Transcription
Clareon IOL: A NewMonofocalPlatformA Sponsored Supplement FromHighlights from Alcon’s Satellite Symposium,held on October 9, 2017, at the XXXVCongress of the ESCRS, Lisbon, Portugal.PresentersRudy Nuijts, Maastricht University Medical Center,Maastricht, The Netherlands (Moderator)Liliana Werner, John A. Moran Eye Center,University of Utah, Salt Lake City, Utah, USAGerd Auffarth, International Vision CorrectionResearch Centre (IVCRC), David J. Apple InternationalLaboratory for Ocular Pathology, University ofHeidelberg, Heidelberg, GermanyStephen Lane, Clinical Professor of Ophthalmologyat the University of Minnesota and Medical Directorof Associated Eye Care in Stillwater, Minnesota, USA;and Chief Medical Officer of AlconThis supplement solely reflects the views, opinions and experiencesof presenters who participated in the ESCRS congress in Lisbonon October 9, 2017. Data presented are representative of eachparticipating surgeons’ own experience, and do not arise from formalclinical studies. Trademarks are the property of their respective owners.www.alcon.com
2 S p o ns o r e d F e a tu r eClareon IOL:A New MonofocalPlatformCataract surgery is constantly advancingand evolving, and one key area ofinnovation is the intraocular lens (IOL)design and biomaterial. Alcon is a companywhich has a vast history of manufacturingand developing best in class IOLs.Recently, Alcon has achieved 100 millionimplantations of the AcrySof platform,one of the world’s most frequentlyimplanted IOLs (1). Alcon is also acustomer centric company and listens tofeedback from cataract surgeons about theimprovements they would like to see in thenext generation of IOLs – specifically, highbiocompatibility and even greater opticalclarity. Hence, Alcon has developed a nextgeneration of IOLs: Clareon .Clareon is an advanced monofocalIOL that is made from a new hydrophobicacr ylic mater ial and enhancedmanufacturing process, along with thetrusted AcrySof platform features (2;see Box 1). These two key innovationsenable the Clareon precision edgedesign (3), which bestows severalbenefits, including significantly loweredge glare (4) and low incidences ofposterior capsule opacification (PCO) –and subsequent YAG rates (2). Previousstudies in Europe and Japan performedwith the same Clareon IOL materialhave shown Nd:YAG rates of 1.5 and 0%, respectively (2), which is comparableto current AcrySof data (2.2 %) (5).AutonoMe Clareon was presentedat the XXXV annual Congress of theESCRS in Lisbon, Portugal, where leadingcataract surgeons overviewed data onClareon bio-optics, biomechanics andbiomaterial features, and also introducedthe AutonoMe pre-loaded IOLdelivery device.Box 1 – Clareon : A New Monofocal IOL PlatformKey Bio-optics Features Precision edge design to minimizepotential for edge glare and positivedysphotopsias, as well as guardingagainst PCO and minimizingNd:YAG procedures (2-4) Fully usable 6 mm biconvexaspheric optic (6) UV and blue light filtering (2) Refractive index: 1.55 (2)Key Biomechanics Features STABLEFORCE Haptics for lowaxial displacement, decentrationand tilt (7) Rapid and controlled unfolding,with haptics that remain planar (8)Key Biomaterial Features Unsurpassed optical clarity(9-12)* Manufactured using an advancedprocess (12) Resistant to phase separation (9) Amongst the lowest levelof surface haze, subsurfacenanoglistenings (SSNGs), andglistenings of competitivemonofocal IOLs (9-12)*Lens SpecificationsClareon Optic typeAsymmetric biconvex opticAsphericity-0.2 µm (anterior surface)Optic materialHydrophobic acrylicOptic diameter6.0 mm diameterOverall length13.0 mmIOL powers (equivalent diopters) 6.0 to 30.0 D (in 0.5 D increments)Haptic angulation0 planarHaptic configurationSTABLEFORCE modified IOL hapticsPhotoprotectionUV and blue light filtrationRefractive index1.55Suggested A-constant (SKR-T)119.1 (PCI-Optical)PCI, partial coherence interferometer.Precision edge design (3)*Based on aggregate results from in vitro evaluations of haze, SSNGs and glistenings compared to TECNIS§§ OptiBlue§§ZCB00V (Abbott), TECNIS§§ ZCB00 (Abbott), Eternity Natural Uni§§ W-60 (Santen), Vivinex§§ XY-1 (HOYA) and enVista§§MX60 (B&L; Bausch & Lomb). §§Trademarks are the property of their respective owners.
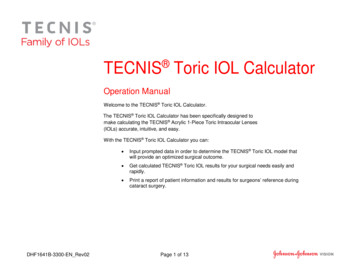
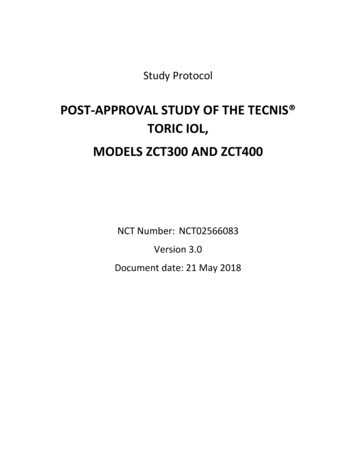
S p o ns o r e d F e a tu r e 3Figure 1. Reverse engineering and SolidWorks 3D software IOL models based on high-resolution images and direct lens measurements for the five IOLs studied.Biooptics – delivering sharp,crisp vision (2)Liliana Werner was the first to present thebio-optical properties of Clareon , andfocused on positive dysphotopsia and glaretype phenomena. IOLs can induce straylight artifacts or veiling glare into the eye(13), and Dr. Werner explained that “glareand photic phenomena can be affected bythe edge profile of the lens as well as byadditional components of the IOL (14).”Clareon has an advanced design, includinga fully usable 6 mm aspheric optic (6) andthe ‘precision edge design’ – which helpsmitigate edge glare (3,4).Dr. Werner overviewed an in vitrostudy in which Clareon was comparedwith four commercially available singlepiece hydrophobic monofocal IOLs(Eternity , Santen; enVista , Bausch Lomb; TECNIS , Johnson and JohnsonVision; and Vivinex iSert , HOYAFigure 2. Non-Sequential ray trace model eye simulation from analysis of Clareon IOLwww.alcon.com
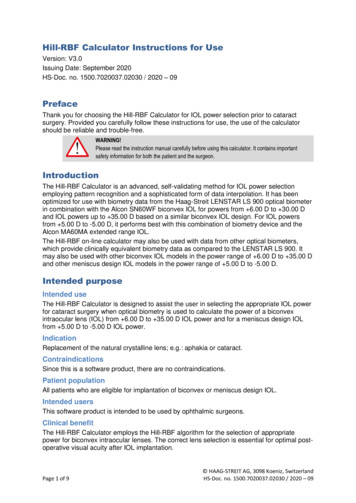
4 S p o ns o r e d F e a tu r eFigure 3. Distribution of normalized glare/main beam ratio comparison at a 550 illumination angle in vitro (n 5 IOLs per group). Evaluated in a schematic modeleye and in vitro evaluation of positive dysphotopsia or glare types photic phenomena. Optical ray trace simulations of incoming light were generated based on acollimated light source with a wavelength of 550 nm for various off-axis angles of illumination (n 5 IOLs per group, 25.0 D). The simulation analyses were verifiedusing a laboratory glare bench-top measurement system, whereby glare components formed from off-axis illumination of IOLs fitted into an artificial eye modelwere measured (15).Surgical Optics IOLs) (15). The aim ofthis study was to evaluate the photicphenomena for all these IOLs. First,SolidWorks was used to create IOLmodels for this study (Figure 1).The assessment of glare type photicphenomenon was done using a nonsequential ray trace program in aschematic model eye. The results of thesimulations were verified by an in vitroglare bench method. From model eyesimulations, Clareon was the only testedIOL that produced only focused images(Figure 2). Vivinex iSert XY1 showedfocused images similar to those observedwith the Clareon , however there wasan additional edge-transmitted glarecomponent. Both TECNIS and enVistalenses produced dispersed images andglare characteristics, whilst Eternity W-60 showed a high edge reflected glarecharacteristic, a feature that Dr. Wernerascribed as being “likely because of itssharp edge geometry.”Results from the laboratory benchimages and glare intensity profiles wereconsistent with the model eye simulationdata and verified that Clareon showedsignificantly lower glare than the othertested lenses at large angles, such as 50 and 55 angles (Figure 3) of incidence.Dr. Werner concluded that lenses withmodified anterior edge curvature, forexample, the precision edge design ofClareon , and a full optic profile withoutperipheral design features demonstratedthe lowest level – or absence – of glarecomponents over a wide range of incidentangles. Further clinical studies are neededto confirm if these differences observedin vitro are clinically significant.Biomechanics – maximizingrefractive predictabilityFollowing implantation, the mechanicalstability of IOLs can affect clinicaloutcomes. For example, axial IOLdisplacement can lead to refractiveerrors and other complications, suchas pigmentary dispersion syndrome orpupillary IOL capture. Postoperativeoptic tilt and decentration can alsobe problematic as they can affect lensperformance (16). Typically, lenses aredesigned for an average capsular sizewhich is 10 mm (17).
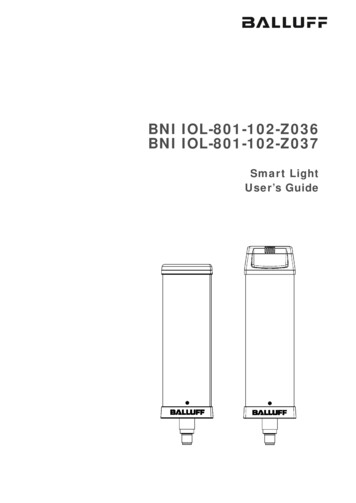
S p o ns o r e d F e a tu r e“Results verifiedthat Clareon showed significantlylower glare thanthe other testedlenses at 50 and55 anglesof incidence.”Multiple studies have shown that theAcrySof IQ monofocal IOL exhibitsexcellent IOL positioning stability andprecise centration, with consistent axiallens position and refractive outcomepredictability (18–21).Dr. Werner described a studyperformed by Dr. Stephen Lane et al.(22) that compared the Clareon IOLwith AcrySof , enVista, TECNIS, andVivinex iSert IOLs. Ten of each lens( 20.0 D) were tested in deionized waterat 35 C for axial displacement, optictilt and decentration. For assessmentsof axial displacement, lenses werecompressed to the following diameters:11.0, 10.5, 10.0, 9.5 and 9.0 mm, andthe effects of the compression on theaxial displacement and correspondingpower change were measured. Opticdecentration and optic tilt were eachmeasured at 10 mm of compression.Clareon and Acr ySof showedsignif icantly lower (P 0.001) axialdisplacement at 10 mm compression(Figure 4a) compared with all othertested lens models.When the IOLs were compressedat different diameters, Clareon andAcrySof showed the lowest axial 5a)b)Figure 4. Axial displacement at 10 mm compression (a) and axial displacement and simulated dioptricpower shifts for five compression diameters (b) of Clareon and AcrySof compared with othercommercially available monofocal IOLs. P-values for axial displacement vs. Clareon .displacement and simulated dioptricpower shifts at the corneal plane atall 5 compression diameters studied(Figure 4b).Dr. Werner showed example imagesof the lenses in their compressed(9 mm) and uncompressed states (Figure5), commenting, “You can appreciate thatsome designs have much higher axialdisplacement.”In terms of optic decentration andoptic tilt, Dr. Werner highlighted thegreat performance of all IOLs evaluated,with decentrations being within 0.06mm and tilt no greater than 1.2 for allIOLs tested (Figure 6). Mean Clareon optic decentration was found to be0.04 0.02 mm, which is lower than themaximum 0.6 mm (sum of the meanand two standard deviations) specifiedby the International Organization forStandardization (ISO; 23). Similarly,www.alcon.com
6 S p o ns o r e d F e a tu r e“Both Clareon andAcrySof lenses arevery stable andhave a similarintraocularperformance in thecapsular bag.”Figure 5. Example images of IOLs compressed at 9.0 mm overall diameter.a)Clareon was well below the maximumISO-specified value of 5 optic tilt (sumof the mean and two standard deviations;23), with a mean value of 0.5 0.2 reported in this study.Concluding her presentation, Dr.Werner noted, “Such studies areimportant because the impact of axialdisplacement and associated refractiveoutcomes on IOL selection need to beevaluated clinically, as the capsular bagchanges post-operatively.”Biomaterial – a newhydrophobic acrylicb)Figure 6. Optic decentration (a) and optic tilt (b) of all tested IOLs. P-value for optic tilt, Clareon vs. enVista.Gerd Auffarth presented the outcomesfrom in vitro evaluations of the newClareon IOL compared to TECNIS ,EnVista and Vivinex lenses (24).Prof. Auffarth tested the IOLs under‘tough’ conditions at the David J. Applelab in Heidelberg. The IOLs studiedwere subjected to an accelerated agingprocess to induce glistening formation(25). Lenses were immersed in a salinesolution at 45 C for 24 hours, beforebeing cooled to 37 C over a 2.5 hourperiod. “This may not seem like a hugetemperature difference, but it has ahuge impact on lenses,” explained Prof.Auffar th. Glistening formation was
S p o ns o r e d F e a tu r eanalyzed (at 37 C) through microscopicimaging of the center of the lens wheredata on glistening size, volume and countwere collected.All lenses displayed a low number ofglistenings. Clareon had a mean numberof 4.09 glistening microvacuoles/mm2, anumber that characterizes Clareon asGrade 0 on the Miyata glistenings scale(26). “As a lens is generally consideredglistening free if it has less than 25microvacuoles/mm2 , this means thatClareon is glistening free,” explainedProf. Auffarth. “With this acceleratedtype of testing we can say that there islittle danger that the lens will developglistenings over time.”Prof. Auffarth moved on to addresshow the new biomaterial in Clareon interacts in the eye, and describedresults from two studies in whichClareon interaction with an ophthalmicviscosurgical device (OVD) (27,28) andsilicone oil was assessed (29,30).Using ProVisc OVD no significantdifference was observed in OVD removaltimes for Clareon and AcrySof (24).For the silicone oil adhesion study, theIOLs were immersed in NaCl solution(0.9%) for 12 hours, before beingimmersed in silicone oil for 12 hoursmore (Siluron 5000, Geuder). Then,they were washed with distilled water,and examined using light microscopyto quantify the percentage of siliconeoil adhesion.T he r esul t s we r e co m pa r a blebetween the two lenses (Figure 7).“The percentage coverages obtained forClareon and AcrySof are much lowerthan what we were seeing 15 years agowith previous silicone and hydrophobicmaterial IOLs, which had around 20–25percent adhesion,” said Prof. Auffarth.“We were quite surprised how improvedthe Clareon and AcrySof materialsare in terms of their adhesion to siliconeoil, and I think that there would be noproblems with these lenses should the 7a)b)Figure 7. Silicone oil coverage of (a) AcrySof (9%) and (b) Clareon (8%) following experimentalstudies on silicone oil adhesion and removal.patient need future retinal surgery.”Prof. Auffarth also analyzed Clareon and AcrySof IOLs implanted in humanautopsy eyes with Miyake-Appleposterior view technique in order toevaluate the behavior of these two lensesin the capsular bag (24). They showedthat both the Clareon and AcrySof lenses are very stable and have a similarintraocular performance in the capsularbag, with Clareon showing a slightlylarger arc of contact and less pronouncedstriae and ovalization.Prof. Auf far th summarized thepresentation, stating that the Clareon biomaterial has an ex tremely lowincidence of glistenings, and comparesfavorably with the AcrySof lens in termsof OVD removal time, silicone oil adhesionand intraocular capsular bag performance.Clinical experience withimplanting the Clareon IOLRudy Nuijts began implanting Clareon lenses in patients in July 2017, and sharedthe Maastricht University Eye Clinic’ssurgical experience with the new lens in acohort of 99 eyes (69 patients). Reflectingon their experiences with Clareon lenshandling compared with the AcrySof ,Prof. Nuijts said, “We found that the IOLhandles less ‘stiffly’ during the cartridgemanipulation and loading, and there is aquicker unfolding of the optic and hapticsin the eye.” He added, “There was alsowww.alcon.com
8 S p o ns o r e d F e a tu r eBox 2 – Case Study ofClareon Implantation 80 year old female withdecreased OD vision (CDVA 1.50 -0.25x 54 : 0.6) Slit lamp examination showedcortical cataract 2 OD Prediction for SRK/TA-constant:o 119.1 0.29 Do 119.2 0.37 D Clareon was implantedin the right eye ( 21 D)through a 2.2 mm incisionless ‘stickiness’ of the haptics on theoptic, as you can sometimes see with theAcrySof .” Based on Prof. Nuijts’s earlyexperience they identified a four seconddifference in unfolding time between theClareon and AcrySof lenses (30 [ 13.5] seconds vs. 34 [ 15.7] seconds,respectively). Prof. Nuijts stated that theunfolding time of other commerciallyavailable hydrophobic lenses has beenshown to range between 30 and120 seconds.Turning to clinical outcomes followingClareon implantation, Prof. Nuijtsnoted that their studies were basedon an academic cohort rather than aselective clinical study population: 31of 99 eyes had comorbidities, includingage-related macular degeneration(AMD), brunescent/mature cataract, highmyopia, amblyopia and Fuch’s endothelialdystrophy; and four of these 31 eyeshad received prior radial keratotomy orLASIK. One month after Clareon IOLimplantation, 100 % of eyes (n 40) hada monocular corrected distance visualacuity (CDVA) greater than 20/40, and64.3 % had a CDVA greater than 20/20. Postoperative results wereas follows:o Day 1 – CDVA ( 0.50 D): 0.6o Week 1 – UDVA 1.0o Month 1 – UDVA 1.2 Slit lamp examination showedclear pseudophakia“We were very pleased with these goodvisual outcomes, especially consideringthat one third of the eyes in our cohorthad comorbidities,” said Prof. Nuijts. Anexample of a routine cataract case canbe seen in Box 2.Prof. Nuijts concluded that Clareon has a shor ter unfolding time thanAcr ySof , and that the estimated
S p o ns o r e d F e a tu r eBox 3 – Key Featuresof AutonoMe (2)A-constant for Clareon is 119.1 –which simply involves adding 0.2 to thepersonalized AcrySof IQ A-constant.Prof. Nuijts also highlighted: “We haveseen no surface haze or glistenings in thisearly post-operative period.”AutonoMe IOL DeliverySystem - An automatedapproach to delivery“AutonoMe (Box 3) is the first andonly automated, disposable, pre-loadeddelivery system in the ophthalmology Single-use Innovative, automated lensadvancement with the use ofthe speed-controlled levermarket,” said Dr. Lane.AutonoMe is the next evolution ofIOL delivery advancements from Alcon,following a series of innovative designsincluding the MONARCH series ofinjectors and pre-loaded injectors, such asthe AcrySert and Ultrasert (Figure 8).The key feature that sets AutonoMe devices apart is the delivery controlmechanism (31, 32), which has evolvedfrom the screw-type mechanism of theMONARCH devices and the syringetype system in the UltraSert (wherepressure is exerted by the surgeon) to 9 IOL delivery speed up to 3.0 mm/s Length: 16.51 cm Outer diameter: 15.24 mmthe automated lever delivery system inAutonoMe , which features an innovativeCO2-powered delivery mechanism (2).“It’s actually a pretty simple system,” saidDr. Lane. “The CO2 cartridge is really whatprovides the mechanism for automatedlens advancement, as it provides thepower to move the piston down the shaftand deliver the lens.” Delivery speed iscontrolled by a responsive speed controllever; the surgeon only needs to useone fingertip as speed is determinedby the level of depression, meaningthat the second hand can remain freewww.alcon.com
10 S p o ns o r e d F e a tu r eFigure 8. Timeline of Alcon IOL delivery advancements.during lens delivery to stabilize the eyeif needed. The CO2-powered deliverymechanism also enables precise plungeradvancement, as well as consistent IOLfolding and delivery into the capsularbag (32).Dr. Lane summarized the preparationsteps (2) with the device (see Box 4– Using AutonoMe ) and highlightedthe three pillars to take away from theinnovative AutonoMe system. “Firstly,it is very easy to use (31),” he said. “Itallows single-handed delivery, and utilizesa very innovative, automated deliverysystem with a CO2-powered cartridgeand responsive speed control lever thatallows the surgeon to stop or start – andvary the speed of – the delivery.” Thesecond pillar relates to the intuitive (31)and ergonomic nature of AutonoMe . “Itis designed for comfortable, ergonomichand positions,” he said. “It is not a ‘onetype fits all’ situation – the surgeon canadapt the device to his or her particulartechnique.” The third pillar is related tocontrol (32): “All surgeons like controlthroughout all phases of the surgery, andAutonoMe enables precise deliveryinto the capsular bag, whilst protectingincisions as small as 2.2 mm and providingfull IOL visibility during the delivery.”Dr. Lane concluded that “The Clareon AutonoMe delivers the ultimate IOLinsertion experience which I believe willchange the way we deliver IOLs into theeye”. “It is the first and only automateddisposable pre-loaded delivery devicethat is easy and intuitive (31,32) – andallows for predictable IOL delivery ofa true and pristine premium IOL witha new hydrophobic biomaterial andadvanced manufacturing process thatachieves – along with the precision edgedesign – unsurpassed optical clarity.”(3, 9-12)6.Imaging of the Usable Optic Diameter ofClareon SY60WF, TECNIS ZCB00, andenVista MX60 IOLs. Alcon internal technicalreport: TDOC-0053803, effective July 12,2017.7.Clareon SY60WF Axial Displacement Studyat Varied Compressions. Alcon internaltechnical report: TDOC-0054028, effectiveJuly 11, 2017.8.L Werner and N Mamalis. Evaluation of IOLpositioning stability and ocular biocompatibilityof a new IOL material in the rabbit cataractsurgery model (University of Utah) – InterimReport.9.Microvacuole Evaluation of Clareon andOther Marketed IOLs. Alcon internal report:References1.Alcon. “Alcon flagship AcrySof intraocular lensreaches 100 million implants and counting”.Available at: http://bit.ly/2hqAnYT. AccessedOctober 31, 2017TDOC-0053516, effective February 28, 2017.10. Clareon and Marketed IOL Slit Lamp SurfaceHaze. Alcon internal technical report:TDOC-0053487, effective February 28, 2017.11. Clareon and Marketed IOL Nidek Surface2.Clareon AutonoMe Directions for Use.Scatter and Bulk Haze. Alcon internal technical3.Improved Milled Edge Quality of Clareon report: TDOC-0053488, effective FebruaryIOLs. Alcon internal technical report:TDOC-0053598, effective March 13, 2017.4.Schematic Model Eye and In Vitro Evaluationof Positive Dysphotopsia or Glare Types PhoticPhenomena. Alcon internal technical report:5.28, 2017.12. Elimination of Clareon IOL Surface HazeSummary. Alcon internal technical reportTDOC-0053072, effective 05-Jan-201713. G Labuz et al., “Straylight from glistenings inTDOC-0053578, effective August 8, 2017.intraocular lenses: In vitro study”, J CataractAcrySof IQ IOL Directions for UseRefract Surg, 43, 102–108 (2017). PMID:
S p o ns o r e d F e a tu r e 11Box 4 – Using AutonoMe (2)Consult the Clareon AutonoMe DFU (2) for complete preparation and delivery inspection, as well as a list of Alcon-qualified viscoelastics28317662.14. JA Davison. “Positive and negativedysphotopsia in patients with acrylicintraocular lenses”, J Cataract Refract Surg, 26,1346–1355 (2000). PMID: 11020620.15. L Werner et al. “Model eye and in vitroand 3-piece hydrophobic acrylic foldable1529–1534 (2013). PMID: 23926419.intraocular lenses”, Ophthalmology, 113,26. A Miyata et al., “Clinical and experimental585–590 (2006). PMID: 1658142021. SS Lane et al., “Comparison of thebiomechanical behavior of foldable intraocularlenses”, J Cataract Refract Surg, 30,assessment of positive dysphotopsia or glare2397–2402 (2004). PMID: 15519095.types photic phenomena: a comparison of a22. SS Lane et al. “Evaluation of the mechanicalobservation of glistening in acrylic intraocularlenses”, Jpn J Ophthalmol, 45, 564–569(2001). PMID: 11754896.27. GU Auffarth et al., “Removal times andtechniques of a viscoadaptive ophthalmicviscosurgical device”, J Cataract Refract Surg,new material IOL to other monofocalbehavior of a new single-piece intraocular lensintraocular lenses”. Presentation at theas compared to commercially available IOLs”.European Society of Cataract and RefractivePresentation at the European Society ofdispersive and a cohesive ophthalmicSurgeons (ESCRS) annual meeting; OctoberCataract and Refractive Surgeons (ESCRS)viscosurgical device correlated with7–11, 2017; Lisbon, Portugal.annual meeting; October 7–11, 2017; Lisbon,intraocular lens material”, J Cataract RefractPortugal.Surg, 30, 2410–2414 (2004). PMID:16. O Findl et al., “Capsular bag performance of ahydrophobic acrylic 1-piece intraocular lens”, J23. International Organization for StandardizationCataract Refract Surg, 41, 90–97 (2015).(ISO). “Standard ISO 11979-3:2012(en)PMID: 25454363.Ophthalmic implants — Intraocular lenses17. A Vasavada et al, “Relationship between lensand capsular bag size”, J Cataract Refract Surg.24: 547–551, (1998). PMID: 9584254.18. JJ Koshy et al., “Rotational stability of a— Part 3: Mechanical properties and testmethods”. Available at: http://bit.ly/2zTkjFC.Accessed October 31, 2017.24. G Auffarth et al. “Laboratory evaluation of thesingle-piece toric acrylic intraocular lens”, Jnew CLAREON hydrophobic acrylic IOLCataract Refract Surg, 36, 1665–1670 (2010).material: biomaterial properties and capsularPMID: 24332372.bag behavior”. Presentation at the European19. MG Wirtitsch et al., “Effect of haptic design onchange in axial lens position after cataractsurgery”, J Cataract Refract Surg, 30, 45–51(2004). PMID: 1496726720. R Nejima et al., “Prospective intrapatientcomparison of 6.0-millimeter optic single-pieceSociety of Cataract and Refractive Surgeons(ESCRS) annual meeting; October 7–11, 2017;Lisbon, Portugal.25. BE Thomes and TA Callaghan. “Evaluation of30, 879–883 (2004). PMID: 15093655.28. GU Auffarth et al., “Removal times for a15519097.29. SN Arthur et al., “Silicon oil adherence tosilicone oil intraocular lenses”, Int OphthalmolClin, 41, 33–45 (2001). PMID: 11481538.30. SN Arthur et al., “Effect of heparin surfacemodification in reducing silicone oil adherenceto various intraocular lenses”, J CataractRefract Surg, 27, 1662–1669 (2001). PMID:11687368.31. Nozzle Preference and Delivery SystemPerformance Study between AutonoMe andUltraSert V3.5. Alcon internal technicalreport: TDOC-0053876, effective 11 July 2017.32. Verification Report, IOL Inserter Plunger Speedin vitro glistening formation in hydrophobicTesting. Alcon internal document. Approved 15acrylic intraocular lenses”, Clin Ophthalmol, 7,March 2017.www.alcon.com
AM-17-MK-SUPPL-001
(13), and Dr. Werner explained that "glare and photic phenomena can be affected by the edge profile of the lens as well as by additional components of the IOL (14)." Clareon has an advanced design, including a fully usable 6 mm aspheric optic (6) and the 'precision edge design' - which helps mitigate edge glare (3,4).