Transcription
POLICY AND GUIDELINETOMAH MEMORIAL HOSPITAL/TOMAH HEALTHTomah, Wisconsin 54660EFFECTIVE DATE: 10/1/18DIVISION: Patient Care ServicesP&G #: 500-Gen-017-0818ORIGINATION DATE: 11/91TITLE: Sedation/AnalgesiaPAGE: 1 of 6DATE:AuthorApproved By:DATE:Administrative Team LeaderDATE:Medical Staff President01 INVOLVESPatient Care ServicesMedical Staff02 PURPOSETo provide a guideline for the safe administration of sedation/analgesia.03 POLICYAll patients receiving sedation/analgesia will be monitored according to the following guidelines. Inorder to ensure quality care, the level of sedation/analgesia must be determined by a credentialedpractitioner. A registered nurse, trained in the use of sedation/analgesia, can administer minimal tomoderate sedation under direct supervision of any appropriately credentialed provider withsedation/analgesia privileges. The provider will acknowledge all intraprocedural orders with his/hersignature on the sedation/analgesia record. A CRNA must be responsible for administering deepsedation or administering anesthesia. The trained RN or CRNA must have no other significantresponsibility that would leave the patient unattended or compromise continuous monitoring. (Thispolicy does not apply to medications administered for pain control, seizures, sedation of mechanicallyventilated patients, or for urgent/ emergent endotracheal intubation.)All patients receiving procedural sedation must have a responsible adult, assuming care of patient,present at time of discharge.
P&G #: 500-Gen-017-0818TITLE: Sedation/AnalgesiaPAGE: 2 of 604 GUIDELINESA. The standards for sedation and anesthesia care apply when patients receive, in any setting, for anypurpose, by any route, moderate or deep sedation as well as general, spinal, or other major regionalanesthesia. Definitions of four levels of sedation and anesthesia include the following:1. Minimal sedation (anxiolysis) A drug-induced state during which patients respond normallyto verbal commands. Although cognitive function and coordination may be impaired,ventilatory and cardiovascular functions are unaffected.2. Moderate sedation/analgesia formerly called (“conscious sedation”) A drug induceddepression of consciousness during which patients respond purposefully to verbal commands,either alone or accompanied by light tactile stimulation. No interventions are required tomaintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function isusually maintained.3. Deep sedation/analgesia: A drug induced depression of consciousness during which patientscannot be easily aroused, but respond purposefully following repeated or painful stimulation.The ability to independently maintain ventilatory function may be impaired. Patients mayrequire assistance in maintaining a patent airway and spontaneous ventilation may beinadequate. Cardiovascular function is usually maintained.4. Anesthesia – Consists of general anesthesia and spinal or major regional anesthesia. It doesnot include local anesthesia. General anesthesia is a drug-induced loss of consciousnessduring, which patients are not arousable, even by painful stimulation. The ability toindependently maintain ventilatory function is often impaired. Patients often require assistancein maintaining a patient airway, and positive pressure ventilation may be required because ofdepressed spontaneous ventilation or drug-induced depression of neuromuscular function.Cardiovascular function may be impaired.Registered nurses may provide minimal to moderate sedation/analgesia. CRNAs may providemoderate sedation/analgesia and are the only providers to provide deep sedation/analgesia.B. EMERGENCY EQUIPMENT:The following must be immediately accessible and include at least the following:Crash CartOxygenDefibrillatorPharmacologic antagonists (Flumazenil and Naloxone)ECG monitorOximeterSuction deviceCapnography
P&G #: 500-Gen-017-0818TITLE: Sedation/AnalgesiaPAGE: 3 of 6C. PHYSICIAN/NURSING CARE RESPONSIBILITY:1. Pre-Procedure Assessmenta. Baseline history and physical information shall include, but not be limited to:1) Indications/symptoms for procedure.2) Current medications.3) Allergies and previous adverse drug reactions.4) Diseases, disorders and abnormalities including history of substance abuse.5) Assessment of mental status.6) Prior surgical procedures.7) Exam specific to procedure proposed.8) Pregnancy status.9) Vital signs/weight & height10) Airway assessment and pertinent patient/family history of prior anesthetics (AppendixA).11) Pulmonary, cardiac and neurologic exam and other as appropriate.12) ASA’s physical status category (Appendix B).13) NPO status14) A brief history and physical must be completed within 30 days prior to the procedure.An update must be completed the day of the procedure.b. Fasting history – If non-urgent procedure: Adult NPO solids 6 hours. NPO clear liquids2-3 hours. This should be closely adhered to due to possibility that minimal or moderatesedation may turn into deep analgesia/sedation. This offers better protection for patientswho may be at risk for aspiration (GERD, diabetics, hiatus hernia). Strong considerationshould be given to having a CRNA provide sedation and monitoring for the patientconsidered to have a full stomach. A colonoscopy patient may not have completed the prepif they are finishing the second half the morning of the procedure. These patients should befinished by 2-3 hours before the procedure.
P&G #: 500-Gen-017-0818TITLE: Sedation/AnalgesiaPAGE: 4 of 6c. Informed Consent - The patient or legal guardian shall be informed by the physician orCRNA about the risks, benefits, and alternatives to sedation as a component of the plannedprocedure. This must be documented by physician or CRNA.d. All patients scheduled for procedures receiving sedation/analgesia will have an armbandplaced after the use of two identifiers; i.e. stated name and date of birth. The procedure isconfirmed with patient.e. All pediatric patients up to age 18 receiving deep sedation/analgesia must haveanesthesia/CRNA present. For Pediatric patients up to age 18 receiving moderatesedation/analgesia the physician should consider anesthesia consult for CRNAinvolvement.2. Pre-Induction:Immediately prior to initiation of sedation, an assessment must be completed and documentedby a qualified provider to ensure patient remains an appropriate candidate forsedation/analgesia and procedure. Once again procedure and patient identity is confirmedduring “time out” just prior to starting procedure.3. During Procedurea. The minimum number of available personnel available shall be two: practitioner and RN orCRNA for monitoring. Patients receiving sedation/ analgesia are to be continuouslymonitored:1)2)3)4)5)Vital signs (BP, P, EKG)Oxygenation (Respiratory rate, skin assessment, 02 sat)Capnography on all patients other than minimal sedation as listed in guidelines 04-1.Medications (dose, route, response)Medication administration guidelines(The provider individualizes treatment for his/herown patient)a. Midazolam(0.5 to 2mg IV, titrated to max dose of 0.1mg/kg) 3-5 minutes prior toprocedure and repeated at 3-5 minute intervalsb. Fentanyl (12.5mcg to 50mcg IV, titrated to maximum dose of 3mcg/kg)at 3-5minute intervals6) Once suggested max dose for patient is reached, the provider will be notified and furtherorders documented.7) Reversal agents for Midazolam and Fentanyl shall be readily available and may beadministered according to the following guidelines:a. Romazicon (reversal agent for Midazolam)- 0.1mg IV every 1-2 minutesb. Naloxone (reversal agent for Fentanyl) – 0.2mgIV every 1-2 minutes
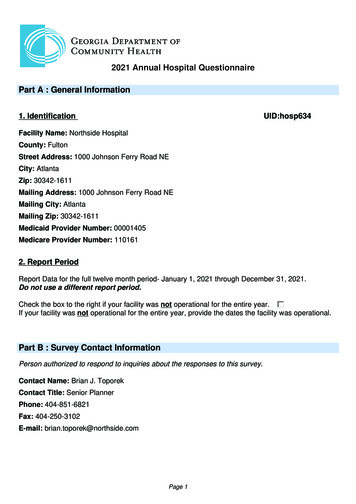
P&G #: 500-Gen-017-0818TITLE: Sedation/AnalgesiaPAGE: 5 of 68) LOC9) Emotional status10) Pain levelb. Exception: Any monitor that interferes with the accuracy or reliability of any diagnosticprocedure, e.g. MRI, can be removed at the discretion of the attending physician anddocumented.c. Supplemental oxygen is recommended for all patients other than minimal sedation.d. Documentation should be dictated by the patient’s physiologic response but should notexceed 5-minute intervals.e. Assessment should include the pre-procedure assessment and the immediate assessment asa baseline from which to compare the patient’s response to sedation.f. Additional documentation shall include:-Safety measures4. Following Procedurea. Patients who have received sedation/analgesia are to be monitored at regular intervals, notto exceed 15-minute intervals until return to baseline is attained. See page 2 of theSedation/Analgesia form section Post Anesthesia Score (Modified Aldrate score).Assessment items:1) Vital signs2) Level of consciousness3) Oxygenation (respiratory, skin assessment, O2 sat)4) Post-Anesthesia (Modified Aldrete) score of 8-10 or return to pre-sedation status(Appendix C). Aldrete score must be completed upon arrival to post procedure areaand before discharge to document a return to baseline.(a) In the ED RASS (The Richmond Agitation Sedation Scale) will be utilized forintubated patients receiving sedation.5) Patients having received reversal agents (Narcan, Romazicon) shall be monitored forone hour following administration of reversal agent (at 15 minute intervals).5. Dischargea. Patients will be assessed upon discharge. See page 2 of the Sedation/Analgesia formsection Post Anesthesia Score (Modified Aldrate score).b. According to the established discharge criteria, if the discharge criterion is not met within areasonable time frame, the practitioner must be notified.
P&G #: 500-Gen-017-0818TITLE: Sedation/AnalgesiaPAGE: 6 of 6c. The practitioner shall document the:- exam and patients response to exam- findings- discharge instructionsD. CREDENTIALING AND COMPETENCY1. The Medical Staff Credentials Committee will recommend to the Medical Staff ExecutiveCommittee approval of practitioners to prescribe, administer and select sedation/analgesiamedications, in addition to, monitoring patients receiving sedation/analgesia.2. The ability of RN’s to provide monitoring for patients undergoing sedation/analgesia will beassessed and maintained through the sedation/analgesia competency program. Minimumrequirements include BLS and ACLS certification.E. PERFORMANCE IMPROVEMENT1. Quality indicators are developed and utilized to monitor sedation/analgesia. These indicatorsmay include:- Patient outcomes- Appropriateness of use- Completeness of assessments.- Utilization Frequency05 FORMSSedation/Analgesia FormSedation/Analgesia Vital Sign Continuation FlowsheetAnesthesia Consent (reviewed with 500-Gen-014)06 REFERENCES1994 Pediatric Emergency Nursing ManualAirway Assessment & Anesthetic History (Appendix A)Selection Criteria (Appendix B)Discharge From Conscious Sedation (Sedation/Analgesia) Criteria (Appendix C)Recommended Drugs/Doses For Pediatric Sedation In Diagnostic, Therapeutic, OrInvasive ProceduresAdult IV Conscious Sedation (Sedation/Analgesia)Pediatric IV Conscious Sedation (Sedation/Analgesia)Pediatric Sedation Program- Standards of Care University of Wisconsin Hospital and ClinicsRichmond Agitation and Sedation Scale (RASS)
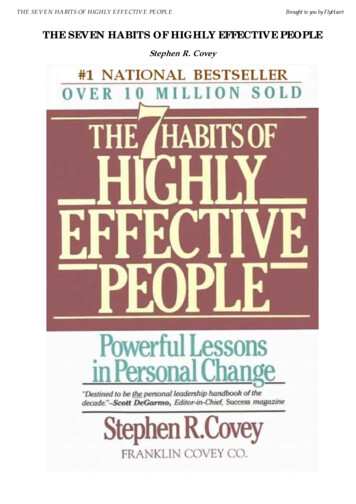
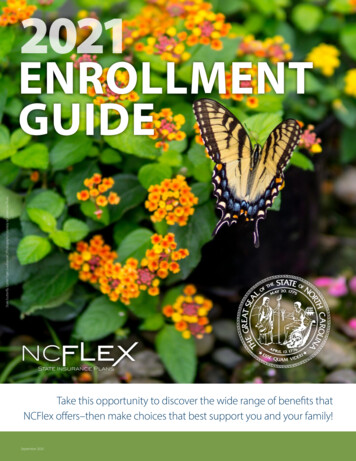
ALLERGIES/ Reaction:Latex Allergy: Yes NoSee Medication Reconciliation Sheet.Tobacco Use: Yes No ppdDesires smoking cessation: Yes NoPamphlet provided: Yes NoAlcohol Use: Yes No How much/oftenHistory of substance abuse: Yes NoAbuse Indicator: Negative PositiveAddress in Narrative.Medical History:No Yes (Explain)Heart DiseaseHTNPacemaker / DefibrillatorMitral valve prolapse/prosthetic valveLung diseaseSleep apneaDiabetes / endocrineNeurological disorderHematologic disorderRenal / Liver disorderProsthesis / ][]Pre-Procedure AssessmentLMP/EDC: Wt. kg. Ht. cm.(Pregnancy test if of child bearing age and no permanent sterilization)Glasses/Contact Lenses: On Off N/AHearing: R L N/AHOH Aid In / OutDentures: In OutN/A UpperLowerIdentification: Verbal ID Band (per 2 identifiers)Time of last solid intake Liquid intakeYesN/ANo*(*address in narrative)Driver with PatientPrep completedEmergency Equipment, Personnel &Medications AvailablePre-Anesthesia Score InitiatedUniversal Protocol Checklist initiated[][][][][][][][][][][][][][][]No Yes (Explain)Prior surgical procedures[ ] [ ]Problems with anesthesia or sedatio n[ ] [ ]History of pseudocholinesterase ormalignant hyperthermia in pt. or famil y [ ] [ ]Narrative:Nurse SignatureDate: Time:PRACTITIONER PORTIONPhysical See H&P []Dictation ocedure specific:Chief Complaint:Airway Assessment:Recessed ChinProtruding Upper TeethDecreased Neck range of motionMouth opening 2 fingerbreathsUvula Not VisibleHistory of sleep apnea/DisorderYes No[][][][][][][][][][][][]ASA Classification: (Circle One)I. A normal healthy patient.II. A patient with mild systemic disease.III. A patient with severe systemic disease that limits activity,but is not incapacitating **IV. A patient with an incapacitating systemic disease that is a constant threat to life.***V. A moribund patient not expected to survive 24 hours with or without operation. ***** Consider review by CRNA*** Administered by CRNAPractitioner SignatureTOMAH MEMORIAL ime
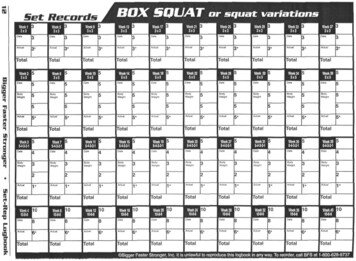
ColonColonEGDEGDScope Number: [ ] 230 2836 [ ] 220 02580[ ] 230 1147[ ] GL[ ] 251 6249PROCEDURE STARTat ileum PROCEDURE STOPPre-ProcAssessmentColon[ ] OximeterETCO2 Value(Reference Range: 35-45 mmHg)ECGSkin: Color, Temp, MoistureEmo/Mental A anxious, C calmMeds –Name Dose RouteWhole Blood Glucose(Patient Result)(Reference Range: 70-110 mg/dL)(Critical: 40mg/dL or 600 mg/dL)LOC:1 Alert; 2 Occ. Drowsy, easyto arouse; 3 Freq. drowsy, easy toarouse; 4 Asleep, easy to arouse; 5 Somnolent, difficult to arouseSafety Measures, ie. 1.Attended atall times; 2. Siderails up, call light inreach.Pain / DiscomfortInitialsIV fluids time site gauge attempt NurseIV dc’d at Cath intact good hemostasis total fluids no edema / erythema NurseCautery pad/location Skin condition before Skin condition afterVersed Total: mg Fentanyl Total: mcgOther Meds: N/ASpecimens obtained:RN Signature / Initials:TechRN Signature / Initials:POST ANESTHESIA SCORE(Modified Aldrete)Pre-ProcedureBaselinePostProcedurePrior ToDischargeDischarge CriteriaAble to move 4 extremities on command 2Able to move 2 extremities on command 1Able to move 0 extremities on command 0Able to deep breathe & cough freely 2Dyspnea or limited breathing 1Apneic 0Alert & OrientedMinimal or no bleedingPain ControlledAmb. w/o dizzinessTolerates oral intakeAble to void post procedureBP 20 of presedation level 2BP 20 – 50 of presedation level 1BP 50 of presedation level 0Fully awake 2Arousable to calling 1Not responding 0Oximetry 95% or baseline 2Oximetry 95% or 1-2% of baseline 1Oximetry 90% or 3% of baseline 0Able to pass flatusDischarge Instructions receivedYNN/AReleased to the care ofDischarge via W/C; Amb, Carried, OtherDate/Time of DischargeNurse SignatureTOTALProvider Signature verifying intra-procedure orders: Date: Time:TOMAH MEMORIAL HOSPITAL/TOMAH HEALTHSEDATION/ANALGESIA 08/2018
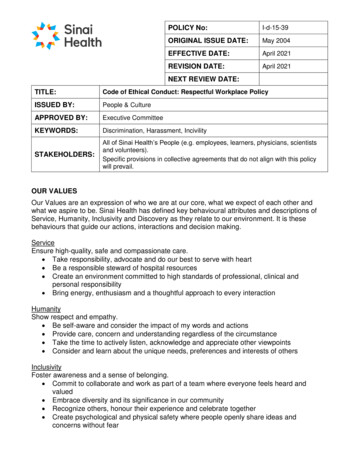
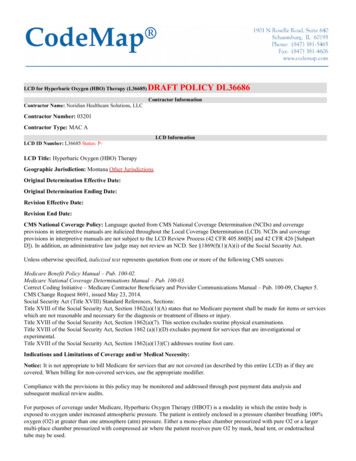
DateTimeBloodPressureMAPPulseResp.OximeterETCO2 Value(Reference Range: 35-45 mmHg)ECGSkin: Color, Temp, MoistureEmo/Mental A anxious, C calmMeds –Name Dose RouteWhole Blood Glucose(Patient Result)(Reference Range: 70-110 mg/dL)(Critical: 40 mg/dL or 600 mg/dL)LOC:1 Alert; 2 Occ. Drowsy, easyto arouse; 3 Freq. drowsy, easy to arouse;4 Asleep, easy to arouse; 5 Somnolent,difficult to arouseSafety Measures, ie. 1.Attended atall times; 2. Siderails up, call light inreach.Pain / ximeterETCO2 Value(Reference Range: 35-45 mmHg)ECGSkin: Color, Temp, MoistureEmo/Mental A anxious, C calmMeds –Name Dose RouteWhole Blood Glucose(Patient Result)(Reference Range: 70-110)LOC:1 Alert; 2 Occ. Drowsy, easyto arouse; 3 Freq. drowsy, easy to arouse;4 Asleep, easy to arouse; 5 Somnolent,difficult to arouseSafety Measures, ie. 1.Attended atall times; 2. Siderails up, call light inreach.Pain / DiscomfortInitialsTOMAH MEMORIAL HOSPITAL/TOMAH HEALTHSEDATION/ANALGESIA VITAL SIGNCONTINUATION FLOWSHEET08/2018
Appendix A500Gen017.frmConsiderations:AIRWAY ASSESSMENT & ANESTHETIC HISTORYPositive pressure ventilation, with or without endotracheal intubation, may be necessary ifrespiratory compromise develops during sedation/analgesia. This may be more difficult in patientswith atypical airway anatomy or conditions, which place them at risk for aspiration. Also, someairway abnormalities may increase the likelihood of airway obstruction during spontaneousventilation. Factors that may be associated with difficulty in airway management are:History-Previous problems with anesthesia or sedationStridor, snoring or sleep apneaDysmorphic facial features (e.g., Pierre-Robin syndrome, trisomy 21)Advanced rheumatoid arthritisUpper airway soft tissue edemaHistory of Gastric problems (see below*)Physical ExaminationHabitusSignificant obesity (especially involving the neck and facial structures)Head and NeckShort neck, limited neck extension, decreased hyoid-mental distance ( 6 cm in an adult),neck mass, cervical spine disease or trauma, tracheal deviationMouthSmall opening ( 3 cm in an adult); protruding incisors; loose or capped teeth; high archedpalate; macroglossia; tonsillar hypertrophy, non visible uvulaJawMicrognathia, retrognathia, trismus, significant malocclusionIf a patient presents with the above factors, an anesthesia consult should be considered.* Patients may also present with an increased risk of aspiration of gastric contents. Factors thatmay be associated with aspiration include, obesity, history of acid reflux, history of hiatal herniaand the patient with a full stomach or delay in gastric emptying (pregnancy, diabetes, trauma,recent narcotic ingestion, and mechanical obstruction).Careful attention must be given to prevent the patient from entering a deep level of sedation.Sodium citrate may be administered to neutralize stomach acid. Metoclopramide may beadministered to minimize risk of aspiration. If appropriate, a field block or regional anestheticmay be employed in order to minimize level of sedation required.
Appendix B500Gen017.frmSELECTION CRITERIA (APPENDIX B)Physical Status Classification of the American Society of AnesthesiologistsStatusIIIIIIIVVDefinitionA normal healthy patientA patient with mild systemic diseaseA patient with a severe systemic disease that limits activity, but isnot incapacitatingA patient with an incapacitating systemic disease that is a constantthreat to lifeA moribund patient not expected to survive 24 hours with or withoutoperationIf a patient has an ASA IV, consultation will occur with CRNA.Appropriate patients for RN administered sedation/analgesia are selected by usingthe Physical Status Classification of the American Society of Anesthesiologists.Patients classified as Status I or II are appropriate for RN administration.Consideration of an anesthesia consult should be given to patients who areclassified as a Status III. Patients classified as Status IV or V are not appropriatefor RN administered sedation/analgesia and should have an anesthesia providerresponsible for care. (Exception: At the discretion of the physician, patients whoare in a critical care setting (trauma patients in the ER) who already have requiredmonitoring in place may be administered sedation/analgesia by the RN.) TheAnesthetist may be consulted for patients difficult to classify. Patients under theage of 18 or pregnant must have clearance for sedation of any type by a providercredentialed to do so. Any patient with a history or family history relevant tomalignant hyperthermia or pseudocholinesterase deficiency, is not a candidate forRN monitoring; - any patient undergoing procedure where significant amounts offluid loss is anticipated, i.e., paraplegic having a major debridement is not acandidate for RN monitoring.
Appendix C500Gen017.frmDISCHARGE FROM CONSCIOUS SEDATION (SEDATION / ANALGESIA)CRITERIA (APPENDIX C)Minimum discharge/transfer criteria for a patient receiving sedation/analgesia is as follows:InpatientsTransfer to a patient care unit when the patient has met the following criteria: Aldrete (post-sedation) score above 8 or per physician order.SpO2 92% on room air or supplemental oxygen to maintain SpO2 90% or a returnto baseline.Transfer order written by a physician.OutpatientsAssessment data is collected and recorded to evaluate the patient status for discharge: Aldrete (post-sedation) score of 8-10 or score prior to sedation/analgesiaVital signs stable including temperaturePain and nausea controlledMinimal or no bleedingAble to void post procedureSpO2 92% on room air or supplemental oxygen to maintain SpO2 90% or a returnto baselineAble to swallowAble to tolerate oral intake oral fluids at a minimumAble to ambulate with assistance consistent with age and procedureBe accompanied by a responsible partyGiven both verbal and written discharge instructions. Include resource to contact if anyproblems arise.Patient and/or responsible adult verbalize understanding of discharge instructions.Able to pass flatus (lower GI endoscopy patient only)All of the above criteria must commensurate with pre-admission status.
ADULT IV (SEDATION / ANALGESIA)This table is meant to provide a quick reference to some commonly recommended sedatives which may be used in adults. These are meant onlyas suggestions. The clinician must individualize treatment for his/her own patient. ALL PATIENTS MUST BE MONITORED USINGGUIDELINES FOR SEDATION/ANALGESIA MONITORING (See reference below).DRUGCONCENTRATIONDiazepam(Valium)5 mg/mlMorphine4 mg/mlMeperidine 25-100 mg/ml(Demerol)ADMINISTRATIONTIME5-10 minutes prior toprocedureDOSINGRECOMMENTATIONS1-3 mg IV titrated to effect.Maximum dose 0.15 mg/kg.15-20 minutes prior toprocedureONSETDURATION3-5 minutes2-8 hours1-2 mg IV titrated to effect.Maximum dose 0.3 mg/kg.15 minutes3-4 hours5-10 minutes prior toprocedure10-20 mg IV titrated to effect.Maximum dose 3 mg/kg.10 minutes1-2 hoursMidazolam(Versed)1 mg/ml3-5 minutes prior toprocedure0.5 mg to 1 mg IV titrated tomaximum dose of 0.1 mg/kg.3-5 minutes2-6 hoursFentanyl50 mcg/ml3-5 minutes prior toprocedure25 mcg to 50 mcg IV titrated tomaximum dose to 3 mcg/kg.3-5 minutes1-2 hoursNaloxone(Narcan)0.4 mg/ml0.2 mg IV. May repeat 1 and 2-3minutes until effect achieved.Maximum dosing 1 mg.1-3 minutes20 minutesRomazicon0.1 mg/ml0.1 mg IV every 1-2 minutes. Mayrepeat every 2-3 minutes until effectachieved.1-3 minutes20-30 minutesKetamine50 mg/ml5-10 mg IV titrated to effect.Maximum dose 0.5 mg/kg.3-5 minutes30 minutes to1 hour.08/20183-5 minutes prior toprocedure
RECOMMENDED DRUGS / DOSES FOR PEDIATRIC SEDATION IN DIAGANOSTIC,THERAPEUTIC, OR INVASIVE PROCEDURESThis table is meant to provide a quick reference to some commonly recommended sedatives which may be used in children. These are meantonly as suggestions. The clinician must individualize treatment for his/her own patient. ALL PATIENTS MUST BE MONITORED USINGGUIDELINES FOR SEDATION/ANALGESIA MONITORING (See reference id500 mg/5 mlROUTE*Oral,RectalADMINISTRATIONTIME20 minutes prior am(Valium)Lorazepam(Ativan)Tab5 mgsyrup2 mg/mlTab (5 mg)Inj. 5 mg/mlTab (0.5 mg)Inj. (2 mg/ml)Oral1 hour prior to procedureOral20 minutes prior toprocedure1 hour prior to procedureOral, IM,SL1 hour prior to procedureMeperidine(Demerol)Inj. 25-100 mg/mlIM / SC15 minutes prior toprocedureMorphine4 mg/ml10 mg/mlIM/SC/PO15 minutes prior toprocedure08/2018IMINITIAL DOSE25-30 mg per kg.Max dose 500 mg (oral)75-100 (deep) rectalMax dose: Infant 1 gramChildren 2 grams5 mg ( 7 Y/O10 mg ( 7 Y/O)0.5 mg per kg.Max dose: 20 mg.2-10 mg.Max dose 10 mg.1-2 mgMax PO / IM dose 4 mgMax SL dose 2 mg50-100 mgIM/IV/SC Max dose 3mg/kg10-30 mg PO 1-5 mgIM/SCMax IM/SC/IV/PO 0.3mg/kg.2ND DOSE IFREQUIREDONSETDURATION37.5 mg/kg (repeatafter 20 minutes)30 minutes4-8 hoursSame dose (repeatafter 60 minutes)0.2 mg/kg60 minutes4-8 hours20-30minutes30 minutes2-6 hours30 minutes6-8 hoursMay repeat ½ doseafter 15 minutes5-10 minutes1-2 hoursMay repeat ½ doseafter 15 minutes20 minutes3-4 hoursMay repeat ½ doseafter 30 minutesMay repeat ½ doseafter 30 minutes4-8 hours
PEDIATRIC IV MODERATE SEDATION (SEDATION/ANALGESIA)This table is meant to provide a quick reference to some commonly recommended sedatives, which may be used in children. These are meantonly as suggestions. The clinician must individualize treatment for his/her own patient. ALL PATIENTS MUST BE MONITORED USINGGUIDELINES FOR MODERATE SEDATION/ANALGESIA MONITORING. (See reference below).DRUGCONCENTRATION ADMINISTRATIONDOSINGTIMERECOMMENTATIONS1 mg/ml3-5 minutes prior to0.5 mg to 1 mg IV titrated toprocedureeffect. Maximum dose 0.1mg/kg.3-5 minutes2-6 hoursFentanyl50 mcg/ml3-5 minutes priorprocedure12.5 mcg to 25 mcg IV titratedto effect. Maximum dose 3mcg/kg.3-5 minutes60-120 minutesKetamine50 mg/ml3-5 minutes prior toprocedure2.5 mg to 5 mg IV titrated toeffect. Maximum dose 0.15mg/kg.3-5 minutes15-60 minutesMorphine2-15 mg/ml15-20 minutes prior toprocedure0.5 mg – 2 mg IV titrated toeffect. Maximum dose 0.3mg/kg.15 minutes3-4 hours5-10 minutes prior toprocedure5 mg to 10 mg IV titrated toeffect. Maximum dose 3 mg/kg.10 minutes1-2 hoursMidazolam(Versed)Meperidine 25-100 mg/ml(Demerol)08/2018ONSETDURATION
Minimal sedation (anxiolysis) A drug-induced state during which patients respond normally to verbal commands. Although cognitive function and coordination may be impaired, ventilatory and cardiovascular functions are unaffected. 2. Moderate sedation/analgesia formerly called ("conscious sedation") A drug induced