Transcription
8/5/20Elizabeth Blecharczyk, MD, FAAPNeonatal HospitalistLucile Packard Children’s Hospital, StanfordClinical Assistant Professor, StanfordLucy Lee, MD, FAAPPediatric HospitalistPalo Alto Medical Foundation / LPCHSAdjunct Clinical Associate Professor, Stanford1July 27, 2020obgmanagement.comStandardized Screening inNeonates with AbnormalCord Blood Gases2DisclosuresWe have no financial disclosures.31
8/5/20Objectives1. Review evidence behind screening infants with abnormalcord gases to evaluate for risk of neonatal encephalopathy.2. Share an algorithm that standardizes clinical managementof infants with abnormal cord gases3. Discuss how to perform and score a Sarnat Exam4Background Neonatal encephalopathy estimated in 8.5 per 1,000 livebirths globally By 2 years of age, up to 60% of infants with encephalopathywill die or have severe disabilities Neuroprotective cooling is standard of care for newborns withmoderate to severe hypoxic ischemic encephalopathy (HIE) Infants at risk of HIE can have abnormal cord blood gases5Background For effective treatment, infants need to be evaluated withinthe first hour of life Timely evaluation ensures cooling can start within 6 hours Cord gases and clinical exam together are essential fordiagnosis. There needs to be clear communication andownership of who monitors and evaluates these infants.62
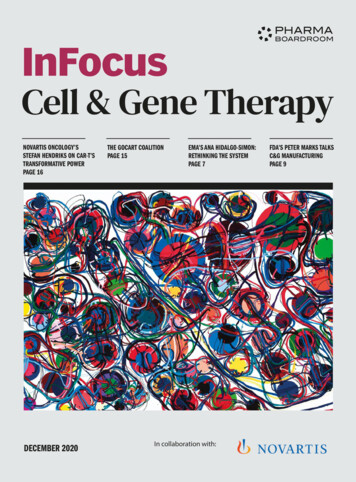
8/5/20What does a cord gas measure? It measures the acid-basestatus of the infant prior todelivery Can show signs of fetalhypoxic stressP om erance, J. J P erinatology (1999)7ACOG Recommendations for Obtaining Cord Gases1. C-section for fetal distress2. Abnormal heart tracing3. Chorioamnionitis/Intrapartum fever4. Low Apgar at 5 minutes5. Placental abruption6. Pre-eclampsia7. Multiple Gestations8. Maternal Thyroid Disease8Cooling is an Effective TreatmentCooling reduced the composite outcome of risk of death or majorneurodevelopmental disability at 18 months by 24%. The NNT was 7.Tagin et al. A rch P ediatr A dolesc M ed 201293
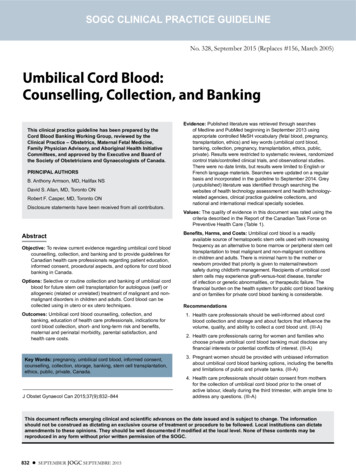
8/5/20Delivery Room CaseYou are called to a c-section due to failure to progress for a 32 yo F G2P1 at 40 2 with meconium and maternalchorioamnionitis diagnosed shortly prior to delivery. The infant is born floppy and apneic and is immediately taken to thewarmer. The infant requires PPV just over 1 minute but then has spontaneous respirations. The tone continues to bediminished but over the first 5 minutes of life shows continued improvement. By 8 minutes of life, the infant is placed skinto skin with its mother. Apgars are 3 and 8 at 1 and 5 minutes, respectively. At 30 minutes of life, you get a call from theL&D nurse with the following cord gases.Arterial cord blood gas: pH 7.1, BD 14Venous cord blood gas: pH 7.12, BD 13What do you do next?A: Nothing, the infant looks clinically wellB: Examine infant in the mother’s roomC: Bring infant to the newborn nursery, exam the infant and get an infant blood gasD: Transfer infant to higher level of care for evaluationE: None of the above10Clinical Exam to Corroborate Cord Gas FindingsCord gaspH 7.0orBD 10med.stanford.edu/newborn11StandardizedScreening forAbnormal Cord GasB irth0-30 m ins60 m ins60-120m ins124
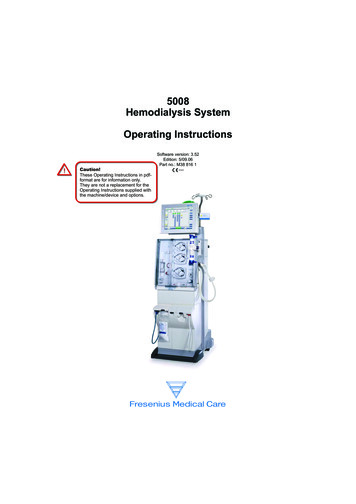
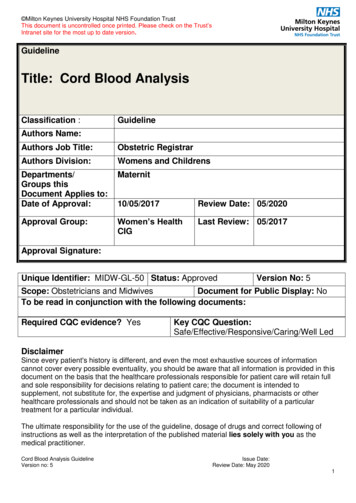
8/5/20StandardizedScreening forAbnormal Cord GasB irth0-30 m ins60 m insOUR CASEArterial cord bloodgas:pH 7.1, BD 14Venous cord bloodgas:pH 7.12, BD 1360-120m ins13Modified Sarnat dizedScreening forAbnormal Cord GasB irth0-30 m ins60 m insOUR CASEArterial cord bloodgas:pH 7.1, BD 16Venous cord bloodgas:pH 7.12, BD 13Normal Sarnat examRepeat Gas normal60-120m ins155
8/5/20Quality Improvement Metrics% Infants with ‘Abnormal’Cord Gas who had Direct Labto-Neonatal Hospitalist CallNotification% Infants with ‘Abnormal’Cord Gas who had a PostnatalBlood Gas and a documentedSarnat exam16StandardizedScreening forAbnormal Cord GasB irth0-30 m ins60 m ins60-120m ins17Future Considerations Is there a potential scenario on our algorithmwhere it would be appropriate to perform aSarnat exam without needing to repeat a gas?The role of cooling in infants who have mildencephalopathy based on Sarnat exam186
8/5/20Take-Home Points1. Pediatricians in the Delivery Room and Newborn Nurseryhave a key role in identifying and monitoring infants withabnormal cord blood gases to determine those at risk forneonatal encephalopathy.2. A timely Sarnat exam in addition to the cord gas is essentialwhen evaluating these infants.3. Having a standardized approach to clinically managing theseinfants leads to appropriate identification and treatment.19AcknowledgementsArun Gupta, MDKrista Birnie, MDAdam Frymoyer, MDKrisa Van Meurs, MDSonia Bonifacio, MDAlexis Davis, MD20Contact UsElizabeth BlecharczykLucy Leeebmorey@stanford.eduleelc1@sutterhealth.org217
8/5/20ReferencesACOG Committee on Obstetric Practice. ACOG Committee Opinion No. 348, November 2006: Umbilical cord blood gas and acid-base analysis. Obstet Gynecol 2006; 108:1319.Armstrong L, Stenson BJ. Use of umbilical cord blood gas analysis in the assessment of the newborn. Arch Dis Child Fetal Neonatal Ed. 2007;92(6):F430–F434.Committee on Fetus and Newborn. Clinical Report: Hypothermia and Neonatal Encephalopathy. Pediatrics 2014 onatal-therapeutic-hypothermia-toolkitJacobs SE et al. Cochrane Database Syst Review 2013;1:CD003311.James L S, Weisbrot I M, Prince C E. et al The acid-base status of human infants in relation to birth asphyxia and the onset of respiration. J Pediatr 1958. 52, 379–394.Lawn JE, et al. Estimating the causes of 4 million neonatal deaths in the year 2000. Intl J Epidemiol. 2006;35:706–718.Martinez-Biarge M et al. Predicting motor outcome and death in term hypoxic-ischemic encephalopathy. Neurology. 2011; 76(24):2055-2061.McAdams RM, Juul SE. Neonatal Encephalopathy: Update on Therapeutic Hypothermia and Other Novel Therapeutics. Clin Perinatol. O’Dea M et al. Management of Multi-Organ Dysfunction in Neonatal Encephalopathy. Frontiers in Pediatrics. 2020; 8(239): 1-17.Robertson CM, Perlman M. Follow-up of the term infant after hypoxic-ischemic encephalopathy. Paediatric Child Health 2006; 11:278–282.Shankaran S et al. Evolution of Encephalopathy during Whole Body Hypothermia for Neonatal Hypoxic-Ischemic Encephalopathy. J Pediatr 2012;160(4):567-572.e3.Shankaran S, et al. Childhood Outcomes after Hypothermia for Neonatal Encephalopathy. NEJM 2012; 366:2085-2092.Shankaran S. Therapeutic hypothermia for neonatal encephalopathy. Curr Treat Options Neurol. 2012;14(6):608–619.Tagin MA, et al. Hypothermia for Neonatal Hypoxic Ischemic Encephalopathy. Arch Pediatric Adolesc 2012; 166 (6), 558-566.22TimeSession TitlePresentersModerator11:00-11:05IntroductionA run G upta (S tanford)-CST(5 m inutes)A llison M arkow sky (C hildren’s N ational)11:05-12:00Top N ew born A rticles:CST(55 m inutes) 12:00-12:05B reak--C M V S creeningN ichole W ang (S tanford)A run G upta (S tanford)C ord B lood G as M anagem entE lizabeth B lecharczyk (S tanford)A llison M arkow sky (C hildren’sNASE arly O nset S epsisC C H D S creeningH ypoglycem iaD elivery R oomLana Ism ail (C hildren’s N ational)C handani D eZure (S tanford)N eha Joshi (S tanford)G ina G allizzi (C hildren’s N ational)R akhi G upta B asuray (N ationw ideC hildren’s)S tephanie Todd (C hildren’s N ational)CST(5 m inutes)12:05-12:35CST(30 m inutes)12:35-1:05 C S T(30 m inutes)Lucy Lee (S tanford – P A M F)N ational)B reak--1:10-1:55 C S TC O V ID -19 and N ew borns: A P anelA run G upta (S tanford)Lana Ism ail (C hildren’s N ational)(45 m inutes)D iscussionA llison M arkow sky (C hildren’s N ational)M elissa M auro-S m all (Tufts)1:55-2:00 C S TW rap-U pA run G upta (S tanford)1:05-1:10 C S T(5 m inutes)23(5 m inutes)-A llison M arkow sky (C hildren’s N ational)8
Arterial cord blood gas: pH 7.1, BD 14 Venous cord blood gas: pH 7.12, BD 13 Birth 0-30 mins 60 mins 60-120 mins Standardized Screening for Abnormal Cord Gas 13 https://wusthoff.people.stanford.edu/ Modified Sarnat Exam 14 OUR CASE Arterial cord blood gas: pH 7.1, BD 16 Venous cord blood gas: pH 7.12, BD 13 Normal Sarnat exam Repeat Gas normal .