Transcription
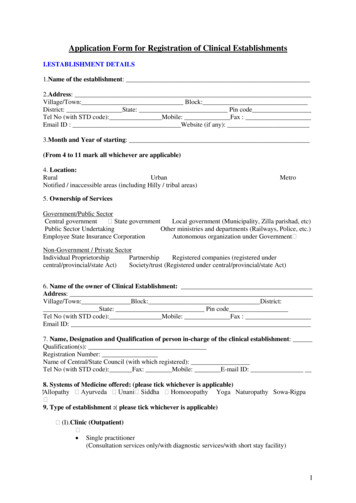
Application Form for Registration of Clinical EstablishmentsI.ESTABLISHMENT DETAILS1.Name of the establishment:2.Address:Village/Town: Block:District: State: Pin codeTel No (with STD code): Mobile: Fax :Email ID : Website (if any):3.Month and Year of starting:(From 4 to 11 mark all whichever are applicable)4. Location:RuralUrbanNotified / inaccessible areas (including Hilly / tribal areas)Metro5. Ownership of ServicesGovernment/Public SectorCentral government State governmentLocal government (Municipality, Zilla parishad, etc)Public Sector UndertakingOther ministries and departments (Railways, Police, etc.)Employee State Insurance CorporationAutonomous organization under Government Non-Government / Private SectorIndividual ProprietorshipPartnershipRegistered companies (registered undercentral/provincial/state Act)Society/trust (Registered under central/provincial/state Act)6. Name of the owner of Clinical Establishment:Address:Village/Town: Block: District:State: Pin codeTel No (with STD code): Mobile: Fax :Email ID:7. Name, Designation and Qualification of person in-charge of the clinical establishment:Qualification(s):Registration Number:Name of Central/State Council (with which registered):Tel No (with STD code): Fax: Mobile: E-mail ID:8. Systems of Medicine offered: (please tick whichever is applicable) Allopathy Ayurveda Unani Siddha Homoeopathy Yoga Naturopathy Sowa-Rigpa 9. Type of establishment :( please tick whichever is applicable) (I).Clinic (Outpatient) Single practitioner(Consultation services only/with diagnostic services/with short stay facility)1
Poly clinic(Consultation services only/with diagnostic services/with short stay facility)DispensaryHealth Checkup Centre(II). Day Care facilityMedicalSurgicalMedical SPAWellness centers (where qualifiedmedical professionals are available to supervise the services).(III). Hospitals including Nursing Home (outpatient and inpatient): Hospital Level 1 a Hospital Level 1 b Hospital Level 2 Hospital Level 3 (Non teaching) Hospital Level 4 (Teaching)(IV). Dental Clinics and Dental Hospital:a. Dental clinicsi.ii.Single practitionerPoly Clinics (dental)b. Dental Hospitals (specialties as listed in the IDC Act.)i.ii.iii.iv.v.vi.vii.viii.ix.Oral and maxillofacial surgeryOral medicine and radiologyOrthodonticsConservative dentistry and EndodonticsPeriodonticsPedodontics and preventive dentistryOral pathology and MicrobiologyProsthodontics and crown bridgePublic health dentistry (V).Diagnostic Centre A. Medical Diagnostic Laboratories: Pathology BiochemistryMolecular Biology and Genetic LabsMicrobiologyVirology B. Diagnostic Imaging centersi.Radiology General radiologyInterventional radiologyii.Electromagnetic imaging Magnetic Resonance Imaging (MRI), Positron Emission Tomography (PET) Scaniii.Ultrasound C. Miscellaneous2
Electro Cardio Graphy(ECG) Tread Mill Test Electro Encephalo Graphy(EEG)Mammography Echocardiography Electro MyoGraphy (EMG) Electrophysiological studiesD. Collection centersFor the clinical labs and diagnostic centres shall function under registered clinicalestablishmentYes/Noif Yes, then No of Collection Centre:(VI). Allied Health professions: AudiologyBehavioral health (counseling, marriage and family therapy etc)Exercise physiologyNuclear medicine technologyMedical Laboratory ScientistDieteticsOccupational therapyOptometryOrthopticsOrthotics and prostheticsOsteopathyParamedicPodiatryHealth Psychology/ Clinical PsychologyPhysiotherapyRadiation therapyRadiography / Medical imagingRespiratory TherapySonographySpeech pathology(VII) AYUSHAyurvedaAusadh ChikitsaShalya ChikitsaPathya VyavasthaYogaAshtangShodhan ChikitsaRasayanaYogaUnaniMatab JarahatIlaj-bit-TadbeerSiddhaMaruthuvamSirappu MaruthuvamHifzan-e-SehatVarmam Thokknam & YogaHomoeopathyGeneral Homoeopathy3
NaturopathyExternal Therapies with natural modalitiesInternal TherapiesII.TYPES OF SERVICE TYPE General Practice ServicesSingle Specialty Services Multi Specialty Services (including Palliative care Centre, Trauma Centre, MaternityHome - applicable for hospitals only)Super Specialty Services SPECIALITY SPECIFICMedical Specialties – for which candidates must possess recognized PG degree(MD/Diploma/DNB or its equivalent xiv.xv.xvi.xvii.xviii.AnesthesiologyAviation MedicineCommunity MedicineDermatology, Venerology and LeprosyFamily MedicineGeneral MedicineGeriatricsImmunoHaematology and Blood TransfusionNuclear MedicinePaediatricsPhysical Medicine pyRheumatologySports MedicineTropical MedicineTuberculosis & Respiratory Medicine or Pulmonary MedicineSurgical specialties - for which candidates must possess, recognized PG degree(MS/Diploma/DNB or its equivalent degree)i.ii.iii.iv.v.OtorhinolaryngologyGeneral SurgeryOphthalmologyOrthopedicsObstetrics & GynecologyMedical Super specialties –i. Cardiologyii. Clinical Hematology including Stem Cell Therapyiii. Clinical Pharmacology4
gyMedical GastroenterologyMedical GeneticsMedical ogySurgical Super-specialitiesi.Cardiovascular thoracic Surgery)ii.Urologyiii.Neuro-Surgeryiv.Paediatrics Surgery.v.Plastic & Reconstructive Surgeryvi.Surgical Gastroenterologyvii.Surgical Oncologyviii.Endocrine Surgeryix.Gynecological Oncologyx.Vascular SurgeryIII INFRASTRUCTURE DETAILS10. Area of the establishment (in sqft):a) Total Area: b) Constructed area:11. Out Patient Department:11.1 Total no. of OPD Clinics:11.2 Specialty-wise distribution of OPD ClinicS.No.Specialty12. In Patient Department:12.1. Total number of beds:12.2. Specialty-wise distribution of beds, please specify:S.No.SpecialtyBeds13. Biomedical waste Management13.1Method of treatment and /or disposal of Bio-medical waste Through Common Facility Onsite Facility Any other (please specify):5
13.2.Whether authorization from Pollution Control Board/Pollution Control Committeeobtained? Yes No Applied For Not ApplicableIV HUMAN RESOURCES14. Total number of Staff (as on date of application):No. of permanent staff: No. of temporary staff:Please furnish the following details:Category of staffNameQualificationRegistration Nature of serviceNoTemporary/PermanentDoctorsNursing staffPara-medical staffPharmacistsAdministrative staffOthers, pleasespecifySeparate annexure may be attached.Support StaffCategoryTotal no.Remark15. Payment options for Registration Fees: Online payment Demand DraftBank Challan Amount (in Rs):Details:Receipt No.I,. on behalf of myself and the company/society/association/body hereby declare that the statements above are correct and true to the best ofmy knowledge and I shall abide by all the provisions made under the Clinical Establishment(Registration and Regulation) Act 2010.I undertake that I shall inform the DistrictRegistering Authority of any changes in the particularsgiven above.I shall comply with the minimum standards prescribed under Clinical Establishment Act for theservices provided by us and also all other conditions of registration as stipulated under the aforesaidAct and Rule there-under.Place:Date:Signature of the Authorized SignatoryOffice Seal6
11.2 Specialty-wise distribution of OPD Clinic S.No. Specialty 12. In Patient Department: 12.1. Total number of beds: _ 12.2. Specialty-wise distribution of beds, please specify: S.No. Specialty Beds 13. Biomedical waste Management 13.1 Method of treatment and /or disposal of Bio-medical waste