Transcription
Sponsored byExtending Vision with AcrySof IQ Vivity IOL,the First and Only Extended Depth of Focus (EDoF)IOL with the Wavefront-ShapingX-WAVE technologyReal-world perspectives and clinical experience fromthe AcrySof IQ Vivity Users Experience MeetingOctober 2020We would like to thank the following advisors for submitting cases studies and contributing tothis valuable discussion:A/Prof. Chandra Bala (Co-chair)Dr. Michael LawlessPersonalEyes, and Macquarie University,Sydney, AustraliaVision Eye Institute and University ofSydney, AustraliaDr. Kjell Gunnar Gundersen (Co-chair)Dr. Francesco CaronesIfocus Øyeklinikk AS,Haugesund, NorwayCarones Ophthalmology Center,Milan, ItalyProf. Thomas KohnenDr. Edoardo LigabueGoethe University,Frankfurt am Main, GermanyOphthalmology Department, CentroDiagnostico Italiano, Milan, ItalyDr. Merce GuarroProf. Rosa Braga-Mele*Valles Oftalmologia Recerca,Barcelona, SpainFaculty of Medicine, University ofToronto, Canada* Was unable to attend the meeting but contributed in a follow-up teleconference.This supplement solely reflects the views, opinions, and clinical practice experiences of presenters who participated in the AcrySof IQ Vivity Users ExperienceMeeting in October 2020. Data presented are representative of each participating surgeon’s own experience and do not arise from formal clinical studies.
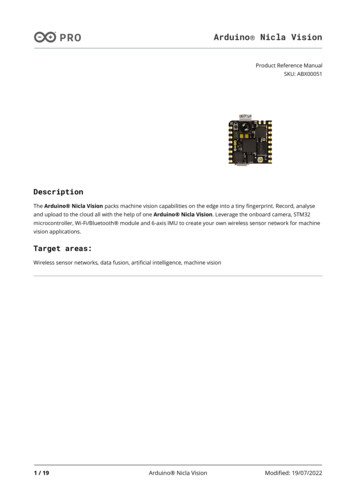
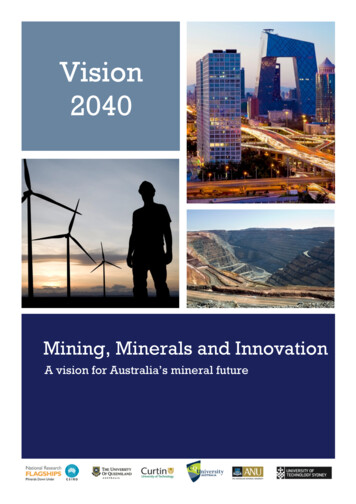
AcrySof IQ Vivity answers thecall for continuous range of vision,with an aspheric monofocal visualdisturbance profileCataract surgery is one of the most frequentlyperformed procedures worldwide, involving theremoval of the opacified natural crystalline lens andsubsequent replacement with an intraocular lens(IOL).1 Traditional IOLs are monofocal and typicallyfocused on distance vision.2,3 However, becausepresbyopia is the most common refractive disorder inpeople over 40 years of age,4 there is a need for IOLsthat offer improved near and intermediate vision.Presbyopia-correcting IOLs have been developed withthe aim of mitigating the effects of presbyopia. Earlyexamples of multifocal IOLs were designed to improvedistance and near vision; more recently, there hasbeen increasing demand for improved intermediatevision to accommodate patients’ needs, such as drivingand technical device use.5 Trifocal IOLs have soughtto bridge this gap by offering improved vision atintermediate distances.5 Several technologies in thiscategory have been employed, including refractiveand diffractive lens optics, but many are associatedwith photic phenomena (such as glare and halo) andreduced contrast sensitivity,3,6 thus compromisingpatients’ quality of life. Extended depth of focus (EDoF) IOLsFigure 1: Introduction toAcrySof IQ Vivity AcrySof IQ Vivity IOL is the Firstand Only Extended Depth of Focus(EDoF) IOL with the Wavefront-ShapingX-WAVE technology Intended benefit: continuousextended range of vision* with anaspheric monofocal visualdisturbance profile (AcrySof IQ)AcrySof IQ Vivity X-WAVE technology(central 2.2 mm) Stretches and shiftsthe wavefront Avoids light splitting Results in an extendedfocal range rather thanmultiple focal pointsLight intensity distribution†DistanceIntermediateNearAcrySof IQMonofocalSymfony‡DiffractiveAT LARA‡DIffractiveAcrySof IQ Vivity X-WAVE TechnologyExtended focal rangeArea of precisely focused lightHalo hnologyAcrySof IQAcrySof IQ Vivity X-WAVE TechnologyDiffractive technologyAcrySof IQ base power7 magnification of central element for illustrative purposesSymfony‡AT LARA‡*AcrySof IQ Vivity demonstrated a mean monocular negative range of focus at 0.2 logMAR of 1.53 D compared to 0.99 D for the monofocal controlIOL; †Simulated photopic through-focus point spread function (light intensity [energy]) – polychromatic; ‡Trademarks are the property of their respectiveowners; §Optical bench data of pinhole images to simulate halo effects (logarithmic scale images of halos around point source).IOL, intraocular lens.
were intended to provide extended range of visionwithout the typical visual disturbances associatedwith diffractive trifocal and bifocal technologies.5However, many EDoF IOLs are still associated withphotic phenomena and reduced contrast sensitivity;2and so, despite the numerous IOL options available tosurgeons and patients, distinct unmet needs remain.4AcrySof IQ Vivity IOL is the First and Only ExtendedDepth of Focus (EDoF) IOL with the Wavefront-ShapingX-WAVE technology. It provides patients with acontinuous extended range of vision from distanceto functional near, thereby reducing their need forspectacles. X-WAVE technology stretches and shiftsthe wavefront rather than splitting it. This means itcan utilize almost all of the light, like a monofocal, andhence has an aspheric monofocal visual disturbanceprofile, while the uniform light intensity distributiongives “more natural vision” (see Figure 1).7–11of experts shared their clinical evidence andpractice insights through case studies in key patientpopulations that may be particularly suited toreceiving AcrySof IQ Vivity ; these included thosetargeted for mini-monovision, post-laser-assisted insitu keratomileusis (LASIK) patients, and patients withmild glaucoma. Highlights of the discussion can befound in Figure 2.Figure 2: Key highlights from theAcrySof IQ Vivity Users Experience MeetingAcrySof IQ Vivity provides very gooddistance and intermediate vision, good nearvision, and an excellent visual disturbanceprofile that is similar to a monofocal IOLSeveral of the group described AcrySof IQ Vivity as their “default lens,” saying it is difficult to findreasons not to use it, including in patients withocular pathologiesGlobal perspectives on thereal-world use of AcrySof IQ Vivity :Helping to translate clinicaldata to practiceRegulatory approval of IOLs in various countries oftenrequires a research study (ie, clinical trial), in whichparticipants are prospectively assigned to one or moreinterventions to evaluate safety and performanceof the IOL. These results are usually compared witha concurrent control group and, collectively, thisevidence forms the basis for supporting the safety andeffectiveness of the device. Although these controlledstudies provide a useful baseline for understandingthe safety and performance of an IOL, clinical trials cansometimes be narrow in scope due to their practicalchallenges and carefully controlled target populations.Hence, case series utilizing real-world data cancomplement this evidence by providing informationon a wider patient population that cannot be obtainedthrough a traditional registration clinical trial alone.In early October 2020, Alcon brought togetherkey thought leaders in ophthalmology from Europe,Australia, and Canada to discuss their real-worldexperience with AcrySof IQ Vivity . This groupPreliminary clinical experience data gathered fromour patient cases suggest AcrySof IQ Vivity could be a great IOL choice for mini-monovision,and potentially post-LASIK and mild glaucomapatients*AcrySof IQ Vivity is a “forgiving lens” interms of refractive error and targeting, whichmakes it an optimal choice when consideringmini-monovision for patientsPreliminary clinical experience is favorable but more data willbe needed to confirm this in a larger population.*IOL, intraocular lens; LASIK, laser-assisted in situ keratomileusis.Several of the group describedVivity as their “default lens,”saying it is difficult to findreasons not to use it.A/Prof. Chandra Bala, PersonalEyes, and Macquarie University, Sydney,Australia and Dr. Michael Lawless, Vision Eye Institute and University ofSydney, Australia.
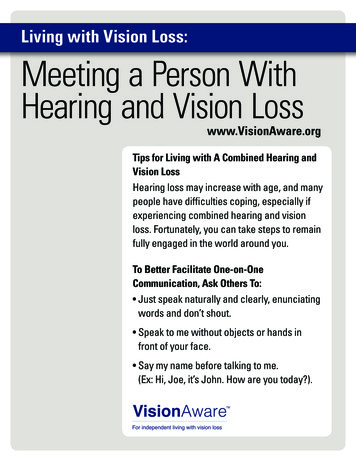
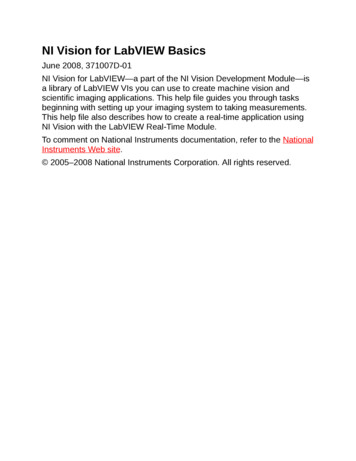
AcrySof IQ Vivity is a “forgiving” IOLwith versatile applications in differenttarget populationsReal-world insights reveal thatAcrySof IQ Vivity is a versatilelens that surgeons consider to bea go-to lensThe group agreed that AcrySof IQ Vivity providesexcellent distance visual acuity, with extended rangeof vision to intermediate and functional near,Figure 3: Binocular mean photopic correctedand uncorrected visual acuity at Month 6 forAcrySof IQ Vivity from the US registrationstudy*8 91.6% of AcrySof IQ Vivity patients (first eyes)achieved MRSE within 0.5 D of emmetropia†Patients (N)106Binocular VAMean logMAR (SD)BCDVA-0.028 (0.084)UCDVA0.035 (0.102)DCIVA0.054 (0.093)UCIVA0.058 (0.083)DCNVA0.253 (0.118)UCNVA0.208 (0.104)*Visual acuities were measured at distance, intermediate (66 cm), andnear (40 cm); †Surgeons were instructed to select the lens power thattargeted emmetropia (closest to 0.0 D) and mean SD MRSE in first eyesat 6 months was 0.049 0.345 D for AcrySof IQ Vivity .BCDVA, best-corrected distance visual acuity; D, diopters;DCIVA, distance-corrected intermediate visual acuity;DCNVA, distance-corrected near visual acuity; logMAR, logarithm ofthe minimum angle of resolution; MRSE, manifest refraction sphericalequivalent; SD, standard deviation; UCDVA, uncorrected distancevisual acuity; UCIVA, uncorrected intermediate visual acuity;UCNVA, uncorrected near visual acuity; VA, visual acuity.combined with a visual disturbance profile similar tothat of a monofocal lens. Personal clinical experienceof using AcrySof IQ Vivity that was discussed duringthe meeting reflected the results of a registrationstudy carried out in the United States (US), whichdemonstrated excellent distance, intermediate, andfunctional near visual acuities for AcrySof IQ Vivity (see Figure 3).8,10 AcrySof IQ Vivity was alsodescribed as the default lens for many, even in thepresence of eye pathologies (see Figure 4).AcrySof IQ Vivity is a “forgiving”lens that can tolerate residualrefractive errorAcrySof IQ Vivity was described as a “forgiving”lens because patients could tolerate some residualrefractive error, which encouraged many of the groupto feel confident in adopting a mini-monovisionapproach with patients. Additionally, it was arguedthat the “forgiving” attributes of AcrySof IQ Vivity could benefit post-LASIK patients, in whom IOLcalculations may be difficult.Vivity provides excellentdistance visual acuity, withextended range of visionto intermediate and functionalnear, combined with anaspheric monofocal visualdisturbance profile.Dr. Francesco Carones, Carones Ophthalmology Center, Milan, Italy.
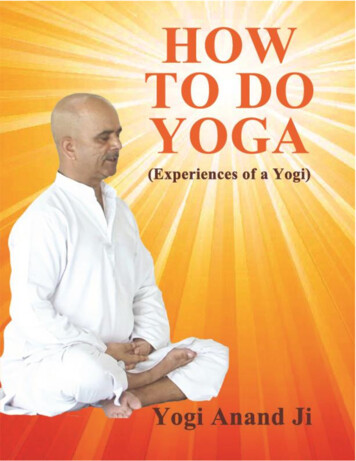
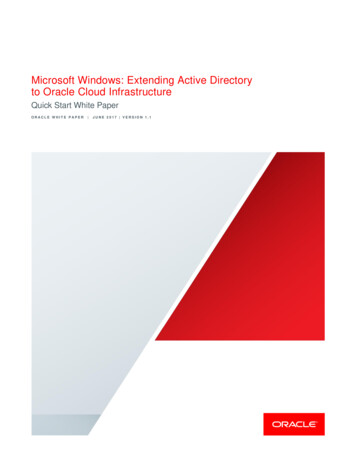
Mini-monovision usingAcrySof IQ Vivity Figure 4: AcrySof IQ Vivity withWavefront-Shaping X-WAVE technologypotentially expands the patient populationfor presbyopia correctionExcellent mini-monovision outcomesachieved with AcrySof IQ Vivity The US registration study demonstrated thatAcrySof IQ Vivity extends the range of vision,with improved intermediate and functional nearvisual acuity compared with a monofocal control.*9Although the US registration trial was limited totargeting emmetropia, many in this users experiencemeeting have utilized a mini-monovision approachwith AcrySof IQ Vivity to enhance the benefit of theWavefront-Shaping X-WAVE technology and extendtheir patients’ vision further into the near range, whilemaintaining monofocal-quality distance visual acuity.Clinical experience from three surgeons’ case series,including 62 patients in total, demonstrated that amini-monovision approach using AcrySof IQ Vivity resulted in excellent distance to near visual acuity(see Figure 5). Furthermore, patient satisfaction, asobserved by the surgeons in their routine clinicalpractice, was reported to be high, with no visualdisturbances or night vision problems reported in themajority of patients. Spectacle independence has alsobeen reported to be high (see Figure 6), although itwas noted that it cannot be guaranteed; reading booksor newspapers, especially in dim light, or activitiesinvolving delicate hand–eye coordination may requirespectacle use in some patients (see Figure 6). Surgeonsreported usingAcrySof IQ Vivity in a wide varietyof patientpopulations:Patients withpreviousophthalmologicalsurgery†: Post-refractivesurgery Post-hyperopicLASIK Post-myopic LASIKPatients with underlyingpathologies/conditions†: Mild glaucoma Diabetes mellitus Mild evaporative DED Migraine Keratoconus Dry macular disease Amblyopia Mild MDF corneal dystrophy Light maculopathy Wet age-related macular degeneration Asteroid hyalosisPatients with various IOLoutcomes (planned/unplanned): Mini-monovision Mix and match (with monofocals) Decentration (high κ angle) Refractive error toleranceThe safety and effectiveness of AcrySof IQ Vivity has not beensubstantiated in clinical trials in patients with certain pre-existingconditions and/or intraoperative conditions, including uncontrolledglaucoma or previous refractive surgery, as these patients wereexcluded from the clinical studies. 8,9†DED, dry eye disease; IOL, intraocular lens; κ angle, angle kappa;LASIK, laser-assisted in situ keratomileusis; MDF, map-dot-fingerprint.*AcrySof IQ Vivity provided mean photopic monoculardistance-corrected intermediate visual acuity and distance-correctednear visual acuity superior to the monofocal control IOL.Figure 5: AcrySof IQ Vivity provides excellent visual acuity across distances for patients targetedfor mini-monovisionBinocular uncorrected VAs in patients with pristine eyes targeted for mini-monovisionPatients (n)Mean target MRSE (non-dominant)VAUCDVAUCIVAUCNVADr. Carones20-0.47 DBinocular (mean logMAR)-0.080.00 (60 cm)0.05 (45 cm)Prof. Bala20-0.58 DBinocular (mean logMAR)-0.040.01 (60 cm)0.04 (40 cm)Dr. Gundersen22-0.35 DBinocular (mean logMAR)-0.040.00 (100 cm)0.01 (50 cm)All eyes were within 0.50 D of target MRSED, diopters; logMAR, logarithm of the minimum angle of resolution; MRSE, manifest refraction spherical equivalent; UCDVA, uncorrected distancevisual acuity; UCIVA, uncorrected intermediate visual acuity; UCNVA, uncorrected near visual acuity; VA, visual acuity.
Figure 6: In patients with pristine eyes, mini-monovision using AcrySof IQ Vivity yields high spectacleindependence (consecutive case series; n 20*)How often do you use spectacles or contact lenses? (Month 3)SportsTVDay drivingNight drivingWatch otosRead newsRead bookRead in the en80%90%100%Always*Spectacle independence data from Dr. Carones, collected in their routine clinical practice.Figure 7: Opinion point: Is this mini-monovisionwith AcrySof IQ Vivity ?Monovision using traditional monofocal IOLscorrects distance vision in the dominant eye,while the non-dominant eye focuses intentionallyon near to mid-range vision.12 “Mini-monovision”requires a smaller interocular refractive errordifference than traditional monovision, buttypically still in the range of -0.75 and -1.75 D.12With the extended vision gained from AcrySof IQ Vivity ,an even smaller difference between the eyes(-0.25 D to -0.75 D for the non-dominant eye) couldbe used to achieve sufficient near vision for somepatients, and each eye provides a range of focusin itself, which would potentially increase withbinocular summation.Considering that the patient will not likelyperceive a difference between their eyes,the group argued that more patients couldtolerate this approach and that the lens will givepatients “more natural vision.”Small refractive offsets can makebig visual improvements withAcrySof IQ Vivity Some of the surgeons reported that they have usedAcrySof IQ Vivity successfully for mini-monovision, witha refractive target between -0.25 D and -0.75 D for thenon-dominant eye bolstering success. The experienceusing mini-monovision with AcrySof IQ Vivity extendsto patients with an array of ocular pathologies, whoalso stand to benefit from similar outcomes, such aspatients with map-dot-fingerprint corneal dystrophy,asteroid hyalosis, dry macular disease, keratoconus, mildamblyopia, glaucoma, post-LASIK correction (myopiaand hyperopia), diabetes, and light maculopathy. However,the group also considered whether the term “minimonovision” was appropriate for AcrySof IQ Vivity , orif it should be considered a new treatment paradigm forpresbyopia correction (see Figure 7).12Perhaps it’s time for new terminology?Vivity was described as a“forgiving” lens becausepatients could tolerate someresidual refractive error, whichencouraged many of the groupto feel confident in adopting amini-monovision approach.D, diopters; IOL, intraocular lens.Dr. Merce Guarro, Valles Oftalmologia Recerca, Barcelona, Spain.
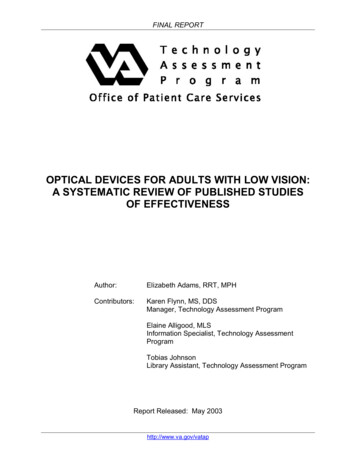
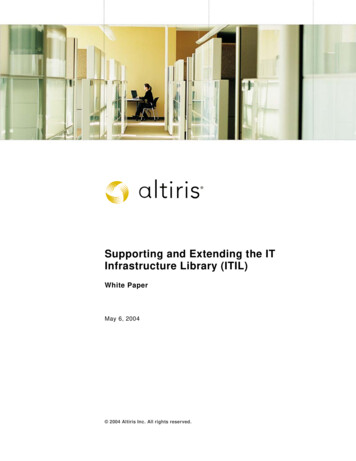
Using AcrySof IQ Vivity in post-LASIK eyesPreliminary clinical experience withAcrySof IQ Vivity in post-LASIKeyes shows early promisePost-LASIK patients are typically more challenging totreat, given the difficulty of IOL power calculationsinherent in the post-LASIK eye due to alterations inthe cornea.13 Furthermore, these patients have highexpectations of treatment and are keen to protecttheir investment in LASIK by retaining or restoringfreedom from spectacle use.13,14 Despite this,promising results have been observed in the limitednumber of post-LASIK patients who have receivedAcrySof IQ Vivity (see Figure 8).Although these early results suggest thatAcrySof IQ Vivity is an appropriate lens for myopicand hyperopic post-LASIK eyes, success is likely todepend on the degree of corneal irregularities inthe post-LASIK eye. Further studies are requiredFigure 8: Preliminary visual acuity data atdistance, intermediate and near in post-LASIKeyes implanted with AcrySof IQ Vivity to determine the types of corneal irregularitiesthat AcrySof IQ Vivity can tolerate, including safethresholds for coma and other higher order aberrations.Using AcrySof IQ Vivity in patients withglaucomaInitial clinical experience inpatients with preperimetric andmild glaucomaBoth glaucoma and cataract are common causes ofblindness worldwide, and frequently coexist in theelderly population.15 Therefore, it was of particularinterest to understand how AcrySof IQ Vivity performs in patients with glaucoma. Initial experiencefrom 2 patient cases shows both cases achieved goodvisual outcomes at all distances (see Figure 9).Another consideration in glaucoma patients iscontrast sensitivity, which has been suggested in thistarget population to be linked to subjective complaintsFigure 9: Visual acuity data fromindividual patients with preperimetricor mild glaucoma (n 2)Binocular uncorrected VAsMean VA (logMAR)-0.16Myopic(n 3*)Myopic(n 1†)-0.12–0.08-0.08-0.040.00Hyperopic(n 1*)0.00 0.000.00 0.000.00 0.000.04All eyes werewithin 0.50 Dof target arTarget MRSE in non-dominant eye was approximately -0.5 D.*Dr. Carones’s patient cases, with VA measured at distance,intermediate (60 cm), and near (45 cm); †Prof. Braga-Mele’s case study,with VA measured at distance, intermediate (60 cm), and near (40 cm).D, diopters; LASIK, laser-assisted in situ keratomileusis; logMAR,logarithm of the minimum angle of resolution; MRSE, manifestrefraction spherical equivalent; VA, visual acuity.Mean VA (logMAR)-0.20Binocular uncorrected .080.100.12Preperimetric(n 1*)0.00 0.00Mild(n 1†)0.00 0.000.050.10DistanceIntermediateNear*Dr. Gundersen’s case study, with VA measured at distance, intermediate(100 cm), and near (50 cm); †Prof. Kohnen’s case study, with VA measuredat distance, intermediate (66 cm), and near (40 cm).LogMAR, logarithm of the minimum angle of resolution; VA, visual acuity.
of blurred vision.16 In the US registration study,reported outcomes in AcrySof IQ Vivity patients(albeit without ocular comorbidities) were similar orbetter than monofocal controls for hazy and blurredvision, despite observed reductions in monocularmesopic contrast sensitivity with increasing spatialfrequency.*8,9 It would be important to study thisfurther and understand if glaucoma patients reportsimilar results.On reflection of the available data, the group agreedthat AcrySof IQ Vivity could be considered in patientswith preperimetric and mild glaucoma. However, furtherresearch is required to determine the performance ofAcrySof IQ Vivity in individuals with glaucoma.*The proportion of patients who reported that they did not experiencehazy vision was 88.6% and 86.5% for AcrySof IQ Vivity and monofocal,respectively (95% CI -7.2, 11.3). Significantly more AcrySof IQ Vivity patients (90.6%) than monofocal patients (80.2%) reported that they didnot experience blurred vision (95% CI 0.6, 20.1).9SummaryAcrySof IQ Vivity IOL is the First and OnlyExtended Depth of Focus (EDoF) IOL with theWavefront-Shaping X-WAVE technology, whichprovides a continuous extended range of vision fromdistance to functional near, reduces patients’ relianceon spectacles, and has an aspheric monofocal visualdisturbance profile. Early clinical experience suggeststhat AcrySof IQ Vivity is a versatile technology thatcan be used in pristine eyes, as well as those withcertain ocular pathologies. As clinical experienceand confidence in the IOL grows, surgeons maygradually expand their use of AcrySof IQ Vivity toother patient groups. In the meantime, Alcon remainscommitted to ongoing research to help guide howbest to use AcrySof IQ Vivity in practice.Based on initial observations of these real-lifepatient cases:A mini-monovisionapproach usingVivity resulted in excellentdistance to near visual acuity,with no visual disturbances ornight vision problems reportedin the majority of patients.Mini-monovision: AcrySof IQ Vivity was considered a great choice formini-monovision by advisorsPost-LASIK: Many surgeons have extendedthe application of AcrySof IQ Vivity topost-LASIK eyesGlaucoma: AcrySof IQ Vivity may beconsidered for patients with preperimetricor mild glaucomaDr. Kjell Gunnar Gundersen, Ifocus Øyeklinikk AS, Haugesund, Norway.References1.2.Davis G. The evolution of cataract surgery. Mo Med 2016;113:58–62.Liu J, Dong Y, Wang Y. Efficacy and safety of extended depth of focusintraocular lenses in cataract surgery: a systematic review andmeta-analysis. BMC Ophthalmol 2019;19:198.3. de Silva SR, Evans JR, Kirthi V et al. Multifocal versus monofocalintraocular lenses after cataract extraction. Cochrane Database SystRev 2016;12:CD003169.4. Davidson RS, Dhaliwal D, Hamilton DR et al. Surgical correction ofpresbyopia. J Cataract Refract Surg 2016;42:920–930.5. Kondylis G, Klavdianou O, Sotiria P. Multifocal and extended depthof focus intraocular lenses. Ann Eye Sci 2019;4:5.6. Rocha KM. Extended depth of focus IOLs: the next chapter inrefractive technology? J Refract Surg 2017;33:146–149.7. Kohnen T. Nondiffractive wavefront-shaping extended range-ofvision intraocular lens. J Cataract Refract Surg 2020;46:1312–1313.8. Alcon Research LLC. AcrySof IQ Vivity product information(US version). Available at: https://ifu.alcon.com.[accessed 11 Feb 2021].9. Alcon Research LLC. AcrySof IQ Vivity product information(UK version). Available at: https://ifu.alcon.com.[accessed 11 Feb 2021].10. McCabe C, Martinez A. Visual outcomes and patient satisfactionafter implantation of a new non-diffractive presbyopia-correcting11.12.13.14.15.16.intraocular lens. 38th Congress of the European Society of Cataractand Refractive Surgeons. Virtual, 2–4 Oct 2020. Oral presentation.Schwiegerling JT, Carson DR, Choi M et al. Optical simulation andbench data of a non-diffractive intraocular lens designed to extenddepth of focus and minimize visual disturbances. Annual Meeting ofthe American Society of Cataract and Refractive Surgery. San Diego,USA, 3–7 May 2019. Oral presentation.Goldberg DG, Goldberg MH, Shah R et al. Pseudophakicmini-monovision: high patient satisfaction, reduced spectacledependence, and low cost. BMC Ophthalmol 2018;18:293.Chang DC, Lawless M, Fracs F, Raviv T. Cataract surgery in patientsafter high myopic LASIK. Cataract & Refractive Surgery Today. 2019.Available at: act-surgery-in-patients-after-high-myopic-lasik/ [accessed9 Nov 2020].Raviv T. Choosing an IOL after LASIK. Cataract & Refractive SurgeryToday. Available at: -iol-after-lasik/ [accessed 9 Nov 2020].Melancia D, Abegao Pinto L, Marques-Neves C. Cataract surgery andintraocular pressure. Ophthalmic Res 2015;53:141–148.Hu CX, Zangalli C, Hsieh M et al. What do patients with glaucoma see?Visual symptoms reported by patients with glaucoma. Am J Med Sci2014;348:403–409. 2021 Alcon Inc. 3/21 GLB-VIV-2100004
could benefit post-LASIK patients, in whom IOL calculations may be difficult. Figure 3: Binocular mean photopic corrected and uncorrected visual acuity at Month 6 for AcrySof IQ Vivity from the US registration study*8 91.6% of AcrySof IQ Vivity patients (first eyes) achieved MRSE within 0.5 D of emmetropia† Patients (N) 106