Transcription
ISSN 1007-9327 (print)ISSN 2219-2840 (online)World Journal ofGastroenterologyWorld J Gastroenterol 2017 September 7; 23(33): 6009-6196Published by Baishideng Publishing Group Inc
SContentsWeekly Volume 23 Number 33 September 7, 2017EDITORIAL6009Helminths as an alternative therapy for intestinal diseasesSipahi AM, Baptista DMREVIEW6016Dextran sodium sulfate colitis murine model: An indispensable tool for advancing our understanding ofinflammatory bowel diseases pathogenesisEichele DD, Kharbanda KK6030Autoimmune hepatitis: Standard treatment and systematic review of alternative treatmentsTerziroli Beretta-Piccoli B, Mieli-Vergani G, Vergani DMINIREVIEWS6049Colorectal cancer, screening and primary care: A mini literature reviewHadjipetrou A, Anyfantakis D, Galanakis CG, Kastanakis M, Kastanakis S6059Behavioral gastroenterology: An emerging system and new frontier of actionJia L, Jiang SM, Liu JORIGINAL ARTICLEBasic Study6065Pharmacological evaluation of NSAID-induced gastropathy as a "Translatable" model of referred visceralhypersensitivityHummel M, Knappenberger T, Reilly M, Whiteside GT6077High yield reproducible rat model recapitulating human Barrett’s carcinogenesisMatsui D, Omstead AN, Kosovec JE, Komatsu Y, Lloyd EJ, Raphael H, Kelly RJ, Zaidi AH, Jobe BA6088Changes in expression of inhibitory substances in the intramural neurons of the stomach followingstreptozotocin- induced diabetes in the pigBulc M, Palus K, Zielonka L, Gajęcka M, Całka J6100HOX transcript antisense intergenic RNA represses E-cadherin expression by binding to EZH2 in gastriccancerChen WM, Chen WD, Jiang XM, Jia XF, Wang HM, Zhang QJ, Shu YQ, Zhao HBWJG www.wjgnet.com September 7, 2017 Volume 23 Issue 33
World Journal of GastroenterologyContents6111Volume 23 Number 33 September 7, 2017Ca2 /calmodulin-dependent protein kinase Ⅱ regulates colon cancer proliferation and migration viaERK1/2 and p38 pathwaysChen W, An P, Quan XJ, Zhang J, Zhou ZY, Zou LP, Luo HS6119Aberrant DNA-PKcs and ERGIC1 expression may be involved in initiation of gastric cancerWang FR, Wei YC, Han ZJ, He WT, Guan XY, Chen H, Li YMRetrospective Cohort Study6128Real world treatment patterns of gastrointestinal neuroendocrine tumors: A claims database analysisBenson III AB, Broder MS, Cai B, Chang E, Neary MP, Papoyan ERetrospective Study6137Patients with inflammatory bowel disease have increased risk of autoimmune and inflammatory diseasesHalling ML, Kjeldsen J, Knudsen T, Nielsen J, Koch-Hansen L6147Suspicious brush cytology is an indication for liver transplantation evaluation in primary sclerosingcholangitisBoyd S, Vannas M, Jokelainen K, Isoniemi H, Mäkisalo H, Färkkilä MA, Arola J6155Management of gastric mucosa-associated lymphoid tissue lymphoma in patients with extra copies of theMALT1 geneIwamuro M, Takenaka R, Nakagawa M, Moritou Y, Saito S, Hori S, Inaba T, Kawai Y, Toyokawa T, Tanaka T, Yoshino T,Okada H6164Ketogenic diet poses a significant effect on imbalanced gut microbiota in infants with refractory epilepsyXie G, Zhou Q, Qiu CZ, Dai WK, Wang HP, Li YH, Liao JX, Lu XG, Lin SF, Ye JH, Ma ZY, Wang WJObservational Study6172Definition of colorectal anastomotic leakage: A consensus survey among Dutch and Chinese colorectalsurgeonsvan Rooijen SJ, Jongen ACHM, Wu ZQ, Ji JF, Slooter GD, Roumen RMH, Bouvy NDCASE REPORT6181How to treat intestinal obstruction due to malignant recurrence after Whipple’s resection for pancreatic headcancer: Description of 2 new endoscopic techniquesMouradides C, Taha A, Borbath I, Deprez PH, Moreels TG6187Arterioportal shunt incidental to treatment with oxaliplatin that mimics recurrent gastric cancerKim HB, Park SGWJG www.wjgnet.comIISeptember 7, 2017 Volume 23 Issue 33
World Journal of GastroenterologyContentsVolume 23 Number 33 September 7, 2017LETTERS TO THE EDITOR6194Comment on “Effect of biofilm formation by clinical isolates of Helicobacter pylori on the efflux-mediatedresistance to commonly used antibiotics”Kazakos EI, Dorrell N, Polyzos SA, Deretzi G, Kountouras JWJG www.wjgnet.comIIISeptember 7, 2017 Volume 23 Issue 33
World Journal of GastroenterologyContentsVolume 23 Number 33 September 7, 2017ABOUT COVEREditorial Board Member of World Journal of Gastroenterology, Mostafa Sira,MD, Associate Professor of Pediatric Hepatology, Gastroenterology and Nutrition, National Liver Institute, Menofiya University, Menofiya 32511, EgyptAIMS AND SCOPEWorld Journal of Gastroenterology (World J Gastroenterol, WJG, print ISSN 1007-9327, onlineISSN 2219-2840, DOI: 10.3748) is a peer-reviewed open access journal. WJG was established on October 1, 1995. It is published weekly on the 7th, 14th, 21st, and 28th each month.The WJG Editorial Board consists of 1375 experts in gastroenterology and hepatologyfrom 68 countries.The primary task of WJG is to rapidly publish high-quality original articles, reviews,and commentaries in the fields of gastroenterology, hepatology, gastrointestinal endoscopy, gastrointestinal surgery, hepatobiliary surgery, gastrointestinal oncology, gastrointestinal radiation oncology, gastrointestinal imaging, gastrointestinal interventional therapy, gastrointestinal infectious diseases, gastrointestinal pharmacology, gastrointestinalpathophysiology, gastrointestinal pathology, evidence-based medicine in gastroenterology, pancreatology, gastrointestinal laboratory medicine, gastrointestinal molecular biology, gastrointestinal immunology, gastrointestinal microbiology, gastrointestinal genetics,gastrointestinal translational medicine, gastrointestinal diagnostics, and gastrointestinaltherapeutics. WJG is dedicated to become an influential and prestigious journal in gastroenterology and hepatology, to promote the development of above disciplines, and toimprove the diagnostic and therapeutic skill and expertise of clinicians.INDEXING/ABSTRACTINGWorld Journal of Gastroenterology (WJG) is now indexed in Current Contents /Clinical Medicine,Science Citation Index Expanded (also known as SciSearch ), Journal Citation Reports , IndexMedicus, MEDLINE, PubMed, PubMed Central and Directory of Open Access Journals. The2017 edition of Journal Citation Reports cites the 2016 impact factor for WJG as 3.365 (5-yearimpact factor: 3.176), ranking WJG as 29th among 79 journals in gastroenterology and hepatology (quartile in category Q2).FLYLEAFI-IXEDITORS FORTHIS ISSUEResponsible Assistant Editor: Xiang LiResponsible Electronic Editor: Yan HuangProofing Editor-in-Chief: Lian-Sheng MaNAME OF JOURNALWorld Journal of GastroenterologyISSNISSN 1007-9327 (print)ISSN 2219-2840 (online)LAUNCH DATEOctober 1, 1995FREQUENCYWeeklyEDITORS-IN-CHIEFDamian Garcia-Olmo, MD, PhD, Doctor, Professor, Surgeon, Department of Surgery, UniversidadAutonoma de Madrid; Department of General Surgery, Fundacion Jimenez Diaz University Hospital,Madrid 28040, SpainStephen C Strom, PhD, Professor, Department ofLaboratory Medicine, Division of Pathology, Karolinska Institutet, Stockholm 141-86, SwedenAndrzej S Tarnawski, MD, PhD, DSc (Med),Professor of Medicine, Chief Gastroenterology, VALong Beach Health Care System, University of California, Irvine, CA, 5901 E. Seventh Str., Long Beach,WJG www.wjgnet.comEditorial BoardResponsible Science Editor: Li-Juan WeiProofing Editorial Office Director: Jin-Lei WangCA 90822, United Stateshttp://www.wjgnet.comEDITORIAL BOARD MEMBERSAll editorial board members resources online at PUBLICATION DATESeptember 7, 2017EDITORIAL OFFICEJin-Lei Wang, DirectorYuan Qi, Vice DirectorZe-Mao Gong, Vice DirectorWorld Journal of GastroenterologyBaishideng Publishing Group Inc7901 Stoneridge Drive, Suite 501,Pleasanton, CA 94588, USATelephone: 1-925-2238242Fax: 1-925-2238243E-mail: editorialoffice@wjgnet.comHelp Desk: net.comPUBLISHERBaishideng Publishing Group Inc7901 Stoneridge Drive, Suite 501,Pleasanton, CA 94588, USATelephone: 1-925-2238242Fax: 1-925-2238243E-mail: bpgoffice@wjgnet.comHelp Desk: http://www.f6publishing.com/helpdeskIVCOPYRIGHT 2017 Baishideng Publishing Group Inc. Articles published by this Open-Access journal are distributed underthe terms of the Creative Commons Attribution Noncommercial License, which permits use, distribution,and reproduction in any medium, provided the originalwork is properly cited, the use is non commercial and isotherwise in compliance with the license.SPECIAL STATEMENTAll articles published in journals owned by the BaishidengPublishing Group (BPG) represent the views and opinions of their authors, and not the views, opinions orpolicies of the BPG, except where otherwise explicitlyindicated.INSTRUCTIONS TO AUTHORSFull instructions are available online at http://www.wjgnet.com/bpg/gerinfo/204ONLINE SUBMISSIONhttp://www.f6publishing.comSeptember 7, 2017 Volume 23 Issue 33
World J Gastroenterol 2017 September 7; 23(33): 6128-6136Submit a Manuscript: http://www.f6publishing.comDOI: 10.3748/wjg.v23.i33.6128ISSN 1007-9327 (print) ISSN 2219-2840 (online)ORIGINAL ARTICLERetrospective Cohort StudyReal-world treatment patterns of gastrointestinalneuroendocrine tumors: A claims database analysisAl B Benson III, Michael S Broder, Beilei Cai, Eunice Chang, Maureen P Neary, Elya PapoyanAl B Benson III, Northwestern University, Chicago, IL 60208,United StatesOpen-Access: This article is an open-access article which wasselected by an in-house editor and fully peer-reviewed by externalreviewers. It is distributed in accordance with the CreativeCommons Attribution Non Commercial (CC BY-NC 4.0) license,which permits others to distribute, remix, adapt, build upon thiswork non-commercially, and license their derivative works ondifferent terms, provided the original work is properly cited andthe use is non-commercial. See: ael S Broder, Eunice Chang, Elya Papoyan, Partnershipfor Health Analytic Research, LLC, Beverly Hills, CA 90212,United StatesBeilei Cai, Maureen P Neary, Novartis Pharmaceuticals, EastHanover, NJ 07936, United StatesManuscript source: Unsolicited manuscriptAuthor contributions: All authors were equally involved in thedesign of the study; Chang E conducted the statistical analysesand all authors contributed equally in the interpretation of resultsand writing of the manuscript.Correspondence to: Michael S Broder, MD, MSHS,Partnership for Health Analytic Research, LLC, 280 S. BeverlyDrive, Suite 404, Beverly Hills, CA 90212,United States. mbroder@pharllc.comTelephone: 1-310-8589555Fax: 1-310-8589552Supported by Novartis Pharmaceuticals, One Health Plaza, EastHanover, No. NJ 07936-1080, United State.Institutional review board statement: We conducted aretrospective cohort study using the Truven Health AnalyticsMarketScan Database and the IMS Health Pharmetrics Database,both commercial health insurance claims database for employerinsured beneficiaries in the United States. The databases arefully compliant with the Health Insurance Portability andAccountability Act and meets the criteria for a limited-usedataset. Since the patient and provider data included in thisanalysis were fully de-identified, this study was exempt from theInstitutional Review Board review.Received: February 9, 2017Peer-review started: February 9, 2017First decision: April 21, 2017Revised: May 9, 2017Accepted: June 18, 2017Article in press: June 19, 2017Published online: September 7, 2017Conflict-of-interest statement: Cai B and Neary MP areemployees of Novartis Pharmaceuticals Corporation; Benson IIIAB was paid as a research consultant for the study as a subjectmatter expert by Novartis and is an employee of NorthwesternUniversity; Broder MS, Chang E and Papoyan E are employeesof Partnership for Health Analytic Research, LLC (PHAR, LLC),a health services research company paid by Novartis to conductthis research.AbstractAIMTo describe real-world treatment patterns of gastro intestinal neuroendocrine tumors (GI NET).METHODSIn this retrospective cohort study, we used 2009-2014data from 2 United States commercial claims databasesto examine newly pharmacologically treated patientsusing tabular and graphical techniques. Treatmentsincluded somatostatin analogues (SSA), cytotoxicchemotherapy (CC), targeted therapy (TT), interferonData sharing statement: The study statistician, EuniceChang, conducted all statistical analysis for this study usingHealth Insurance Portability and Accountability Act-compliantcommercial-insurance secondary databases MarketScan andPharMetrics.WJG www.wjgnet.com6128September 7, 2017 Volume 23 Issue 33
Benson III AB et al . GI NET treatment patterns(IF) and combinations. We identified patients at least18 years of age, with 1 inpatient or 2 outpatientclaims for GI NET who initiated pharmacologictreatment from 7/1/09-6/30/14. A 6 mo clean periodprior to first treatment ensured patients were newlytreated. Patients were followed until end of enrollmentor the study end date, whichever was first.INTRODUCTIONNeuroendocrine tumors (NET) comprise a broadfamily of rare and often slow growing malignancies.NET can develop anywhere in the body and arisefrom neuroendocrine cells throughout the endocrine[1,2]system . Approximately two-thirds of NET tumorsoccur in the gastrointestinal (GI) tract. These sitesinclude the stomach, small intestine, appendix, colon,[3]and rectum . NET secrete peptides and neuroaminesthat cause distinct syndromes (e.g., carcinoid syn drome), in which case they are referred to as “functional”tumors. Clinical presentation depends on the site ofthe primary tumor and whether they are functional.Surgery may be curative in the early stages, butdelayed diagnosis is typical.While rare, the incidence and prevalence of NET[4-8]appear to be increasing worldwide . The incidenceof NET in the United States increased from 10.9 casesper million person-years (PMPY) in 1973 to 52.5 PMPYin 2004, and to 69.8 PMPY in 2012 as reported usingthe United States Surveillance Epidemiology and End[4,9]Results database . Prevalence also increased andwas reported as 216 per million per year for GI NET inthe United States.The management of GI NET is based on a varietyof factors including stage, anatomic location, and thepresence and type of symptoms. The most recentNCCN guidelines for unresectable and metastatic GINET recommend somatostatin analogues (SSA) asfirst-line treatment, but do not recommend a particular[10]treatment sequence for the remaining therapies .Considering the heterogeneity of GI NET tumors andthe resultant lack of specificity in guidelines, we aimedto describe the current real-world treatment patternsof GI NET in a large sample of patients.RESULTSWe identified 2258 newly treated GI NET patients:mean (SD) age was 55.6 years (SD 9.7), 47.2%of the patients were between 55 and 64 years, and48.8% were female. All regions of the United Stateswere represented. 59.6% started first-line therapy withSSA monotherapy (964 with octreotide LAR, 380 withoctreotide SA, and 1 with lanreotide), 33.3% CC, 3.6%TT, and 0.5% IF. The remainder received combinations.Mean follow up was 576 d. Overall mean first-line the rapy duration was 361 d (449 d for SSA, 215 for CC,267 for TT). 58.9% of patients had no pharmacologicaltreatment beyond first line. The most common secondline was combination therapy with SSA. In graphicalpattern analysis, there was no clear pattern visible afterfirst line therapy.CONCLUSIONIn this study, 60% of patients initiated treatmentwith SSA alone or in combination. The relatively longtime to discontinuation suggests possible sustainedeffectiveness and tolerability.Key words: Gastrointestinal neuroendocrine tumors;Treatment patterns; Insurance claims; Somatostatinanalogue; Targeted therapy; Chemotherapy The Author(s) 2017. Published by Baishideng PublishingGroup Inc. All rights reserved.Core tip: In this retrospective study of real-worldtreatment patterns, somatostatin analogues werethe most common initial pharmacologic treatmentin patients with gastrointestinal neuroendocrinetumors, and most of the remaining patients begantreatment with chemotherapy. However, despite themany treatment options, over half of the patientsdiscontinued treatments after first line and onlyless than 10% of patients received any second-linepharmacotherapy. Given limitations of claims data toelucidate reasons for this lack of continued treatment,a study using more detailed clinical information such asmedical charts or physician surveys is warranted.MATERIALS AND METHODSData sourceWe conducted a longitudinal, retrospective cohortanalysis of newly pharmacologically treated GI NETpatients using two large United States commercialclaims databases. Data from the Truven HealthAnalytics MarketScan database and the IMS Phar Metrics database (both using dates from January1, 2009 to December 31, 2014) were combined toincrease sample size. To prevent duplicate records,patients with the same age, gender, region, and dateof first GI NET diagnosis in a calendar year foundin both databases were randomly removed fromone of the databases. Both databases are HealthInsurance Portability and Accountability Act compliantadministrative claims databases that contain deidentified adjudicated medical claims (e.g., inpatientand outpatient services) and pharmacy claims (e.g.,outpatient prescriptions) submitted for payment byBenson III AB, Broder MS, Cai B, Chang E, Neary MP,Papoyan E. Real-world treatment patterns of gastrointestinalneuroendocrine tumors: A claims database analysis. World JGastroenterol 2017; 23(33): 6128-6136 Available from: 128.htm DOI:http://dx.doi.org/10.3748/wjg.v23.i33.6128WJG www.wjgnet.com6129September 7, 2017 Volume 23 Issue 33
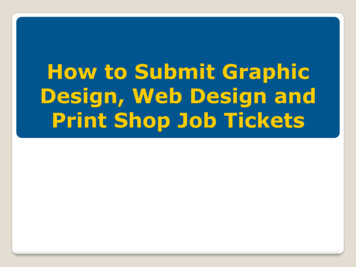
Benson III AB et al . GI NET treatment patternsDay 1(first GI NET pharmacologic treatment)6-mo washout period(No GI NET treatment)Follow-up period(Until the end of enrollment or 12/31/14)1/1/0912/31/147/1/096/30/14Identification periodFigure 1 Study timeline. The first gastrointestinal neuroendocrine tumors (GI NET) pharmacologic treatment claim on or after the appearance of the GI NETdiagnosis code and within the ID period (7/1/2009 to 6/30/2014) was considered to be the index date. Patients were required to be enrolled for a baseline period of atleast six months before the index date. Patient follow-up was variable and continued until the end of enrollment or the study end date (12/31/14), whichever was first.providers, healthcare facilities, and pharmacies. Forboth data sources, claims include information on eachphysician visit, medical procedure, hospitalization,drug dispensed, date of service, number of days ofmedication supplied, test performed, and completepayment information. Each medical claim has a principaldiagnosis and secondary diagnoses codes associatedwith it. Available patient demographic informationincludes age, gender, and geographic region. Dates ofenrollment and disenrollment are also recorded. As thedata were fully de-identified, this study was consideredexempt from approval by the Institutional ReviewBoard.temozolomide, streptozotocin, doxorubicin, liposomaldoxorubicin, fluorouracil, capecitabine, dacarbazine,oxaliplatin and thalidomide. Pharmacologic therapywas identified in claims using both the HealthcareCommon Procedure Coding System (HCPCS) andNational Drug Codes (NDC). Liver directed therapiescomprised liver resection, transplant, lesion ablation(using radiotherapy, cryotherapy, microwave andthermal energy, and including laparoscopic, openand percutaneous routes), embolization (includingbland, radioisotope, and chemotherapy), and radiationtherapy. Liver directed therapies were identified inclaims using HCPCS, ICD-9-CM, and Current ProceduralTerminology (CPT) codes. Chemotherapy observedonly once and on the same date as embolization wasconsidered chemoembolization and not part of a pharma cologic regimen.First-line therapy was defined as the pharmacologictreatment regimen observed on, or within threemonths of, the index date. Therapy included mono therapy or combination therapies. A three-monthperiod after the index date was used to identifypharmacologic therapy intended as first-line but notadministered on the index date. This would include,for example, combination chemotherapy where thesecond agent is given after some delay. Second-linetherapy was defined as beginning when treatment wasswitched from one category of pharmacotherapy toanother (e.g., from SSA alone to CC alone), or when anew category of treatment was added (e.g., from SSAalone to SSA plus CC). Changes from one cytotoxicagent to another, or one SSA to another, were notconsidered a switch. The first day of treatment switchor addition was defined as the initiation date of secondline therapy.Cohort selectionPatients at least 18 years of age were identifiedfrom each dataset if they had at least 1 inpatient or2 outpatient claims with an International StatisticalClassification of Disease-9-Clinical Modification (ICD9-CM) for GI NET (209.00-209.03, 209.10-209.17,209.23, 209.24-209.27, 209.40-209.43,209.50-209.57, 209.62, 209.65-209.67) during thestudy period (1/1/2009-12/31/2014). The first GINET pharmacologic treatment claim on or after theappearance of the GI NET diagnosis code and withinthe ID period (7/1/2009 to 6/30/2014) was consideredto be the index date. Patients were required to beenrolled for a baseline period of at least six monthsbefore the index date. To ensure new treatment,patients with any evidence of pharmacologic treatmentduring this baseline period were excluded. In ordernot to include the same patient twice, we searched forany patients with the same age, gender, region, anddate of GI NET diagnosis who could be found in bothdatabases, but we found none. Patient follow-up wasvariable and continued until the end of enrollment orthe study end date (12/31/2014), whichever was first(Figure 1).Statistical analysisMeans and proportions were presented in tabularanalyses. An inverse Kaplan-Meier curve was usedto show duration of first-line therapy. All datatransformations and statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).Graphical analyses were conducted using GRAPHx ,a proprietary graphics-based algorithm. The GRAPHxmethod uses multi-colored line segments to representStudy variables and measuresThe primary outcome measure was the use ofpharmacologic or liver directed therapy. Pharmaco therapy was divided into four groups: SSA, TT, CCand IF. SSA included octreotide and lanreotide, TTincluded everolimus and sunitinib, and CC includedWJG www.wjgnet.com6130September 7, 2017 Volume 23 Issue 33
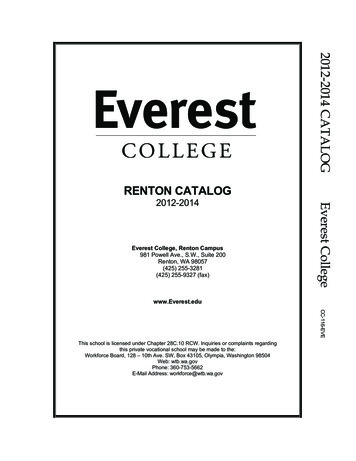
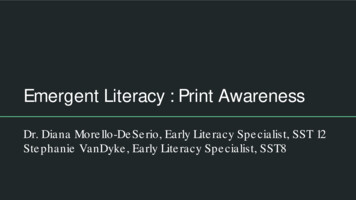
Benson III AB et al . GI NET treatment patternsMarketScan databasePharMetrics database2453 GI NET patients received1pharmacologic treatment in ID period(7/1/2009-6/30/2014)2900 GI NET patients received1pharmacologic treatment in ID period(7/1/2009-6/30/2014)435 had treatment in the 6 mopre-index period430 had treatment in the 6mopre-index periodn 2470n 20183711 started treatment beforethe first GI NET diagnosis2932 started treatment beforethe first GI NET diagnosisn 1538n 13077 were 18 yr old1 was 18 yr oldn 1306n 1531264 were not continuouslyenrolled in 6 mo pre-index period315 were not continuouslyenrolled in 6 mo pre-index periodn 1042n 12162258 Newly treated GI NET patientsFigure 2 Patient identification. There were 2900 and 2453 gastrointestinal neuroendocrine tumors (GI NET) patients who also had a claim for pharmacologictreatment between 7/1/2009 and 6/30/2014 in the MarketScan and PharMetrics databases, respectively. After excluding patients who had treatment during a 6-mopre-index period (and therefore were considered to be continuing, rather than initiating, treatment); received treatment before receiving a diagnosis of GI NET; were 18 yr old; or were not continuously enrolled in the 6-mo pre-index period, there remained 2258 newly treated GI NET patients who were included in the study.1Somatostatin analogues (SSAs), targeted therapy, cytotoxic chemotherapy, or interferon; 2324 (34.8%) within 3 mo, and 516 (55.4%) within 6 mo; 3249 (35.0%) within3 mo, and 380 (53.4%) within 6 mo.various treatments, plotting them over time. Theimages are reviewed visually for the presence andlength of segments and change in colors and patternsover time.Mean duration of first-line therapy was 361 d (SD 385) for all newly treated patients. The mean observedduration of treatment for first-line SSA monotherapyusers was 449 d (SD 434.2). It was 215 d (SD 228.8) for first-line CC monotherapy and 267 d (SD 325.7) for first-line TT monotherapy (Table 2). By 588d of treatment (1.61 years), half of SSA initiators haddiscontinued treatment, compared to 182 d (0.498years) for half of CC users and 171 d (0.47 years) forhalf of TT users to discontinue treatment (Figure 3).Liver directed therapy was used by 12.5% during firstline pharmacologic therapy; another 3.7% received itsometime after the first-line (Table 2).By the end of the study follow-up period [mean(SD, median) of 576 d (447.1, 454)] 58.9% (n 1331) patients had stopped pharmacologic therapycompletely. These patients continued to be enrolledin one of the databases but no longer had claimsfor pharmacologic treatment. In Figure 4, thesepatients can be identified as colored line segmentsthat terminate in gray segments of variable length,with the gray representing the period of no treatment.An additional 32.7% (n 738) continued their initialtherapy until the end of their enrollment; thesepatients were still receiving their first-line therapy atthe time they left a covered plan or reached the endof study. This pattern is shown in Figure 4 as a coloredsegment terminating in white. The remaining 8.4%(n 189) were observed to change pharmacologictreatment during the follow-up period (a coloredsegment terminating in different colored segment)RESULTSThere were 2900 and 2453 patients meeting thedefinition of GI NET who also had a claim for pharma cologic treatment between 7/1/2009 and 6/30/2014 inthe MarketScan and PharMetrics databases, respectively.After excluding patients who had treatment during a6-mo pre-index period (and therefore were consideredto be continuing, rather than initiating, treatment);received treatment before receiving a diagnosis of GINET; were 18 years old; or were not continuouslyenrolled in the 6-mo pre-index period, there remained2258 newly treated GI NET patients who were includedin the study (Figure 2).Gender was evenly split with n 1103 (48.8%)female patients and n 1155 (51.2%) male. Theaverage age was 55.6 years (SD 9.7) and 47.2% ofthe patients were between 55 and 64 years. All regionsof the United States were represented. More than halfof patients, n 1345 (59.6%), were treated with SSAas first-line monotherapy, 964 with octreotide LAR, 380with octreotide SA, and 1 with lanreotide. An additional75 patients (3.3%) received SSA in combination withother either CC, TT or IF. The second largest group, n 752 (33.3%), was treated with CC monotherapy,and n 81 (3.6%) received TT monotherapy (Table 1).WJG www.wjgnet.com6131September 7, 2017 Volume 23 Issue 33
WJG www.wjgnet.com6132183 (24.3)150 (19.9)323 (43.0)96 (12.8)41 (5.5)122 (16.2)159 (21.1)168 (22.3)174 (23.1)88 (11.7)514(409.1)393321 (23.9)261 (19.4)563 (41.9)200 (14.9)130 (9.7)271 (20.1)282 (21.0)270 (20.1)268 (19.9)124 (9.2)621(468.5)500454(403.6)2904 (4.9)15 (18.5)33 (40.7)16 (19.8)9 (11.1)20 (24.7)12 (14.8)36 (44.4)13 (16.0)4 (4.9)813.6%54.9 10.50 (0)4 (4.9)9 (11.1)18 (22.2)39 (48.1)11 (13.6)40 (49.4)588(424.1)45511 (26.2)17 (40.5)4 (9.5)3 (7.1)5 (11.9)13 (31.0)11 (26.2)12 (28.6)6 (14.3)2 (4.8)421.9%53.5 10.91 (2.4)3 (7.1)4 (9.5)12 (28.6)20 (47.6)2 (4.8)26 (61.9)SSA CC425(269.6)3607 (22.6)5 (16.1)10 (32.3)4 (12.9)4 (12.9)7 (22.6)7 (22.6)15 (48.4)2 (6.5)1 (3.2)311.4%53.8 10.10 (0)0 (0)4 (12.9)12 (38.7)11 (35.5)4 (12.9)17 (54.8)SSA TTFirst-line treatment244(140.7)2160 (0)0 (0)0 (0)2 (66.7)1 (33.3)0 (0)1 (33.3)2 (66.7)0 (0)0 (0)30.1%59.3 3.80 (0)0 (0)0 (0)0 (0)3 (100.0)0 (0)1 (33.3)TT CC675(145.7)6751 (50.0)0 (0)1 (50.0)0 (0)0 (0)1 (50.0)0 (0)1 (50.0)0 (0)0 (0)20.1%58.5 3.50 (0)0 (0)0 (0)0 (0)2 (100.0)0 (0)1 (50.0)IF964 with octreotide LAR, 380 with octreotide SA, and 1 with lanreotide. SSA: Somatostatin analogues; CC: Cytotoxic chemotherapy; TT: Targeted therapy; IF: Interferon.75233.3%54.7 9.92 (0.3)25 (3.3)92 (12.2)225 (29.9)338 (44.9)70 (9.3)341 (45.3)1345159.6%56.3 9.56 (0.4)20 (1.5)121 (9.0)371 (27.6)651 (48.4)176 (13.1)677 (50.3)TT836N/A8360 (0)0 (0)0 (0)0 (0)0 (0)0 (0)0 (0)0 (0)1 (100.0)1 (100.0)10.0N/A0 (0)0 (0)0 (0)0 (0)1 (100.0)0 (0)0 (0.0)SSA IF496N/A4960 (0)0 (0)1 (100.0)0 (0)0 (0)0 (0)0 (0)1 (100.0)0 (0)0 (0)10.0N/A0 (0)0 (0)0 (0)0 (0)1 (100.0)0 (0)0 (0.0)SSA TT CC576(447.1)454416 (18.4)478 (21.2)487 (21.6)467 (20.7)231 (10.2)545 (24.1)442 (19.6)953 (42.2)318 (14.1)179 (7.9)2258100.0%55.6 9.79 (0.4)52 (2.3)230 (10.2)638 (28.3)1066 (47.2)263 (11.6)1103 (48.8)All newly treatedpatientsThis study used two very large, nationally repre sentative claims databases, which together represent up to 100 million covered lives, to describe real-world treatmentof GI NET. Three findings were of particular interest. First, the most common initial pharmacologic treatment was with SSA, with average duration of use of just over 18mo. Second, although 60% of patients initiated treatment with SSA alone or in combination, most of the remainder began treatment with CC, therapy recommendedDISCUSSION(Figure 4 and Table 2). Among these 189 patients who were observed to begin second-line therapy, 128 (67.7%) had initially been treated with SSA. Among these128 first-line SSA users, 89 (69.5%) added additional therapy (e.g., CC or TT) as their second-line treatment. In patients who did not begin therapy with SSA, mostreceived SSA monotherapy or combination therapy as second-line (Table 3). Liver direc
Supported by Novartis Pharmaceuticals, One Health Plaza, East Hanover, No. NJ 07936-1080, United State. Institutional review board statement: We conducted a retrospective cohort study using the Truven Health Analytics MarketScan Database and the IMS Health Pharmetrics Database, both commercial health insurance claims database for employer-