Transcription
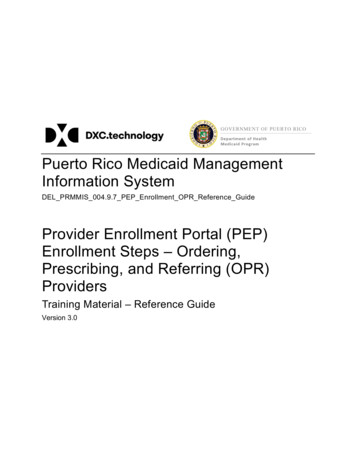
VERMONT MEDICAID PROVIDER ENROLLMENT & REVALIDATION FORMNon-Billing Providers - Ordering, Prescribing, Referring & Attending (OPRA) Providers and ResidentsCompletion of this form is limited to providers seeking non-billing enrollment privileges as an ordering, prescribing, referring, or attending providerand residents.The Affordable Care Act (ACA) requires that physicians or other eligible providers enroll in Medicaid to order, prescribe, refer or attend items orservices for Medicaid beneficiaries, even when they do not submit claims to Medicaid. The Provider Enrollment and Revalidation Form for OPRAProviders is an abbreviated enrollment form for those OPRA providers that do not intend to submit claims.Enrolling ensures that physicians, other practitioners and facilities that provide services and bill based on your order referral, or prescription, will bepaid for such items or services.Enrolling in Vermont Medicaid as an OPRA Provider or Resident: Does not obligate you to see Medicaid patients; Does not mean you will be listed as a Medicaid provider for patient assignment or referral; Helps ensure that your orders, prescriptions and referrals for Medicaid patients are accepted and processed appropriately.Providers who complete this application are not eligible for reimbursement. The facility or group must be enrolled to receive payment.Please refer to the Green Mountain Care Instructions for Enrollment and Revalidation for instructions.All *asterisked sections must be completed.1. *Type of RequestNew Enrollment Request (Enrollment limited to ordering, prescribing, referring or attending privileges and residents; non-billing practitioners)Revalidation Request (existing ordering, prescribing, referring and attending — not billing; required to revalidate)(If Revalidation Request) Provider Number Indicated on Notification Letter:Specify Practitioner Type (select all that nt2. *Provider/Applicant InformationApplicant Name (please format LAST, FIRST MI, Title)Provider Name:Street:City: State: Zip Code:Other Name (former, maiden, professional) Last, First, MI:Email Address:DOB (mm/dd/yyyy):Medicare Enrolled?:YesSSN:NoAre you enrolled in other state Medicaid Program?:FEIN:If Yes, Medicare Number:YesNoIf Yes, what state(s):NPI (Individual): Taxonomy Number(s):*Group or Facility Name:If group or facility affiliated, Group or Facility NPI:Driver’s license or other state issued identification number: Gender (M/F):DEA Number: Expiration Date (mm/dd/yyyy):DEAX Number: Expiration Date (mm/dd/yyyy):CLIA Number: Issue Date (mm/dd/yyyy):0120221
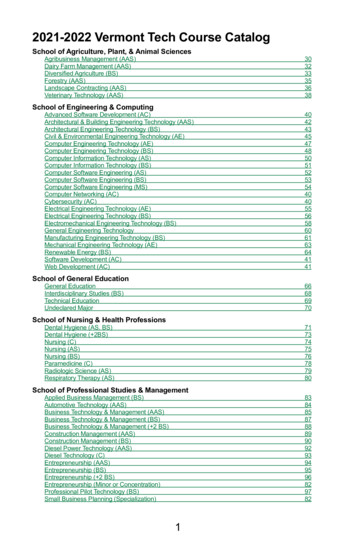
3. *Licensing Information (list all current licenses held, attach additional sheets as needed)License/Certification #: State Issued: Date of Expiration:License/Certification #: State Issued: Date of Expiration:License/Certification #: State Issued: Date of Expiration:4. Medical/Dental/Clinical Specialties **** The following health care professionals are required to complete this section at time of application: physicians, nurse practitioners, dentists,doctoral-level psychologists & social workers and individual DME providers (includes prosthetics).Specialty: End Date: Board Certified (Yes or No):Specialty: End Date: Board Certified (Yes or No):Specialty: End Date: Board Certified (Yes or No):5. *Proof of Professional Liability InsuranceProof of Professional Liability Insurance – attach a copy of the face page of Malpractice CertificateName of Insurance Company:Street:City: State: Zip code:Telephone: Email:Insurance Policy #: Date Issued (mm/dd/yyyy): Expiration Date (mm/dd/yyyy):6. Hospital PrivilegesDo you have hospital privileges:YesNoIf No, please explain why:If Yes, provide the following hospital information (attach additional sheets, as needed)Name of Hospital: NPI #:Street:City: State: Zip code:Telephone Number: Email:Name of Hospital: NPI #:Street:City: State: Zip code:Telephone Number: Email:Name of Hospital: NPI #:Street:City: State: Zip code:Telephone Number: Email:0120222
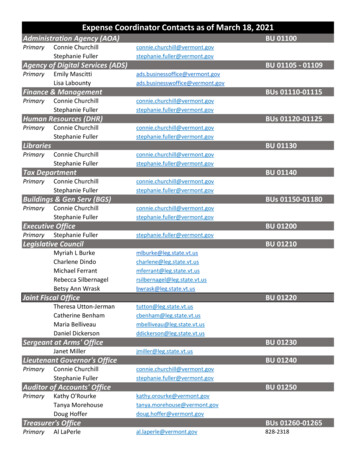
7. *Applicant/Provider Address InformationMail to Address(correspondence & newsletters)Street: Suite #:City: State: Zip Code:Telephone number: Fax:Email:Service Address(physical address only - PO boxes not accepted)Street: Suite #:City: State: Zip Code:Telephone number: Fax:Email:Handicap AccessibilityNonePartial (At least one building, office and examining room are accessible)Totally AccessibleAlternate Methods of Access: The provider’s office is not accessible, but he or she will see patient at analternate site that is accessible.Languages Accommodated:EnglishOther (specify all):Patient Age LimitsAll agesNewbornAge range only (Youngest) (Oldest)(Age range of patients that you will see; not the age range of your current patients).Established Patients OnlyYes(If not accepting new patients check “Yes”;If accepting new patients check “No”)8.No*Conviction/Sanction/Disclosure and Suspension/Debarment Information“Sanction” is defined as recoupment, payment hold, imposition of penalties or damages, contract cancellations, exclusion,debarment, suspension, revocation, or any other synonymous action.Have you ever been sanctioned (as defined above) in any state or federal program?YesNoIf Yes, fully explain the details, include any applicable documentationIs your professional license or certification currently revoked, suspended or otherwise restricted?YesHave you ever had your professional license or certification revoked, suspended, or otherwise restricted?Are you currently, or have you ever been, subject to a licensing or certification board order?YesHave you voluntarily surrendered your professional license or certification in lieu of disciplinary action?Do you have any outstanding debt in relation to any other state’s federally funded program?YesNoYesNoNoYesNoNo(You are subject to a license or certification verification/status check with your licensing or certification board.)If Yes was answered to any of the above questions, fully explain details, include any applicable documentation (attach additional sheets as needed):0120223
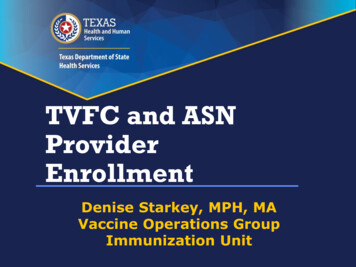
8.*Conviction/Sanction/Disclosure and Suspension/Debarment Information (Continued)“Convicted” means that:(a) A judgment of conviction has been entered against an individual or entity by a federal, state or local court, regardless of whether:(1) There is a post-trial motion or an appeal pending, or(2) The judgment of conviction or other record relating to the criminal conduct has been expunged or otherwise removed;(b) A Federal, State or local court has made a finding of guilt against an individual or entity;(c) A Federal, State or local court has accepted a plea of guilty or nolo contendere by an individual or entity, or(d) An individual or entity has entered into participation in a first offender, deferred adjudication or other program or arrangement where judgment ofconviction has been withheld.Are you currently charged with or have you ever been convicted of a crime (excluding Class C misdemeanor traffic citations)?YesNoTo answer this question, use the federal Medicaid/Medicare definition of “Convicted” in 42 CFR. § 1001.2 as described above, andwhich includes deferred adjudications and all other types of pretrial diversion programs. Providers are screened per requirements of 42 CFR 4554.434.Have you been arrested for a crime but not yet charged?Is there an outstanding warrant for your arrest?YesYesNoNoIf Yes was answered to any of the above questions, fully explain details, please include supporting documentation (attach additional sheets as needed):In accordance with 32 VSA §3113(b), I declare, under the pains and penalties of perjury, that I am in good standing with respect to (or in fullcompliance with a plan to pay) any and all taxes due.YesNoIf No, supply explanation:Within ten years of the date of this statement, has the entity or person been convicted of any felony or misdemeanor involving fraud or abuse in anygovernment program?YesNoIf Yes, provide the date of the conviction and explain details (mm/dd/yyyy):Within ten years of the date of this statement, has the entity or person been found liable for fraud or abuse involving a governmentprogram in any civil proceeding?YesNoIf Yes, provide the date of the conviction and explain details (mm/dd/yyyy):Within ten years of the date of this statement, has the entity or person entered into a settlement in lieu of conviction for fraud or abuse involving agovernment program?YesNoYes, provide the date of the settlement and explain details (mm/dd/yyyy):Does the entity or person currently participate or have they ever participated, as a provider in the Vermont Medicaid program or in another state’sMedicaid program?YesNoIf Yes, State: Name(s) (Legal & DBA):NPI and/or Provider Number(s):0120224
9. *Contact InformationPlease provide the name and contact information of the individual to contact regarding to this form.Name: Title:Phone #:Fax:Email:10. Backdating Enrollment Start DateFor New or Reenrolling providers ONLY. If you wish to have your effective date backdated, up to a year from the date of receipt of acompleted application, please indicate below the date requested and rationale. Backdates will only be approved if confirmation canbe obtained that screening requirements are meet, as of requested effective date, under 42 CFR §§455.410 and §455.450. (Currentlyenrolled providers, please use Enrollment backdate form.) Attachments accepted.Effective Date Backdate:Office Use OnlyPECOS Effective Date End Date11. *Declaration & SignatureI have read the contents of this application. I declare under penalty of perjury under the laws of the State of Vermont that the information in thisapplication and any attachments are true, accurate and complete to the best of my knowledge and belief. My signature legally and financiallybinds this provider to the laws, regulations, and program instructions of the Vermont Medicaid program and state/federal assisted healthcareprograms. I declare that I have the authority to legally bind the provider(s) listed or I am the provider on this Application.If I become aware that any information in this application is not true, correct or complete, I agree to notify HP Enterprise Services of this factimmediately (within 30 days of change) at 800.925.1706.Individual Practitioner First Name:Authorized Signature or Practitioner Signature:Middle:Individual Last Name:Jr., Sr, M.D., D.O. etc.:Date:Title of Authorized Signature:All signatures must be original and signed in blue ink. Applications with signatures deemed not original will not beprocessed. Stamped, faxed or copied signatures are not accepted.STOP!As a reminder, the following is required to accompany this application for it to be considered complete. Failure toinclude the following will result in a returned application and a delay in your enrollment or revalidation.1. All pages of the Provider General Agreement must be returned with this application, to include the last page withan original signature.2. Proof of Professional Liability Insurance - attach a copy of the face page of Current Malpractice Certificate3. If you are one of the following provider types, you are required to complete Section 4: physicians, nursepractitioners, dentists, doctoral-level psychologists & social workers and individual DME providers (includesprosthetics). If your provider type is listed above and you do not complete the section, your application will beconsidered incomplete and your application will be return.0120225
4. New and Re-Enrollment effective dates are based on the day the complete packet is received by Gainwell. If youwish your effective date to be up to a year earlier and you are Medicare enrolled, please complete section 10 of thisapplication. For requests that are older than a year or for non-Medicare enrolled providers, please complete theEnrollment Backdate Form located here: http://www.vtmedicaid.com/#/provEnrollDataMaint. If, upon verificationof Medicare enrollment, we find your Medicare enrollment has lapsed, your effective will be the date of receipt ofyour complete application, not your requested effective date.If the enrollment application is not complete upon receipt by Gainwell, it will be returned to the provider.Return all completed forms to:Gainwell Technologies, Attn: Enrollment Unit , P.O. BOX 888, Williston, VT 05495If confirmation of delivery is requested, please return to:Gainwell Technologies, 28 Walnut Street, Suite 245 Building CMaple Tree Place Shopping Center, Williston, VT 054950120226
Individual Practitioner First Name: Middle: Individual Last Name: Jr., Sr, M.D., D.O. etc.: Authorized Signature or Practitioner Signature: Date: Title of Authorized Signature: 10. ackdating Enrollment Start Date For New or Reenrolling providers ONLY. If you wish to have your effective date backdated, up to a year from the date of receipt of a