Transcription
A Patient’s Guide toMedial Epicondylitis (Golfer’s Elbow)Iain is a specialist in musculoskeletal imaging and the diagnosis of musculoskeletal pain.This information is provided with the hope that you can better understand and manage yourcondition. The information is not specific to your condition and is meant as a general guideonly. Iain has added some information at the end of each booklet which might help addsome context in regard to assessment and management from a local perspective.info@driainduncan.com.auAll materials within these pages are the sole property of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is aregistered trademark of Medical Multimedia Group, LLC.DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain169
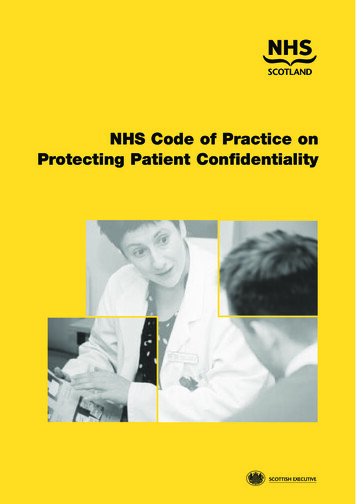
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)eOrthopod.comepicondyle. Wrist flexors are the muscles of theforearm that pull the hand forward. The wristflexors are on the palm side of the forearm.Most of the wrist flexors attach to one maintendon on the medial epicondyle. This tendonis called the common flexor tendon.IntroductionMedial epicondylitis is commonly known asgolfer's elbow. This does not mean that onlygolfers have this condition. But the golfswing is a common cause of medial epicondylitis. Many other repetitive activitiescan also lead to golfer's elbow: throwing,chopping wood with an ax, running a chainsaw, and using many types of hand tools.Any activities that stress the same forearmmuscles can cause symptoms of golfer'selbow.This guide will help you understand what parts of the elbow are affected what causes golfer's elbow how to make the pain go awayTendonsconnect muscleto bone.Tendons aremade up ofstrands of amaterial calledcollagen.The collagenstrands arelined up inbundles next to each other.CollagenBecause the collagen strands in tendons arelined up, tendons have high tensile strength.This means they can withstand high forces thatpull against both ends of the tendon. Whenmuscles work, they pull on one end of thetendon. The other end of the tendon pulls onthe bone, causing the bone to move.The wrist flexor muscles contract when youflex your wrist, twist your forearm down, orgrip with your hand. The contracting musclespull on the flexor tendon. The forces that pullon the tendon can build when you grip a golfclub during a golf swing or do other similaractions.CausesAnatomyWhy did I develop golfer's elbow?What parts ofthe elbow areaffected?Golfer's elbowcauses pain thatstarts on theinside bumpof the elbow,the medialMedial epicondyleOveruse of the muscles and tendons of theforearm and elbow are the most commonreason people develop golfer's elbow.Repeating some types of activities over andover again can put too much strain on theelbow tendons. These activities are not necessarily high-level sports competition. Shoveling,gardening, and hammering nails can all causethe pain of golfer's elbow. Swimmers whoDISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1692
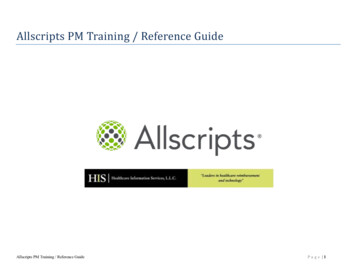
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)try to pick up speed by powering their armthrough the water can also strain the flexortendon at the elbow.In some cases, the symptoms of golfer'selbow are due to inflammation. In an acuteinjury, the body undergoes an inflammatoryresponse. Special inflammatory cells maketheir way to the injured tissues to help themheal. Conditions that involve inflammation areindicated by -itis on the end of the word. Forexample, inflammation in a tendon is calledtendonitis. Inflammation around the medialepicondyle is called medial epicondylitis.However,golfer's elbowoften is notcaused byinflammation.Rather, it is aproblem withinthe cells ofthe tendon.Doctors callthis condition tendinosis. In tendinosis, wear and tearis thought to lead to tissue degeneration. Adegenerated tendon usually has an abnormalarrangement of collagen fibers.Instead of inflammatory cells, the bodyproduces a type of cells called fibroblasts.When this happens, the collagen loses itsstrength. It becomes fragile and can breakor be easily injured. Each time the collagenbreaks down,the bodyrespondsby formingscar tissue inthe tendon.Eventually,the tendonbecomes thickened fromextra scartissue.eOrthopod.comNo one really knows exactly what causestendinosis. Some doctors think that the forearmtendon develops small tears with too muchactivity. The tears try to heal, but constantstrain and overuse keep re-injuring the tendon.After a while, the tendons stop trying to heal.The scar tissue never has a chance to fullyheal, leaving the injured areas weakened andpainful.SymptomsWhat does golfer's elbow feel like?The main symptom of golfer's elbow is tenderness and pain at the medial epicondyle ofthe elbow. Pain usually starts at the medialepicondyle and may spread down the forearm.Bending your wrist, twisting your forearmdown, or grasping objects can make the painworse. You may feel less strength whengrasping items or squeezing your hand into afist.DiagnosisHow can my doctor be sure I have golfer'selbow?Your doctor will first take a detailed medicalhistory. You will need to answer questionsabout your pain, how your pain affects you,your regular activities, and past injuries to yourelbow.The physical exam is often most helpful indiagnosing golfer's elbow. Your doctor mayDISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1693
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)position your wrist and arm so you feel astretch on the forearm muscles and tendons.This is usually painful with golfer's elbow.Other tests for wrist and forearm strength areused to help your doctor diagnose golfer'selbow.You may need to get X-rays of your elbow.The X-rays mostly help your doctor rule outother problems with the elbow joint. The Xray may show if there are calcium deposits onthe medial epicondyle at the connection to theflexor tendon.Golfer's elbow symptoms are very similar to acondition called cubital tunnel syndrome. Thiscondition is caused by a pinched ulnar nerveas it crosses the elbow on its way to the hand.If your pain does not respond to treatments forgolfer's elbow, your doctor may suggest teststo rule out problems with the ulnar nerve.When the diagnosis is not clear, the doctormay order other special tests, such as amagnetic resonance imaging (MRI) scan orultrasound. An MRI scan uses magnetic wavesto create pictures of the elbow in slices. TheMRI scan shows tendons as well as bones.Ultrasound tests use high-frequency soundwaves to generate an image of the tissuesbelow the skin. As the small ultrasound deviceis rubbed over the sore area, an image appearson a screen. This type of test can sometimesshow collagen degeneration.TreatmentHow can I make my pain go away?Nonsurgical TreatmentThe key to nonsurgical treatment is to keep thecollagen from breaking down further. The goalis to help the tendon heal.If the problem is caused by inflammation, antiinflammatory medications such as ibuprofenmay give you some relief. If inflammationdoesn't go away, your doctor may inject theelbow with cortisone. Cortisone is a powerfuleOrthopod.comanti-inflammatory medication. Its benefits aretemporary, but they can last for a period ofweeks to several months.Shock wave therapy is a newer form of nonsurgical treatment. It uses a machine to generateshock wave pulses to the sore area. Patientsgenerally receive the treatment once each weekfor up to three weeks. It is not known exactlywhy it works for golfer's elbow, but recentstudies indicate that this form of treatmentcan help ease pain, while improving range ofmotion and function.Doctors commonly have their patients withgolfer's elbow work with a physical or occupational therapist. At first, your therapist willgive you tips on how to rest your elbow andhow to do your activities without putting extrastrain on your elbow. Your therapist may applytape to take some of the load off the elbowmuscles and tendons. You may use an elbowstrap that wraps around the upper forearm ina way that relieves the pressure on the tendonattachment.Your therapist may apply ice and electricalstimulation to ease pain and improve healingof the collagen. Therapy sessions may alsoinclude iontophoresis, which uses a mildelectrical current to push anti-inflammatorymedicine to the sore area. This treatmentis especially helpful for patients who can'ttolerate injections. Exercises are used togradually stretch and strengthen the forearmmuscles.Because tendinosis is often linked to overuse,your therapist will work with you to reducerepeated strains during activity. Whensymptoms are from a particular sport or workactivity, your therapist will observe your styleand motion with the activity. Your therapistmay suggest ways to protect the elbow duringyour activities. Your therapist can also checkyour sports equipment and work tools andrecommend ways to alter them to keep yourelbow safe.DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1694
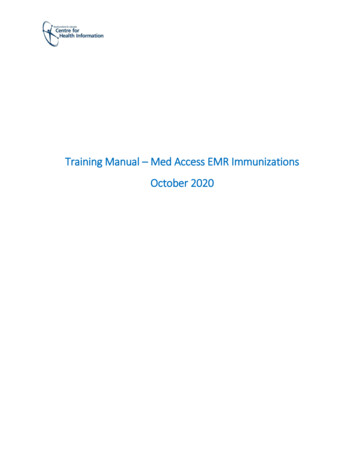
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)SurgerySometimes nonsurgical treatment fails to stopthe pain or help patients regain use of theelbow. In these cases, surgery may be necessary.Tendon DebridementWhen problems are caused by tendinosis,surgeons may choose to take out (debride)only the affected tissues within the tendon. Inthese cases, the surgeon cleans up the tendon,removing only the damaged tissue.Tendon ReleaseA commonlyused surgeryfor golfer'selbow is calleda medialepicondylerelease. Thissurgery takestension offthe flexortendon. Thesurgeon beginsby making an incision along the arm overthe medial epicondyle. Soft tissues are gentlymoved aside so the surgeon can see the pointwhere the flexor tendon attaches to the medialepicondyle.The flexortendon is thencut where itconnects to themedial epicondyle. Thesurgeon splitsthe tendonand takes outany extra scartissue. Anybone spurs found on the medial epicondyleare removed. (Bone spurs are pointed bumpsthat can grow on the surface of the bones.)eOrthopod.comSome surgeonssuture the looseend of thetendon to thenearby fasciatissue. (Fasciatissue coversthe musclesand organsthroughoutyour body.)Your surgeonwill look at theulnar nerve, tomake sure thatit is not beingpinched. If thenerve looksfine, the skinis then stitchedtogether.This surgery canusually be done on an outpatient basis, whichmeans that you don't have to stay overnightin the hospital. It can be done using a generalanesthetic or a regional anesthetic. A generalanesthetic puts you to sleep. A regional anesthetic blocks only certain nerves for severalhours. For surgery on the elbow, you wouldmost likely get an axillary block to numb yourarm.RehabilitationHow soon can I use my elbow again?Nonsurgical RehabilitationIn cases where the tendon is inflamed, nonsurgical treatment is usually only needed for fourto six weeks. When symptoms are from tendinosis, you can expect healing to take longer,usually up to three months. If the tendinosis ischronic and severe, complete healing can takeup to six months.DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1695
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)After SurgeryRecovery from surgery takes longer.Immediately after surgery, your elbow isplaced in a removable splint that keeps yourelbow bent at a 90-degree angle. Ice andelectrical stimulation treatments may be usedduring your first few therapy sessions to helpcontrol pain and swelling from the surgery.Your therapist may also use massage and othertypes of hands-on treatments to ease musclespasm and pain.You will gradually work into more activestretching and strengthening exercises. Youjust need to be careful to avoid doing toomuch, too quickly. Active therapy starts abouttwo weeks after surgery. Your therapist maybegin with light isometric strengthening exercises. These exercises work the muscles of theforearm without straining the healing tissues.You will use your own muscle power in activerange-of-motion exercises.eOrthopod.comAt about six weeks, you start doing moreactive strengthening. As you progress, yourtherapist will give you exercises to helpstrengthen and stabilize the muscles and jointsof the wrist, elbow, and shoulder. You'll alsodo exercises to improve fine motor control anddexterity of the hand. Some of the exercisesyou'll do are designed to work your hand andelbow in ways that are similar to your worktasks and sport activities. Your therapist willhelp you find ways to do your tasks that don'tput too much stress on your elbow.You may need therapy for two to threemonths. It may take four to six months to getback to high-level sports and work activities.Before your therapy sessions end, your therapist will teach you a number of ways to avoidfuture problems.DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1696
A Patient's Guide to Medial Epicondylitis (Golfer’s Elbow)eOrthopod.comNotesDISCLAIMER: The information in this booklet is compiled from a variety of sources. It may not be complete or timely. It does not cover all diseases, physical conditions, ailments or treatments. The information should NOTbe used in place of a visit with your health care provider, nor should you disregard the advice of your health care provider because of any information you read in this booklet. All materials within these pages are the soleproperty of Medical Multimedia Group, LLC and are used herein by permission. eOrthopod is a registered trademark of Medical Multimedia Group, LLC.iain1697
eOrthopod.comMore about the role of ultrasound and injections forthis conditionAbout ultrasound1. Ultrasound can resolve finer details than MRI and has a more flexible field-of-view2. The ultrasound probe can be placed exactly where it hurts and focus on sorting outyour symptoms3. Doppler ultrasound gives important information about the blood flow4. Ultrasound is best for guiding therapeutic interventionsPerhaps one of the biggest advantages of MSK ultrasound is its use to help guidetargeted injections. Ultrasound guided injections of corticosteroid into the tendon arehelpful in reducing the symptoms but repeated injections are not recommended as theycan weaken an already damaged tendon. Injection of other materials is sometimesundertaken and can provide excellent symptomatic relief.About InjectionsCorticosteroid (cortisone) injections are sometimes part of managing the pain for thiscondition but do not change the long term outcome which is generally good. When thecondition persists or the healing response is delayed, slowed, or abnormal then asubstance known as POLIDOCANOL is sometimes recommended. This directly altersthe healing response by causing sclerosis of abnormal small vessels and nerves.Whether this is appropriate depends on a host of factors including most importantly theultrasound appearance in relation to the duration of symptoms. Dr Duncan or yourphysician can advise you whether this might be appropriate.Occasionally when the healing response is deficient early (lack of blood flow) in theclinical course AUTOLOGOUS BLOOD injections are suggested to promote thehealing response. This involves taking a small amount of your own blood and injectingit into the abnormal zone of the tendon. There are multiple chemical and healingpromoters within your own blood.For more about Injections for this condition see also 69
Medial epicondylitis is commonly known as golfer's elbow . This does not mean that only golfers have this condition. But the golf swing is a common cause of medial epicon - dylitis. Many other repetitive activities can also lead to golfer's elbow: throwing, chopping wood with an ax, running a chain saw, and using many types of hand tools.