Transcription
ISSN 1007-9327 (print)ISSN 2219-2840 (online)World Journal ofGastroenterologyWorld J Gastroenterol 2018 April 14; 24(14): 1491-1582Published by Baishideng Publishing Group Inc
SContentsWeekly Volume 24 Number 14 April 14, 2018REVIEW1491Nonalcoholic fatty liver disease and liver transplantation - Where do we stand?Mikolasevic I, Filipec-Kanizaj T, Mijic M, Jakopcic I, Milic S, Hrstic I, Sobocan N, Stimac D, Burra P1507Hepatitis B virus pre-S/S variants in liver diseasesChen BFMINIREVIEWS1521Extra-intestinal manifestations of non-celiac gluten sensitivity: An expanding paradigmLosurdo G, Principi M, Iannone A, Amoruso A, Ierardi E, Di Leo A, Barone MORIGINAL ARTICLEBasic Study1531Punctual mutations in 23S rRNA gene of clarithromycin-resistant Helicobacter pylori in Colombian populationsMatta AJ, Zambrano DC, Pazos AJRetrospective Study1540Post-polypectomy bleeding and thromboembolism risks associated with warfarin vs direct oralanticoagulantsYanagisawa N, Nagata N, Watanabe K, Iida T, Hamada M, Kobayashi S, Shimbo T, Akiyama J, Uemura NRandomized Controlled Trial1550Maintenance for healed erosive esophagitis: Phase Ⅲ comparison of vonoprazan with lansoprazoleAshida K, Iwakiri K, Hiramatsu N, Sakurai Y, Hori T, Kudou K, Nishimura A, Umegaki EMETA-ANALYSIS1562Application of enhanced recovery after gastric cancer surgery: An updated meta-analysisWang LH, Zhu RF, Gao C, Wang SL, Shen LZLETTERS TO THE EDITOR1579Should hot biopsy forceps be abandoned for polypectomy of diminutive colorectal polyps?Panteris V, Vezakis A, Triantafillidis JKWJG www.wjgnet.com April 14, 2018 Volume 24 Issue 14
World Journal of GastroenterologyContentsVolume 24 Number 14 April 14, 2018ABOUT COVEREditorial board member of World Journal of Gastroenterology , Maria Gazouli,PhD, Associate Professor, Basic Medical Science, School of Medicine, Nationaland Kapodistrian University of Athens, Athens 11527, GreeceAIMS AND SCOPEWorld Journal of Gastroenterology (World J Gastroenterol, WJG, print ISSN 1007-9327, onlineISSN 2219-2840, DOI: 10.3748) is a peer-reviewed open access journal. WJG was established on October 1, 1995. It is published weekly on the 7th, 14th, 21st, and 28th each month.The WJG Editorial Board consists of 642 experts in gastroenterology and hepatology from59 countries.The primary task of WJG is to rapidly publish high-quality original articles, reviews,and commentaries in the fields of gastroenterology, hepatology, gastrointestinal endoscopy, gastrointestinal surgery, hepatobiliary surgery, gastrointestinal oncology, gastrointestinal radiation oncology, gastrointestinal imaging, gastrointestinal interventional therapy, gastrointestinal infectious diseases, gastrointestinal pharmacology, gastrointestinalpathophysiology, gastrointestinal pathology, evidence-based medicine in gastroenterology, pancreatology, gastrointestinal laboratory medicine, gastrointestinal molecular biology, gastrointestinal immunology, gastrointestinal microbiology, gastrointestinal genetics,gastrointestinal translational medicine, gastrointestinal diagnostics, and gastrointestinaltherapeutics. WJG is dedicated to become an influential and prestigious journal in gastroenterology and hepatology, to promote the development of above disciplines, and toimprove the diagnostic and therapeutic skill and expertise of clinicians.INDEXING/ABSTRACTINGWorld Journal of Gastroenterology (WJG) is now indexed in Current Contents /Clinical Medicine,Science Citation Index Expanded (also known as SciSearch ), Journal Citation Reports , IndexMedicus, MEDLINE, PubMed, PubMed Central and Directory of Open Access Journals. The2017 edition of Journal Citation Reports cites the 2016 impact factor for WJG as 3.365 (5-yearimpact factor: 3.176), ranking WJG as 29th among 79 journals in gastroenterology and hepatology (quartile in category Q2).EDITORS FORTHIS ISSUEResponsible Assistant Editor: Xiang LiResponsible Electronic Editor: Yan HuangProofing Editor-in-Chief: Lian-Sheng MaResponsible Science Editor: Xue-Jiao WangProofing Editorial Office Director: Ze-Mao GongCA 90822, United StatesPUBLICATION DATEApril 14, 2018NAME OF JOURNALWorld Journal of GastroenterologyISSNISSN 1007-9327 (print)ISSN 2219-2840 (online)LAUNCH DATEOctober 1, 1995FREQUENCYWeeklyEDITORS-IN-CHIEFDamian Garcia-Olmo, MD, PhD, Doctor, Professor, Surgeon, Department of Surgery, UniversidadAutonoma de Madrid; Department of General Surgery, Fundacion Jimenez Diaz University Hospital,Madrid 28040, SpainStephen C Strom, PhD, Professor, Department ofLaboratory Medicine, Division of Pathology, Karolinska Institutet, Stockholm 141-86, SwedenAndrzej S Tarnawski, MD, PhD, DSc (Med),Professor of Medicine, Chief Gastroenterology, VALong Beach Health Care System, University of California, Irvine, CA, 5901 E. Seventh Str., Long Beach,WJG www.wjgnet.comEDITORIAL BOARD MEMBERSAll editorial board members resources online at EDITORIAL OFFICEZe-Mao Gong, DirectorWorld Journal of GastroenterologyBaishideng Publishing Group Inc7901 Stoneridge Drive, Suite 501,Pleasanton, CA 94588, USATelephone: 1-925-2238242Fax: 1-925-2238243E-mail: editorialoffice@wjgnet.comHelp Desk: net.comPUBLISHERBaishideng Publishing Group Inc7901 Stoneridge Drive, Suite 501,Pleasanton, CA 94588, USATelephone: 1-925-2238242Fax: 1-925-2238243E-mail: bpgoffice@wjgnet.comHelp Desk: net.comIICOPYRIGHT 2018 Baishideng Publishing Group Inc. Articles published by this Open-Access journal are distributed underthe terms of the Creative Commons Attribution Noncommercial License, which permits use, distribution,and reproduction in any medium, provided the originalwork is properly cited, the use is non commercial and isotherwise in compliance with the license.SPECIAL STATEMENTAll articles published in journals owned by the BaishidengPublishing Group (BPG) represent the views and opinions of their authors, and not the views, opinions orpolicies of the BPG, except where otherwise explicitlyindicated.INSTRUCTIONS TO AUTHORSFull instructions are available online at http://www.wjgnet.com/bpg/gerinfo/204ONLINE SUBMISSIONhttp://www.f6publishing.comApril 14, 2018 Volume 24 Issue 14
World J Gastroenterol 2018 April 14; 24(14): 1550-1561Submit a Manuscript: http://www.f6publishing.comDOI: 10.3748/wjg.v24.i14.1550ISSN 1007-9327 (print) ISSN 2219-2840 (online)ORIGINAL ARTICLERandomized Controlled TrialMaintenance for healed erosive esophagitis: Phase Ⅲcomparison of vonoprazan with lansoprazoleKiyoshi Ashida, Katsuhiko Iwakiri, Naoki Hiramatsu, Yuuichi Sakurai, Tetsuharu Hori, Kentarou Kudou,Akira Nishimura, Eiji UmegakiKiyoshi Ashida, Department of Gastroenterology, RakuwakaiOtowa Hospital, Kyoto 607-8062, Japanwritten informed consent prior to study enrollment.Conflict-of-interest statement: Kiyoshi Ashida has receivedfees and honoraria from Takeda Pharmaceutical CompanyLimited and Otsuka Pharmaceutical Company Limited;Katsuhiko Iwakiri has received grants, fees, and honoraria fromTakeda Pharmaceutical Company Limited, and fees from OtsukaPharmaceutical Company Limited; Yuuichi Sakurai, TetsuharuHori, Kentarou Kudou, and Akira Nishimura are full-timeemployees of Takeda Pharmaceutical Company Limited; NaokiHiramatsu and Eiji Umegaki have no conflicts of interest todeclare.Katsuhiko Iwakiri, Department of Gastroenterology, NipponMedical School Graduate School of Medicine, Tokyo 113-8603,JapanNaoki Hiramatsu, Department of Gastroenterology andHepatology, Osaka Rosai Hospital, Sakai, Osaka 591-8025, JapanYuuichi Sakurai, Tetsuharu Hori, Kentarou Kudou, AkiraNishimura, Takeda Pharmaceutical Company Limited, Osaka540-8645, JapanData-sharing statement: No additional data are available.Eiji Umegaki, Department of Gastroenterology, Kobe UniversityGraduate School of Medicine, Kobe, Hyogo 650-0017, JapanOpen-Access: This article is an open-access article which wasselected by an in-house editor and fully peer-reviewed by externalreviewers. It is distributed in accordance with the CreativeCommons Attribution Non Commercial (CC BY-NC 4.0) license,which permits others to distribute, remix, adapt, build upon thiswork non-commercially, and license their derivative works ondifferent terms, provided the original work is properly cited andthe use is non-commercial. See: D number: Kiyoshi Ashida (0000-0002-5072-9399);Katsuhiko Iwakiri (0000-0002-5558-6104); Naoki Hiramatsu(0000-0002-8803-4488); Yuuichi Sakurai (0000-0003-3337-8213);Tetsuharu Hori (0000-0003-0638-6664); Kentarou Kudou(0000-0003-0125-6174); Akira Nishimura (0000-0001-6085-6829);Eiji Umegaki (0000-0003-3353-8096).Author contributions: Ashida K, Sakurai Y, Hori T andNishimura A were involved in study conception and design;Hiramatsu N served as Medical Expert; Umegaki E, Iwakiri Kand Ashida K served as the Central Adjudication Committee;Kudou K conducted statistical analyses; all authors were involvedin the drafting and critical revision of the manuscript, andapproved the final version, including the authorship list.Manuscript source: Unsolicited manuscriptCorrespondence to: Kiyoshi Ashida, MD, PhD, Departmentof Gastroenterology, Rakuwakai Otowa Hospital, 2 Otowachinjicho, Yamashina-ku, Kyoto 607-8062,Japan. rakuwadr1185@rakuwadr.comTelephone: 81-75-5934111Fax: 81-75-5934160Institutional review board statement: The study wasreviewed and approved by the institutional review board of eachparticipating site.Received: November 30, 2017Peer-review started: December 1, 2017First decision: December 13, 2017Revised: February 6, 2018Accepted: March 7, 2018Article in press: March 6, 2018Published online: April 14, 2018Clinical trial registration statement: This study is registeredat ClinicalTrials.gov. The registration identification number isNCT01459367.Informed consent statement: All study participants providedWJG www.wjgnet.com1550April 14, 2018 Volume 24 Issue 14
Ashida K et al. Vonoprazan in healed erosive esophagitis patientsAbstractreflux disease; however, symptoms of reflux persist insignificant numbers of patients treated with PPIs. Wecompared two doses of the novel potassium-competitiveacid blocker vonoprazan (10 and 20 mg once daily) withlansoprazole at its approved dose of 15 mg once dailyas maintenance therapy for healed EE in 607 Japanesepatients. Vonoprazan was shown to be non-inferior tolansoprazole 15 mg at both investigated doses, whiledemonstrating a similar safety profile.AIMTo compare vonoprazan 10 and 20 mg vs lansoprazole15 mg as maintenance therapy in healed erosiveesophagitis (EE).METHODSA total of 607 patients aged 20 years, with endo scopically-confirmed healed EE following 8 wk oftreatment with vonoprazan 20 mg once daily, wererandomized 1:1:1 to receive lansoprazole 15 mg (n 201), vonoprazan 10 mg (n 202), or vonoprazan20 mg (n 204), once daily. The primary endpointof the study was the rate of endoscopically-confirmedEE recurrence during a 24-wk maintenance period.The secondary endpoint was the EE recurrence rateat Week 12 during maintenance treatment. Additionalefficacy endpoints included the incidence of heartburnand acid reflux, and the EE healing rate 4 wk after theinitiation of maintenance treatment. Safety endpointscomprised adverse events (AEs), vital signs, electro cardiogram findings, clinical laboratory results, serumgastrin and pepsinogen Ⅰ/Ⅱ levels, and gastric mucosahistopathology results.Ashida K, Iwakiri K, Hiramatsu N, Sakurai Y, Hori T, KudouK, Nishimura A, Umegaki E. Maintenance for healed erosiveesophagitis: Phase Ⅲ comparison of vonoprazan withlansoprazole. World J Gastroenterol 2018; 24(14): 1550-1561Available from: URL: htm DOI: TIONGastroesophageal reflux disease (GERD) is a commongastric acid-related disorder that is characterized byheartburn and/or acid regurgitation caused by the[1]reflux of gastric contents . The spectrum of GERDranges from non-erosive to erosive or complicateddisease (ulcer, columnar metaplasia, and stricture),each of which is thought likely to progress if either[2]left untreated or not treated adequately . The maingoals for the clinical management of GERD consist ofsymptom relief, healing of erosive esophagitis (EE),prevention of recurrences and complications, and[1,3]overall improvement of patients’ quality of life .Owing to their superior ability to inhibit gastricacid secretion compared with H2 receptor antagonists(H2RAs), proton pump inhibitors (PPIs) remain the[1,3-5]mainstay of long-term therapy for GERD. However,resolution of GERD symptoms with PPIs appears tohave a less predictable outcome than esophageal[4-6]mucosal inflammation, with reflux symptomspersisting in up to 60% of patients treated with PPIs in[7]randomized controlled clinical trials and observational[5]studies . Proposed underlying mechanisms for PPIfailure include drug- and patient-related factors, such aslow bioavailability, nocturnal acid breakthrough, rapidmetabolism (CYP2C19 extensive metabolizer genotype),[6]and poor compliance with the prescribed regimen .The slow cumulative onset of PPI action at therapeutic[8-10]doses may also be a contributing factor. Theselimitations have led to a renewed interest in alternativetreatment modalities for the management of patients[1,4]with GERD .Discovered and developed by Takeda Pharmaceu tical Company Limited, Japan, vonoprazan fumarate(TAK-438) belongs to a novel class of acid suppressants[11]known as potassium-competitive acid blockers (P-CABs) . Like PPIs, vonoprazan inhibits gastric H , K -ATPase,RESULTSRates of EE recurrence during the 24-wk maintenanceperiod were 16.8%, 5.1%, and 2.0% with lansoprazole15 mg, vonoprazan 10 mg, and vonoprazan 20 mg,respectively. Vonoprazan was shown to be non-inferiorto lansoprazole 15 mg (P 0.0001 for both doses).In a post-hoc analysis, EE recurrence at Week 24 wassignificantly reduced with vonoprazan at both the 10 mgand the 20 mg dose vs lansoprazole 15 mg (5.1% vs16.8%, P 0.0002, and 2.0% vs 16.8%, P 0.0001,respectively); by contrast, the EE recurrence rate did notdiffer significantly between the two doses of vonoprazan(P 0.1090). The safety profiles of vonoprazan 10 and20 mg were similar to that of lansoprazole 15 mg inpatients with healed EE. Treatment-related AEs werereported in 11.4%, 10.4%, and 10.3% of patientsin the lansoprazole 15 mg, vonoprazan 10 mg, andvonoprazan 20 mg arms, respectively.CONCLUSIONOur findings confirm the non-inferiority of vonoprazan10 and 20 mg to lansoprazole 15 mg as maintenancetherapy for patients with healed EE.Key words: Gastroesophageal reflux disease; Erosiveesophagitis; Lansoprazole; Potassium-competitive acidblockers; Vonoprazan; Maintenance therapy The Author(s) 2018. Published by Baishideng PublishingGroup Inc. All rights reserved.Core tip: Proton pump inhibitors (PPIs), including lanso prazole, are widely used to maintain healing of erosiveesophagitis (EE) in patients with gastroesophagealWJG www.wjgnet.com1551April 14, 2018 Volume 24 Issue 14
Ashida K et al. Vonoprazan in healed erosive esophagitis patientsan enzyme that catalyzes the final step in the acidsecretion pathway. However, unlike PPIs, vonoprazan inhibits the enzyme in a K -competitive and reversible[12]manner , with its inhibitory effects (pKa 9.4) ongastric acid secretion largely unaffected by ambient pH,as it accumulates in parietal cells under both acidic and[12,13]resting conditions. In animal studies, vonoprazanproduced more potent and sustained suppression of[11-14]gastric acid secretion than lansoprazole. In healthyvolunteers, single doses of vonoprazan 1-120 mg werewell tolerated, and produced rapid, prolonged, and dose[15]related suppression of 24-h gastric acid secretion . Inanother study in healthy volunteers, these effects weremaintained with multiple dosing (10-40 mg once daily)[16]over 7 d, and were also dose-related .Lansoprazole 30 mg once daily is the recommendeddosage for healing EE, while its step-down dose of15 mg once daily is recommended for the maintenancetreatment of healed EE, providing well-balanced[17]efficacy and safety over the long term . The currentstudy aimed to demonstrate that vonoprazan 20 mgand its step-down dose of 10 mg once daily were noninferior to lansoprazole 15 mg once daily in preventingEE recurrence during a 24-wk maintenance period inJapanese patients who achieve EE healing after 2, 4,or 8 wk treatment with vonoprazan 20 mg.Helsinki, the International Council for Harmonizationof Technical Requirements for Pharmaceuticals forHuman Use (ICH) Harmonized Tripartite Guidelinefor Good Clinical Practice, and Japanese regulatoryrequirements. All patients provided written informedconsent prior to undergoing any study procedures.PatientsMale or female outpatients aged 20 years, whopresented with endoscopically-confirmed healed EE(no mucosal breaks) after up to 8 wk of treatment withvonoprazan 20 mg once daily, entered the maintenancephase of the study. Main exclusion criteria included:esophageal complications (e.g., eosinophilic esophagitis,esophageal varices, scleroderma, infection, esophagealstenosis); acute upper gastrointestinal bleeding;gastric or duodenal ulcer characterized by mucosaldefects; hypersecretion disorders, such as ZollingerEllison syndrome; serious neurologic, cardiovascular,pulmonary, hepatic [alanine aminotransferase (ALT) oraspartate aminotransferase (AST) 2.5 the upperlimit of normal (ULN)], renal (serum creatinine 2 mg/dL),metabolic, gastrointestinal, urologic, endocrinologic,or hematologic disorders; need for surgery; historyof drug (including alcohol) abuse; HIV or hepatitis;history of malignancy; and pregnancy or lactation infemales. Any sexually active female of childbearingpotential was required to use adequate contraceptivemeasures. Excluded concomitant medications includedPPIs, H2RAs, muscarinic M3 receptor antagonists,gastrointestinal motility stimulants, anticholinergicdrugs, prostaglandins, acid suppressants, anti-gastrindrugs, mucosal protective agents, H. pylori eradi cation therapies, atazanavir sulfate, and any otherinvestigational drug. As the exclusion of non-steroidalanti-inflammatory drugs (NSAIDs) would have beendifficult for patients eligible for inclusion in this study,their use was permitted; however, changes to NSAIDregimens during the study were prohibited.MATERIALS AND METHODSStudy designThis was a multicenter, randomized, double-blind,parallel-group, phase Ⅲ clinical study, which wasdesigned and conducted to demonstrate the noninferiority of vonoprazan 20 and 10 mg to lansoprazole15 mg as maintenance therapy in Japanese patientswith healed EE. During the initial treatment period,patients with EE Los Angeles (LA) Classification gradesA to D received vonoprazan 20 mg once daily forup to 8 wk. All patients in whom endoscopic healingof EE was confirmed 2, 4, or 8 wk after the start ofthe study medication were immediately stratified bybaseline endoscopic LA Classification grade (A/B orC/D), and subsequently randomized in a 1:1:1 ratioto receive maintenance therapy with vonoprazan10 mg, vonoprazan 20 mg, or lansoprazole 15 mggiven once daily after breakfast for 24 wk. All patientsin whom endoscopic healing of EE was not confirmedat Week 8 completed the study without entering themaintenance phase. All patients in whom EE recurrencewas endoscopically confirmed during maintenancetreatment were withdrawn from the study and handledas ‘completed cases’.Registered at ClinicalTrials.gov with the identifierNCT01459367, the study was conducted at 55 sitesin Japan between November 2011 and March 2013.The study protocol was reviewed and approved bythe Institutional Review Board at each study site, andwas conducted in accordance with the Declaration ofWJG www.wjgnet.comTreatment, randomization, and blindingPatients were randomized to treatment groups in a 1:1:1ratio according to a computer-generated randomizationschedule prepared by independent randomizationpersonnel. The independent rando mization personnelmanaged the randomization process, and stored therandomization schedule in a secure area. The randomi zation schedule incorporated LA Classification gradesas a stratification factor (A/B or C/D), to ensure thattreatment groups were balanced with respect to diseaseseverity. A double-dummy method, using matchedvonoprazan placebo tablets and lansoprazole placebocapsules, was employed to ensure that the double-blindconditions were maintained throughout the study.ProceduresMaintenance treatment was initiated on the day ofrandomization. Clinic visits were scheduled at Weeks1552April 14, 2018 Volume 24 Issue 14
Ashida K et al. Vonoprazan in healed erosive esophagitis patients4, 12, and 24, or upon early withdrawal from the study(discontinuation/recurrence). Endoscopic examinationswere performed at Weeks 12 and 24. A centraladjudication committee (CAC), composed of independentexperts, was established to perform standardizedand consistent reviews of endoscopic EE grading byinvestigators, while all decisions about patient eligibilityand withdrawal owing to EE recurrence were made bythe investigators, irrespective of the CAC’s assessment.Safety assessments were conducted at Weeks 4, 12, and24. Histopathologic examinations of the gastric mucosawere performed at the start of treatment (baseline)and at Week 24 for subjects enrolled at designatedstudy sites only. All biopsy specimens were full mucosallayer samples taken from the greater curvature of theupper gastric corpus during endoscopic procedures.Samples were fixed in 20% neutral buffered formalinand embedded in paraffin. Five slices were taken fromeach paraffin block, and were stained with hematoxylinand eosin, Grimelius, chromogranin, synaptophysin,and Ki-67 (MIB-1). For the CYP2C19 genotyping, asingle 2 mL blood sample was collected at Week 4, andwas analyzed to obtain information on genotypes thataffect the pharmacokinetics of lansoprazole. G681A (*2)and G636A (*3) of CYP2C19 were detected using anInvader assay. Both the histopathologic testing andCYP2C19 genotyping were carried out by MitsubishiChemical Medience Corporation, Tokyo, Japan. Thegastric mucosa histopathology findings reported by thecompany were reviewed by an independent assessmentcommittee, which assessed specimens for distributionpatterns of Grimelius-positive cells, chromograninA-positive cells, synaptophysin-positive cells, and Ki-67positive cells. Treatment compliance was assessed in allpatients on the basis of returned tablet/capsule countsat each study site visit.Although no evidence has been reported ofvonoprazan-associated liver function test abnorma [18]lities , drug-related hepatic changes have previouslybeen reported with another member of the P-CAB drug[19]class . Liver function abnormalities (ALT or AST 3 ULN, or total bilirubin 2 ULN in two consecutivemeasurements) were therefore classified as specialinterest adverse events (SIAEs) in the present study,and were monitored throughout.The primary study endpoint was the rate of recur rence of endoscopically-confirmed EE at Week 24 of themaintenance period. The secondary endpoint was therate of EE recurrence at Week 12 of the maintenanceperiod. Safety endpoints included adverse events (AEs),vital signs, electrocardiogram (ECG) findings, clinicallaboratory test values (hematology, serum chemistry,and urinalysis), serum gastrin and pepsinogenⅠ/Ⅱlevels, and gastric mucosa histopathologic findings.lansoprazole 15 mg and 30 mg, respectively, over 24[20]wk . It was therefore assumed that the endoscopicEE recurrence rate with vonoprazan 20 mg in thepresent study would be 14%, while the EE recurrencerate with vonoprazan 10 mg would be 22% - that is,halfway between the rates observed with lansoprazole15 mg and 30 mg in the study mentioned above.It was assumed that the EE recurrence rate withlansoprazole 15 mg would again be 30%. Based onthese assumptions, a sample size of 148 patientsper treatment group would provide 90% power toconfirm the non-inferiority of the two vonoprazan dosesto lansoprazole, with respect to the EE recurrencerate at Week 24, with a non-inferiority margin of 10%utilizing a two-sided 95% confidence interval (CI).Assuming a dropout rate of 15% during maintenancetherapy, 174 randomized patients would be requiredfor each treatment group. We therefore set therandomization target at 200 patients per treatmentgroup, to enable evaluation of the long-term safety ofvonoprazan in a sufficient number of patients.For the primary endpoint of EE recurrence rate atWeek 24 of maintenance treatment, frequency, pointestimates, and corresponding 95%CIs were calculatedby treatment group for the full analysis set (FAS),defined as all randomized patients who received atleast one dose of study drug during the maintenanceperiod. Vonoprazan 10 mg and 20 mg were evaluatedfor non-inferiority to lansoprazole 15 mg using the[21]Farrington and Manning testwith a non-inferioritymargin of 10%. The same analyses were performedfor the secondary endpoint.AEs (including their frequency, severity, investigatorassessed causality, and seriousness) and concomitantmedications were monitored throughout the study.Treatment-emergent adverse events (TEAEs) werecoded using the Medical Dictionary for RegulatoryActivities (MedDRA) version 16.0. All TEAEs weresummarized descriptively by treatment group, time ofonset, and severity, and were categorized by SystemOrgan Class and Preferred Term. All drug-relatedTEAEs were summarized by severity, while TEAEsleading to study discontinuation and serious TEAEswere summarized by treatment group.The statistical methods of this study were preparedand conducted by Kentarou Kudou of TakedaPharmaceutical Company Limited, and were reviewedand approved by Takamasa Hashimoto of TakedaPharmaceutical Company Limited, Osaka, Japan.RESULTSPatientsIn total, 737 patients signed the informed consentform. Of these 737 patients, 627 were enrolled into thetreatment phase, with 611 patients completing up to8 wk treatment for EE with vonoprazan 20 mg. Of the611 who completed treatment, 607, who representedboth the FAS and the safety analysis set (SAS), wereStatistical analysesA double-blind, controlled study of lansoprazole asmaintenance therapy for patients with healed EEreported EE recurrence rates of 30% and 14% withWJG www.wjgnet.com1553April 14, 2018 Volume 24 Issue 14
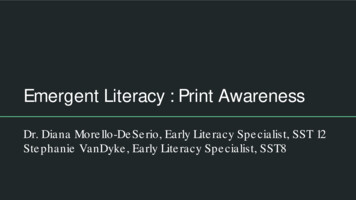
Ashida K et al. Vonoprazan in healed erosive esophagitis patientsAInformed consentRandomizationVonoprazan 10 mg (once daily)Vonoprazan 20 mg (once daily)Vonoprazan 20 mg (once daily)Lansoprazole 15 mg (once daily)Treatment period2, 4, or 8 wkMaintenance period(Subjects with endoscopically confirmed healed EE only)6 mo (24 wk)BInformed consent (n 737)Pretreatment event/adverse event (n 2)Voluntary withdrawal (n 20)Failure to meet entrance criteria (n 87)Other (n 1)Eligible for study entry (n 627)Pretreatment event/adverse event (n 4)Major protocol violation (n 4)Voluntary withdrawal (n 3)Lack of efficacy (n 1)Abnormal clinical values at start of treatment (n 3)Other (n 1)Completed treatment phase (n 611)Did not meet entrance criteria for maintenance phase (n 4)Randomized (n 607)Lansoprazole 15 mg (n 201)Pretreatment event/adverse event (n 8)Voluntary withdrawal (n 7)Completed maintenance phase (n 186)Vonoprazan 10 mg (n 202)Pretreatment event/adverse event (n 6)Lost to follow-up (n 1)Voluntary withdrawal (n 4)Other (n 1)Completed maintenance phase (n 190)Vonoprazan 20 mg (n 204)Pretreatment event/adverse event (n 8)Voluntary withdrawal (n 8)Other (n 1)Completed maintenance phase (n 187)Figure 1 Study design (A) and patient disposition (B). EE: Erosive esophagitis.randomized to maintenance therapy with lansoprazole15 mg (n 201), vonoprazan 10 mg (n 202), orvonoprazan 20 mg (n 204) (Figure 1). Five hundredsixty-three patients (92.8%) completed maintenancetreatment. The main reasons for premature studydiscontinuation were pretreatment events/AEs (n 22)and voluntary withdrawals (n 19). The first informedconsent form was signed on 21 November 2011, andthe last follow-up visit took place on 7 March 2013.The three maintenance groups were well matched interms of demographic and other baseline characteristics(Table 1), and had similar baseline EE severities andmedical histories. The mean treatment compliance ratewas 97% in each treatment group.therapy (primary endpoint) was 16.8%, 5.1%, and2.0% with lansoprazole 15 mg, vonoprazan 10 mg,and vonoprazan 20 mg, respectively. Point estimates ofdifferences in EE recurrence between the maintenancetreatment groups and 95%CIs are shown in Table 2.Vonoprazan 10 mg and 20 mg were both found to benon-inferior to lansoprazole 15 mg in the FAS (bothP 0.0001), with the upper limits of 95%CIs for thedifferences between vonoprazan 10 mg or 20 mgand lansoprazole 15 mg being 0, thus indicating astatistically significant difference. In a post-hoc analysisperformed using the Fisher exact test, a statisticallysignificant difference in the rate of EE recurrence wasdemonstrated between vonoprazan 10 mg or 20 mgand lansoprazole 15 mg (P 0.0002 and P 0.0001,respectively, vs lansoprazole 15 mg), but not betweenthe two vonoprazan doses (P 0.1090).EfficacyThe rate of EE recurrence at 24 wk of maintenanceWJG www.wjgnet.com1554April 14, 2018 Volume 24 Issue 14
Ashida K et al. Vonoprazan in healed erosive esophagitis patients1Table 1 Demographic and other baseline characteristics in the randomized set (n 607)CharacteristicLPZ 15 mg (n 201)VPZ 10 mg (n 202)VPZ 20 mg (n 204)57.8 12.9140 (69.7)163.5 10.267.0 13.455.5 13.8160 (79.2)165.5 9.368.2 12.356.8 13.6160 (78.4)165.6 9.369.0 13.1160 (79.6)41 (20.4)162 (80.2)40 (19.8)161 (78.9)43 (21.1)31
Medical School Graduate School of Medicine, Tokyo 113-8603, Japan Naoki Hiramatsu, Department of Gastroenterology and Hepatology, Osaka Rosai Hospital, Sakai, Osaka 591-8025, Japan Yuuichi Sakurai, Tetsuharu Hori, Kentarou Kudou, Akira Nishimura, Takeda Pharmaceutical Company Limited, Osaka 540-8645, Japan