMENTS No link to quality/value CLINICAL PROTOCOLS No standardization ofclinical protocols CARE MANAGEMENT Limited, if any QUALITY IMPROVEMENTS Quality-imClinical and CareManagementprovement and disease-managementprograms exist but are not coordinatedacross different parts of the healthsystem ELECTRONIC HEALTH RECORD Functional EHRbut little interoperability with affiliates POPULATION HEALTH MANAGEMENT TOOLS Use of disease registries/reportingIT Infrastructureand Analytics 2019 American Hospital Association PERFORMANCE ANALYTICS Some ability totrack performance against quality/utilization benchmarksFOUNDATIONAL NETWORK Robust network (either ownedor affiliated). Health systems can addressmost patient care needs across continuum through owned or affiliated providers. AFFILIATION REQUIREMENTS Contractsrequire commitment to shared quality/utilization metrics QUALITY IMPROVEMENTS Portion of payment to physicians tied to performance/valueADVANCED NETWORK Comprehensive, clinically integrated network AFFILIATION REQUIREMENTS Affiliation rela-tionship contingent on meeting quality andcost-management objectives QUALITY IMPROVEMENTS Strong alignment ofphysician compensation with clinical objectives through use of incentives CLINICAL PROTOCOLS Shared clinical proto- CLINICAL PROTOCOLS Process for updating ELECTRONIC HEALTH RECORD Strategy in ELECTRONIC HEALTH RECORD Common EHR,cols and standards of care CARE MANAGEMENT Integrated care teams,including nonphysician providers; dedicated care managers for high-risk patients QUALITY IMPROVEMENTS Shared qualitymeasuresplace to integrate EHR and analyticsplatforms across network, though notnecessarily common platform POPULATION HEALTH MANAGEMENT TOOLS Population health-management system toidentify high-risk patients PERFORMANCE ANALYTICS Integration ofclinical, administrative and care management data at patient-level; practice-leveldashboards to track performance againstquality/utilization targetsprotocols with latest evidence and monitoring adoption CARE MANAGEMENT Population-health anddisease-management programs, includinguse of telehealth and new technologies,where appropriate; assessment of socialdeterminants of health and referrals to community-based organizations QUALITY IMPROVEMENTS Culture of continuousprocess improvement with progressivelyevolving performance standardsanalytics and care management platformused across network POPULATION HEALTH MANAGEMENT TOOLS Ability to identify defined subpopulationsfor targeted interventions; use of predictivemodeling to identify at-risk members; abilityto facilitate and track closed-loop referrals tocommunity-based organizations PERFORMANCE ANALYTICS Near real-time visibility into quality and cost performanceContinuedpage( Continuedonon page136)LEARN MORE Visit AHA.org/centerwww.aha.org October 2019 5
13NEW D ELIVERY MO D ELSMaturity Framework for New Care Models/Risk-sharing Arrangements (continued)M AT U R I T Y L E V E LCAPABILITYBASIC PRACTICE MANAGEMENT AND REVENUE-CYCLE MANAGEMENT Systems in placeACTUARIAL/RISK-MANAGEMENT CAPABILITIES Limited to non existent PRACTICE MANAGEMENT AND REVENUE-CYCLEMANAGEMENT Evolving to address evolv-ing reimbursement models ACTUARIAL/RISK-MANAGEMENT CAPABILITIES Ability to negotiate and manage performance for contracts with downside risk;some risk mitigation in placeFinancialManagement GOVERNANCE STRUCTURE Informal OPERATING UNITS No change PROVIDER ENGAGEMENT Limited providerengagement in development of qualityimprovement programsGovernanceand ProviderEngagementFOUNDATIONAL GOVERNANCE STRUCTURE Structure in placeto oversee APMs OPERATING UNITS New functions createdto support contract management withpayers and provider partners PROVIDER ENGAGEMENT Clinical and administrative leadership buy-in to supportalternative payment/care delivery; workforce-development strategy in place tosupport transition; change-managementstrategy to guide organizational transformationADVANCED PRACTICE MANAGEMENT AND REVENUE-CYCLEMANAGEMENT Systems fully aligned withreimbursement models ACTUARIAL/RISK-MANAGEMENT CAPABILITIES Forprovider-sponsored health plans, ability toperform claims payment, underwriting andmeet reserve requirements GOVERNANCE STRUCTURE Corporate gover-nance with clear roles for board, executiveteam, medical staff leaders with regard toclinical direction, state regulatory reporting,compliance, management and operations OPERATING UNITS Organizational modelaligned with new care delivery and reimbursement models PROVIDER ENGAGEMENT Providers well integrated into strategic planning efforts“Reformed paymentmechanisms will onlybe as successful as thedelivery system capabilities and innovationsthey support.” 2019 American Hospital AssociationLEARN MORE Visit AHA.org/centerwww.aha.org October 2019 6
NEW D ELIVERY MO D ELSRoad Map to Advance Along the Maturity ModelHealth system leaders who have embarked oncare delivery change say they are committed tocontinuing the evolution toward value-based carebecause the approach is better for patients, butthey caution that there is no silver bullet that cansubstitute for: setting an inspiring vision for caredelivery; engaging clinicians to agree on evidence- 2019 American Hospital Associationbased protocols and care plans; retraining staff tosupport the new approach; and building feedbackloops to measure organizational performance andadjust accordingly.The following “road map” on page 8 offers leadership lessons for those wishing to transform theircare models.www.aha.org October 2019 7
1414NEW D ELIVERY MO D ELSRoad Map to Advance Along the Maturity ModelRoad Map to Advance Along the Maturity ModelThe experiences of these and other provider organizations offer a road map for others seeking to accelerate their transition to greater levels of risk.The experiences of these and other provider organizations offer a road map for others seeking to accelerate their transition to greater levels of risk.11Develop andcommit to aDevelop andtransformedcommitavisionof caretodelivery,transformedrecognizingthat the newvision ofcareapproachmayrisk delivery,short-termrecognizingthat butthe willnewdrivefinanciallosses,approach mayrisk t will driveon cess.health systemson interviewsconductedthatimplementednew forthis report,systemscaredeliveryhealthmodelssawthat implementednewbetterhealth sandbetterengagedhealth outcomes,moreproviders.moresatisfied andpatientsandAsconsumerspayersmore engagedcometo expectproviders.greater valueAs consumerspayersfromproviders and— includingcometo expectgreater avaluehigh-qualityoutcomes,pafrom providers approach— includingtient-centeredandhigh-qualityoutcomes,a pamultiplepathwaysto accesstient-centeredapproachandcare(e.g., in person,virtualmultipleaccesscare,etc.)pathways— healthtosystemscare(e.g., in person,virtualandthat developsuch a visioncare, etc.)— healthremainsteadfastwillsystemsbe wellthat developforsucha visionsucandpositionedlong-termremainsteadfastbe wellcessdespiteinitialwillchallengespositionedfor newlong-termsuctofinance lscatchup.to finance the new system aspayment models catch up.22Identify a source offinancing for the careIdentify atransformation.source ofdeliveryfor the careBuildingfinancingnetworks, ation.and investing ngrequire capital.deliveryprocessesand investinginSome providersin moremature marsupportcapital.ketsmaysystemsbe ableallto requirequickly negotiateSome providersin morematuremarrisk-basedcontractsacrossmultiplekets mayable toquicklypayersto befinancetheircare mayacrossneed tomultiplefocuspayersto financetheir (e.g.,care deliveryon a handfulof payersMSSP,changes. Othersmay needto focusMedicareAdvantage,one commeron acontract,handful ofpayers(e.g., MSSP,tocialetc.)or funding onefor caredeliverycial contract, althprovideforupfrontcare repaid”sharedsystems inmightnegotiateupfrontcareupsavings,whichthey receivefundsmanagementor “prepaid”frontthat are feesdiscountedagainstsharedanysavings,generated.in which they receive funds upsavingsfront that are discounted against anysavings generated.44Build financialmanagementBuild financialcapabilitiestomanagementmanagerisk contracts.capabilitiesto theAs providersadvance alongmanagerisktheycontracts.risk spectrum,will needAs providersadvance alongtheadditionalcapabilitiesto manrisk spectrum,they payers.will needagecontracts withThisadditionalis capabilitiesto manfunctioncritical to translatingage contractswith payers.caredelivery innovationintoThisfunctionsuccess. is critical to translatingcare delivery innovation intosuccess.5533Develop a proofof concept.Develop changesa proofImplementconcept.and testofthemodel, dqualitytest thecarefullytoandmodel,cost forthetrackingrelevant outcomespopulation.relatedto quality and cost for therelevant population.66Leverage theproof of conceptLeveragethemoretonegotiateproofAPMsof rethanadvancedAPMswithwaitingfor payersto rswaitingpayersto evolveusetheirforproofof concepttheirmodels, providerscantoproactivelybring a valueusetheir proofof conceptpropositionto payers.to proactively bring a valueproposition to payers.Align physicianincentives withAlign ybroaderAPMsers. Providersinterviewednegotiatedwith payfor this report nwhenfor thissystemsreport identifiedhealthimplementan inherenttensionwhenAPMsdesignedto reducehealth to reducewhile edphysicianswhile payingemployedbasedon volume(e.g., iderbased on volumeorganizationscan(e.g.,workrelcolativevalue units).Providerlaborativelywith physiciansorganizationscanwork coltodevelop newcompensalaborativelyphysicianstionmodels with— generallyto develop newcompensaincorporatinga lity, andincorporatinga basea smaller portiontiedsalary,to vola portiontiedalignto quality,andume— thatphysiciana smaller portiontied to volincentiveswith APMs.ume — that align physicianincentives with APMs.LEARN MORE Visit AHA.org/centerLEARN MORE Visit AHA.org/center 2019 American Hospital Associationwww.aha.org October 2019 8
NEW D ELIVERY MO D ELSConclusionBy building care delivery prototypes, testingtheir models and bringing a value propositionto payers, health systems can achieve greateralignment among reimbursement from government and commercial payers, thereby furtheraccelerating care delivery transformation. Suchan approach creates a virtuous cycle where initialsuccesses in care delivery and payment reformprovide feedback to drive bolder care modelchanges and increased levels of financial risk. Aspayers continue to shift higher levels of risk ontoQuestions for Board Discussionproviders, hospitals and health systems that canleverage this positive feedback loop to transitiona substantial portion of their payment streamto APMs will be well positioned for success.Through the hard work of changing their caremodels, providers are poised to lead care deliverychange to improve patient outcomes.The report was collaboratively prepared withinsights from Benjamin Chu, Naomi Newman andAvi Herring from Manatt Health.1. How has our organization gained experience with alternative care delivery/paymentmodels? Which models have we adoptedand what have we learned?2. W hat are the key challenges we havefaced in gaining experience with new caredelivery/payment models (for example,engaging staff and clinicians, financing thetransition to these models, acquiring thetechnology, tools and capabilities neededto make the change, etc.)? How has ourorganization addressed these challenges?3. W ill experience with alternate care deliveryand payment models require us to changeour risk appetite/tolerance and, if so, how?4. W here does our organization fall on eachdimension of the maturity framework shownabove?5. W hat steps along the above road mapmight our organization take to continueto advance our capabilities to effectivelyengage in value-based care delivery andpayment?6. H ow should our board continue to monitorour organization’s progress toward adoptingvalue-based care and payment models? 2019 American Hospital Associationwww.aha.org October 2019 9
The Four Most Common Alternative Care Delivery Models Each model — while not exhaustive — represents the most common alternative care delivery frameworks in the field and observed in the literature. Each model includes a real-world example and emerging insights. 1 ACCOUNTABLE CARE ORGANIZATION Networks of health care providers jointly respon-