Transcription
DCCUMENT PESUME03758 - [B2934205]Cost of Spinal Cord Injuries in the United States and Progressin Spinal Cord Regeneration. HRD-78-10; B-164031(2). October 14,1977. 42 pp.Staff study.Issue Area: Health Programs (1200).Contact: Susan Resources Div.Budget Function: Health: health Research anri Education (552).Organi7aticn Concerned: Department of Health, Education, andWelfare; Veterans Administraticm.A study was conducted of spinal cord injury costs inthe United States and current research efforts involving spinalcord regeneration. The consequences of a spinal cord injuryrange from partial paralysis to death. A victim who survivesincurs lifetime medical costs that can range between 44,000 to 115,000 depending on the extent of the injury, not to mentionthe lost earnings and other injury related costs. Advances havebeen made in diagnosing spinal cord injuries and treating damageto the cord caused by pressure on the spine. However, once thecord's nerve fibers aree jtroyed, function below the level ofthe injury is usually lost and no treatment available canregenerate nerve fibers. Regenerati:n research to date has notbeen successful in regrowing nerve fibers in humans for numerousreasons. many Federal agencies are bsudying the pLoblem with nocentral direction and are supporting various approaches to solvethe problem. In England special centers have been developed totreat spinal cord injuries and the concept has been acceptedthroughout Europe. (Author)
STUDY BY THE STAFF OFTHEU.S. GENERAL ACCOUNTING OFFICECost Of Spinal Cord InjuriesIn The United States AndProgress In Spinal Cord RegenerationThe consequences of a spinal cord injury can bedevastating- from partial paralysis to death. A victimwho survves Incurs lifetlnm medical costs that canrange between 44,000 to 115,000 depending onthe extent of the injury, not to menticn the lostearnings and other injury related costs.Advances have been made in diagnosing spinal cordinjuries and treating damage to the cord caused bypressure on the spine. However o--; the cord's nervefibers are destroyed, function below the :evel of theinjury is usually lost and no treatment available canregenerate nere fibers.In England, special centers were developed to treatspinal cord injuries and the concept has beenaccepted throughout Europe. This concept consists ofestablishing acute spinal cord injury centersthroughout the country staffed with amulti-disciplined team of medical specialists. Thisapproach should be more widely used in the UnitedStates, according to medical authorities, whileresearch on regenerating the spinal cord continues.Regeneration research to date has not been successfulin regrowing nerve fibers in humans for numerousreasons Many Federal .aencies are studying theproblem with no central direction and are supportingvarious approachds to solve the problem.mD-3o1OOCTOBER 14, 1977
Con tentsPageCHAPTER1INTRODUCTIONNature of spinal cord injuryConsequences of spinal cord injury1242EXTENT AND CAUSES OF SPINAL CORD INJURYIncidence and prevalenceCauses8883METHODS OF TRPATING SPINAL CORD INJURYDiagnostic advancesTreatment of injury related problemsTreatment of spinal cord injuryAcute spinal cord injury centers10101012134COSTS OF SPINAL CORD INJURIESCost componentsDirect costs1718195PROGRESS AND PROBLEMS IN SPINAL CORDINJURY AND REGENERATION RESEARCHProjects funded on spinal cord injuryand regeneration researchSpinal cord injury researchRegeneration research .in theUnited StatesRegeneration research in theSoviet UnionProspects for a breakthrough inspinal cord regenerationComputer by-pass approach6TRAINING AND COORDINATIONTrainingCoordination efforts26262931353838414141
ral Accounting OfficeInsurance Institute for Highway SafetyNational Institutes of HealthNational Institute for Neurological andCommunicative Disorders and StrokeNational Paraplegia FoundationNew York UniversityParalyzed Veterans of AmericaRehabilitation Services AdministrationSpinal Cord InjuryVeterans Administration
CHAPTER 1INTRODUCTIONIn a letter dated October 8, 1976, five members of theCongress from Oregon requested that GAO conduct a study ofspinal cord injury (SCI) costs in the United States andcurrent research efforts involving spinal cord regeneration.We agreed that we would examine other aspects of traumaticspinal cord injuries including annual incidence, prevalence,and causes of such injuries; progress and problems intreatment; the status of efforts to regenerate the humanspinal cord after injury; vnd coordination efforts amongthe various Federal organizations involved in researchin this area.This staff study included reviewing studies, reportedon in the literature, and interviewing officials of thefollowing organizations:Federal Agencies and Depa-tmentsDepartment of the ArmyDepartment of the NavyNational Aeronautics and Space AdministrationNational Institutes of HealthNational Science Foui.dationRehabilitation Services AdministrationVeterans AdministrationPrivate Organizations, Medical Schools, and HospitalsInsurance Institute for Highway SafetyInstitute for Rehabilitation MedicineNational Paraplegia FoundationParalyzed Veterans of AmericaBellevue Hospital Acute Spinal Cord Injury CenterCase-Western Reserve UniversityCornell University Medical SchoolJohns Hopkins University Medical SchoolMedical University of South CarolinaNew York University Medical CenterOhio State University Acute Spinal Cord Injury CenterRancho Los Amigos HospitalUniversity of Maryland Medical SchoolUniversity of MichiganUniversity ot Texas Medical SchoclUniversity of Wisconsin Medical School
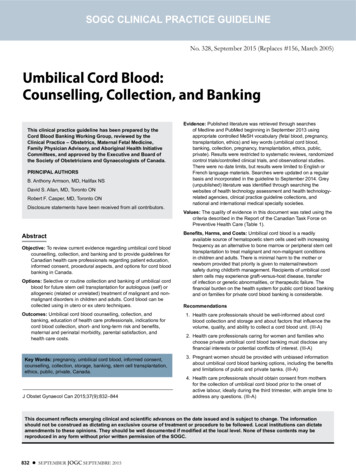
We also visited acute SCI centers at Bellevue Hospital,New York, New York and the Veterans Administration Hospital,West Ruxbury, Massachusetts. Finally, to identify currentspinal cord injury and regeneration research projects, weused data provided by the various Federal agencies and private organizations.NATURE OF SPINAL CORD INJURYThe spinal cord and the brain make up the central nervous system. The spinal cord is composed of approximately100 million nerve fibers and cells and is about 17 incheslong. It connects the brain with the muscles, skin, andinternal organs.All important motor and sensory functions controlled bynerve messages or impulses that originate in the brain travel along the nerve fibers in the spinal cord.As shown in figure 1, the spinal cord is divided into31 segments (8 cervical or neck, 12 thoracic or chest and 11lumbar or lower back) with nerve roots emerging from eachsegment. These nerve roots carry messages to and from themuscles or other parts of the body. Nerves which connectthe central nervous system to other parts of the bodymake up the peripheral nervous system. Figure 1 also showsthe consequences of suffering an SCI by level of injuryor the cord.Internally, the spinal cord is composed of an Duterwhite matter consisting of nerve fibers carrying impulses toor from the brain and peripheral nerves, and an inner graymatter made up of nerve cells. The gray matter has thegreatest metabolic activity and is the most sensitive toinjury.The gray matter is composed of nerve cells calledneurons. Each neuron consists of a cell body and one or morethreadlike projections that may reach a length of severalfeet. Those projections that receive messages and carry themtowards the cell body are called dendrites and those thatcarry them away from the cells are called axons (nervefibers).Nerve fibers which have a common origin and common destination are called nerve tracts.Nerve fibers terminate by branching into many fine filaments called terminals. These terminals establish contactwith other cell bodies or organs at a junction called a synapse. The function of the synapse is to transfer chemical2
Figure 1Corvical(C)c:5 quadriplegiaPeduced respiratory capacity. Patienttotally depencden: i.nothers. Wheel.I--.----.----.-Thoracicchair indispensable.(Th)C7 quadriplegiaReduced respiratory capacity. Patientalmost totally dependent on others. Wheelchair Indispendable Need for splints andother aids for the forearms and hands.C8-Th 1 parapiegiaReduced respiratory capacity. Partialdependence on others but only minimalaid needed for personal care.Wheel.chair indispensabie Crutchgait possible with long leg braces.pelvic bend with hip locks and withor without a spinal brace, and twocrutches Possible to drive a carfitted with hand controls andautomatic clutch.Th 1-2 paraplegaReduced respiratory capacity Complete independence. Whee! chair indispensable. Crutch gait possiblewith long leg braces but not necessarilV a pelvic band, and crutchesPossible to drive a car finedwith hand controls but not necessardly with an automat c clutch------Lumber(L)Th 7 parapleg aComplete IndependenceWheel-charindispensable Crutch gat possblelwith long leg braces but not neces'arilv a pelvic band, and crutchesPossible to drive a car finedwith hand controls.Th 12 L1egiComplete independence Wheel-chairindispensable. Crutch gait possiblewith leg braces and crutches Possible to drive a car with handcontrols.Complete independence at home andelsewhere. Wheel-chair not Indispensable. Normal walking possiblewith foot braces to counter dropfoot, crutches and sometimes kneestabilizers. Possible to drivea car fitted with hand controlsII'C&uds lQuina-------
or electrical activity from the neuron to its target in order to transfer the nerve impulse.The human spinal cord like the brain is unable to replace destroyed nerve cells. When a spinal nerve fiber isdamaged it is unable to cross the area of injury and reestablish communication beyond the point of injury. Thisis in contrast to tne peripheral nervous system where severed nerves can grow back and reestablish functional communication. The spinal cord, unlike s-me portions of the brain,has no spare parts or alternate pathways so that undamagedportions generally cannot take over or be trained to takeover the function of the damaged portion.CONSEQUENCES 0SPINAL CORD INJURYThe consequences of spinal cord injury range frompartial paralysis to death. An SCI causes an interruption ofthe nerve messages that are transmitted from the brain downto the skin and muscles and vice versa. Thus, the portionsof the body below the level of the injury are left unfeeling, and nonfunctional. Generally, the higher the injury onthe spinal cord, the greater the disability.There are two main categories of SCI, complete and incomplete. Complete lesions are defined as those in which thereis a total paralysis of all muscles and a total loss of allsensations below the level of injury. Incomplete lesions aredefined as those in which there is preservation of some voluntary movements or sensations below the level of injury.According to NIH and VA officials, injuries to the spinalcord rarely result in complete lesions, and persons sustaining complete lesions rarely show improvement. Generally,persons sustaining incomplete lesions have a better chancefor functional recovery.SCI victims are classified as either paraplegics orquadriplegics. Victims whose lower extremities and abdominalfunctions are affected are called paraplegics. Their injuryis at the thoracic level or below. Victims whose injury isin the cervical region have paralysis of both the upper andlower extremities with effects on body organs such as thelungs. "'he;are called quadriplegics. However, often theterm wparaplegic' is used as a general description of a person suffering an SCI, regardless of the level of injury.The main determinant in recovery of function after anSCI is the level of the injury to the spinal cord. Injuries4
in the cervical region usually result in quadriplegiawith paralysis of both arms and legs and with involvementof bladder and bowel functions. The higher levels, 'thoseabove the fourth cervical level, are usually fatal.Persons with injuries at the sixth and seventh cervicallevel have nearly normal shoulder and elbow function, butdiminished hand function. These persons are often able toperform many elements of self care, but are significantlydependent on others. Patients with injuries at the eighthcervical and first thoracic levels have most of their handfunctions, but despite paralyzed lower limbs, bowels andbladder can achieve nearly complete independence. Personswith injuries at the second thoracic level and below areparapalegic with normal upper extremity function but paralyzed legs. Their bladder, bowel and sexual functions arealso affected. These individuals are capable of completeindependence but are confined to a wheelchair. Not untilthe level of injury is in the mid-lumbar segments isreasonable ambulatory function possible with the help ofcrutches and foot braces.The medical complications and functional disabilities ofSCI are more serious than might be apparent. Paralysis ofthe legs does more than prevent walking. It can cause severeand painful muscle contractions, spasticity, and orthopedicdeformities. The sensation of pain is lost in the affectedarea, thus removing a body safety mechanism. Pain signalsdanger from heat, cold, and pressure. These signals reachhealthy persons even while they are sleeping, causing physical reactions. Thus, we change our sleeping position without waking because of the discomfort of skin and body tissueswhich have been under pressure. We shift our position whenawake, too, often without realizing it. Lacking sensation inlarge areas of his body, both asleep and awake, the paraplegic develops decubitus ulcers (pressure sores) on hisbuttocks, heels, and other bony parts of his body. Aparaplegic's ability to perspire is also impaired. Sinceperspriation helps to cool the body under conditions ofsevere heat, the SCI victim is vulnerable to hot weather andto fever caused by mild infections due to his reduced abilityto perspire.Paraplegics may also lose voluntary control of theirbowel and bladder functions. Genital sensation may be lostand sexual function impaired. Urinary infections, bladderstones. end gastrointestinal disorders are frequent complications. Bladder catheterization is usually needed, eithercontinuously or on an intermittent basis and catheterizationitself can be a cause of infection. Respiratory disorders5
are also a serious complication and problem for quadriplegics.Along with the physical disabilities and complications,an SCI victim and his family must cope with emotional problems. The victim may suddenly be dependent on others, often at a tome of life when he is at a peak of physical andsocial independence. Career, financial independence,marriage, family, and social relationships are all changed.Although rehabilitation and a somewhat satisfactory lifestyle are now possible, the patient's own psychologicaladjustment to his disability is zriti:al to his recovery.According to NIH and VA officials, most spinal cordinjuries are thoue of contusion (bruising), crushing ordestruction due to loss of blood flow. If the sprinal cordis compared to a telephone cable containing thousands ofwires, damage to the cord is similar to twisting andDissolving of the individual wires with a resultarnt gapin the cable and a barrier composed of non-conductingmaterial introduced at the location of the damage. In aminority of cases, the cord is transected (cut) at the timeof injury and all function is immediately lost.NIH and VA officials told us that while paralysis isimmediate after a traumatic SCI, the pathological processesthat result in destruction and death of nerve tissue evolveover a tour to six hour period. SCI research showed thatduring this period circt ition is impaired and hemorrhagebegins in the central gray matter of the cord. Oxygenlevels in the nerve tissues drop and the hemorrhagecontinues to spread causing cell death. Following this,edema (swelling) forms in the spinal white matter andcauses degeneration of the spinal nerve fibers. Thisdegeneration produces an actual gap in the spinal cordnerves. Scar tissue forms at the point of the damageand motor and sensory functions are lost. The processthen spreads up and down the spinal cord sometimesinvolving destruction of brain cells. These officialstold us that in order to prevent permanent injury to thespinal cord, this process must be stopped very earlyin its progression.Present day SCI research is mainly directed in twoareas. The first area of research is called spinal cordinjury research and its goal is to limit the degenerationin the spinal cord by preventing the sequence of eventsthat occurs after an injury. The second field of researchis directed towards stimulating or encouraging the orderly
regrowth of spinal nerve fibers. Such research is calledregeneration research. To date, no one has been akle toregenerate nerves in the human spinal cord. Proqress andproblems in spinal cord injury and regeneration researchwill be discussed in Chapter 5.
CHAPTER 2EXTENT AND CAUSES OFfMAL- RDC INJURIESINCIDENCE AND PREVALENCENumerous studies have been performed on the extentof spinal cord injuries in the United States with vastdifferences in their results.In a study released in 1975, NIH estimated thatthere were 100,000 victims of traumatic spinal cord injuryand nearly 10,000 new cases each year.In 1974, the National Paraplegia Foundation (NPF),an organization providing primarily information andreferral services for paraplegic on matters such asrehabilitation, care, and research, also studied spinalcord injury. NPF estimated that in 1970 there were 46,700victims of traumatic spinal cord injury alive in the UnitedStates and that this figure will increase to 75,2000 by1980. NPF estimated that 3,190 new cases occurred in 1974.Also, in 1974, the Rehabilitation Services Administration (RSA) estimated that the total number of SCIvictims to be between 100,000 and 125,000. RSA saidthat 7,000 to 10,000 new cases occur each year.Studies have shown that young people suffer mostfrom SCI. In 1976, NPF stated that 90 percent of thevictims are between the ages of 16 and 30, and a 1974study by RSA yielded similar results.CAUSESWe identified seven studies that assessed the causesof SCI. While four of the studies were conducted outsideof the United States and were conducted during differenttime periods (1968-1976) all the studies showed motorvehicle accidents to be the leading causes of SCI. Forexample, using the results of a 1974 California study,NIH said that motor vehicle accidents account for 56percent of all acute SCI cases. The table belowsummarizes the results of the three American studies.
Causes of SCI (in percent)Motor Vehicle FallsSports Assault OtherNIH (1974)56197126Rancho Los Amigos SCICenter, Calif. (1969)4812lla/1910Florida Study (1976)381621187a/Diving only
CHAPTER 3METHODS OFTREATING SPINAL CORD INJURYAt the time of World War I only 10 percent of paraplegics lived for a year after injury according to NIH. Today,90 percent survive and after one year following the injurytheir mortality rate only slightly exceeds that of the general population. These results are attributable to a numberof factors which are discussed below.DIAGNOSTIC ADVANCESOnce an SCI victim's condition is stabilized, a thoroughneurological examination with specific attention to demonstrating the presence or absence of function in the spinalcord below the injury is the main part of diagnosis, according to medical officials we interviewed. A new developmentin testing the ability of the spinal cord to function isthrough "evoked sensory corti, al potentials." This techniqueinvolves placing recording electrodes on the patient's scalpand stimulating peripheral nerves below the injury. The electrodes pick up any responses and a recorder prints out theresults. The primary value of this technique is in distinguishing complete from incomplete injuries.Another diagnostic advance has come in the developmentof myelography which is a special technique to photograph thespinal cord. Myelography involves injecting a substance intothe area around the spinal cord (called th- aQinal canal) toenhance X-rays taken of the cord and its soft tissue.TREATMENT OF INJURY RELATED PROBLEMSSeveral clinical advances have been made in treatingacute SCI related problems. Injury below the waist oftenresults in loss of bladder and bowel function. Thus, bladderand bowel infections are a problem and urinary tract complications are a major cause of death for paraplegics.Thedevelopment of antibiotics, the specialty of urology andeducating the patient in proper bladder and bowel maintenancehave greatly aided in solving these problems.A major advance in preventing urinary infections is thedevelopment of the technique of intermittent catheterizationto pass urine.A catheter, which is a tubular instrument10
used for withdrawing body fluids, is inserted into thebladder through the urethra every six to eight hours.Urine is then withdrawn through the catheter, emptying thebladder. Before the development of this technique, acatheter had to be inserted permanently in the victim.According to the medical officials we interviewed, thecatheter itself was often a cause of infection. Medicalstudies by hospitals using intermittent catheteriztion haveshown that 75 to 85 percent of patients were free fromurinary infections upon discharge.Advances in treating bowel problems have consistedmainly of establishing a regular elimination pattern for thepatient through a combination of proper diet, massage andrectal stimulation.Decubitus ulcers (pressure sores) are a serious problemfor paraplegics. When a paraplegic remains in the sameposition for an extended period, the constant pressure ofthe body's weight will cause the skin to break down andsores to develop. Because of paralysis, the SCI victim canneither perform the shiftings and turnings that are naturalto healthy people, nor feel that a sore is developing.Today, this problem can be virtually eliminated, accordingto medical authorities.Prevention of pressure sores is based on maintaininggood general skin condition and avoidance of prolonged skinpressure. To accomplish the latter, special'y designed bedshave been developed so that the patient can be turned torelieve pressure while confined to bed and special wheelchairs have been developed to prevent pressure on thepatient's skin. In addition, the victim is educated on thenecessity of avoiding prolonged skin pressure and the importance of daily inspections of the parts of the body mostsusceptible to pressure sores.When a person suffers an acute SCI, the muscles belowthe injury often are still function but cannot be conttrolled. This condition is called spasticity. Severe spasticity is treated by either muscle relaxants or surgery.According to a neurosurgeon at the University of MarylandMedical School, surgery to reduce spasticity has an initialsuccess rate of 90 percent, but only about 50 percent ofpatients having such surgery retain any long term benefit.One of the biggest problems for quadriplegics is musclecalcification (hardening of tissue resulting from calciumdeposits), according to a physician at the Institute for
Rehabilitation Medicine in New York. When musclecalcification occurs, motion becomes impossible. These problemshave been lessened through improved rehabilitation techniques and returning the patient to activity in a shortperiod of time.All quadriplegics suffer impairmentrespiratoryfunction to some degree because the chest ofand abdominalmuscles are paralyzed. Injuries above the fourthcervicallevel result in total paralysis of the diaphram andlifeis not possible without artificial respiratory supportwithin minutes after injury.TREATMENT OF SPINAL CORD INJURYAccording to medical authorities, an SCI is usuallycaused by an external force on the spine. The force causesthe spine to come into contact with the spinal cord andresults in damage to the cord. While specific methodsoftreating damage to the spine causing injuries to thespinalcord have been developed, there art no accepted methodspractice for treating damage to the spinal cord itself. inTreatment used on the individL4l patient will varythe level of injury and the amount of damage to the cord.withIn those injuries involving complete transection of thecord,all that is done is to heal the associated injuriesas effectively as possible and prevent the complicationsfollowparalysis. However, most SCI's are incomplete andwhichthe specific modes of treating incomple SCI are discussed below.Skull tractionSkull traction is used to correctdeformity and/ordislocation and immobilize the spine. spinalSeveral mechanicaldevices have been designed to provide the traction.As practiced at the VA Acute Spinal Cord Injury Centerin West Roxbury, Massachusetts, skull traction is performedafter diagnostic X-rays have been taken. The alignmentthe traction is adjusted in accordance with the X-rays. ofAssuming reduction in the deformity or dislocation isachieved with skull traction, the procedure isforone to eight weeks, depending on the level and continuedextent of theinjury. X-rays are taken to determine that healinghasoccurred before the traction is removed.12
Spinal fusionAccording to VA medical authorities, the primary indications for a spinal fusion operation are the failure of spontaneous healing with abnormal spinal mobility or increasingspine deformity. Fusion is also used with other surgicalprocedures. The level of the injury and the amount of damagewill determine whether the operation is to be performed andif so, the type of operation.Neurosurgeons at New York University Medical Center andBellevue Hospital Acute Spinal Cord Injury Center statedthat they normally use the fusion operation to realign thevertebrae of the spine. Misaligned vertebrae cause pressureon the spinal cord and increase damage. During the operation, the damaged vertebrae is removed and a piece of bone,taken from the patient's hip, is inserted into the area wherethe damaged vertebrae was removed. Once this has been accomplished, specially designed steel support rods are insertedinto the spine to add stability and to keep the proper alignment. Large doses of steroids are used to reduce swelling.LaminectomyA laminectomy is performed to relieve pressure on thespinal cord. It is an operation whereby the bony protectiveshields along the spine, the laminae, are removed and thevertebrae are realigned and stabilized. Officials at NewYork University Medical Center, Bellevue Hospital Acute SCICenter, and NIH said that laminectomy may produce increasedmobility of the spine. Such mobility, however, may increasecontusions and bruises of the spinal cord and could lead toincreased neurological damage.According to VA neurosurgeons, only if diagnosticstudies show material pressing on the spinal cord from thespine which correlates with the neurological damage shouldSuch an approach is sharedthe laminectomy be performed.by NIH authorities. In their opinion, the only reason toperform a laminectomy is to expose the spinal cord for othersurgical procedures.ACUTE SPINAL CORD INJURY CENTERSSome medical authorities told us that the quality ofspinal cord injury treatment in the United States isheavily dependent upon the experience and expertise of the13
personnel treating such an injury. These officials. saidthat due to the low incidence rates of SCI, it is unlikelythat the average hospital will have experienced peopletrained in dealing with SCI and cognizant of the importanceof proper treatment during the first few hours followingIn order to rectify this situatic :, some medicalinjury.officials said that a concept for treating acute SCI developed in England and now accepted generally in Europe shouldbe more widely used in the United States. This conceptinvolves establishing acute spinal cord injury centersthroughout the country. These centers were described bythe medical officials as a significant advance in treatingacute SCI.The acute spinal cord injury center concept was developed by Dr. Ludwig Guttman, a British neurosurgeon at theStoke-Mandeville Hospital in England. Guttman's conceptbegins with early case finding and referrals. It also consists of having highly trained emergency medical servicepersonnel, organized in comprehensive regional systems andprovided with proper equipment, communications, vehicles,and easily accessible medical facilities. Once the patientarrives at a center he is treated by a clearly defined teamof physicians, surgeons, specially trained nurses, and otherprofessionals ranging from physical therapists to vocationalrehabilitation counselors. The patient not only receivesservices from all these disciplines, directed and coordinated by a single physician in charge of his case, but hereceives these services concurrently. From acute carethrough rehabilitation he is followed by the same team.Rehabilitation services such as physical therapy, psychological counseling, and vocational planning begin as soon asacute medical and surgical procedures are accomplished. Thepatient is followed steadily by the physicians involved atthe acute stage, as well as by specialists such as urologistsand orthopedic surgeons.Some medical officials we interviewed stated thatemploying the acute SCI center concept does not require asubstantial construction program. On the contrary, theysaid the center should be a part of an existing hospital(preferably a hospital connected or affiliated with ateaching facility, such as a university) with a full complement of medical surgical services.Medical officials said a spinal cord unit should rangefrom a minimum of 20-30 beds to a maximum of 50-60 beds.Units smaller than 20 beds are unable to ensure a patient14
turnover rate sufficient to retain an incentive program forthe staff. Also. the financial burden on the hospitalwould be unbearab.e. Units over 60 beds become unwieldyand difficult to manage effectively, according to medicalauthorities.One person with sufficient training and experienceshould direct the spinal cord unit, accor
RSA Rehabilitation Services Administration SCI Spinal Cord Injury VA Veterans Administration. CHAPTER 1 INTRODUCTION In a letter dated October 8, 1976, five members of the Congress from Oregon requested that GAO conduct a study of spinal cord injury (SCI) costs in the United States and . Institute for Rehabilitation Medicine National .