Transcription
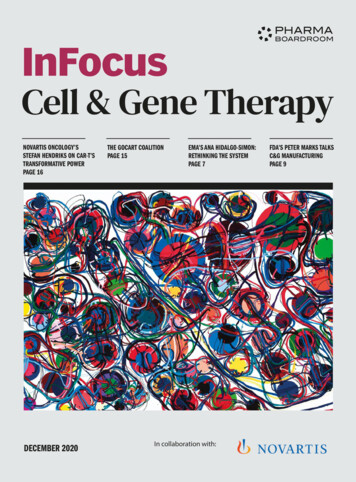
Review ArticleSpinal Cord Blood Supply and ItsSurgical ImplicationsAbstractMatthew W. Colman, MDFrancis J. Hornicek, MD, PhDJoseph H. Schwab, MDThe blood supply to the spine is based on a predictable segmentalvascular structure at each spinal level, but true radiculomedullaryarteries, which feed the dominant cord supply vessel, the anteriorspinal artery, are relatively few and their locations variable. Underpathologic conditions, such as aortic stent grafting, spinal deformitysurgery, or spinal tumor resection, sacrifice of a dominantradiculomedullary vessel may or may not lead to spinal cord ischemia,depending on dynamic autoregulatory or collateral mechanisms tocompensate for its loss. Elucidation of the exact mechanisms for thiscompensation requires further study but will be aided by preoperative,intraoperative, and postoperative comparative angiography.Protocols in place at our center and others minimize the risk of spinalcord ischemia during planned radiculomedullary vessel sacrifice.General Structure of SpinalCord Blood SupplyFrom the Department of OrthopaedicSurgery, Massachusetts GeneralHospital, Boston, MA.J Am Acad Orthop Surg 4-00219Copyright 2015 by the AmericanAcademy of Orthopaedic Surgeons.The spinal cord is nourished bya structure of arterial supply that follows a generally predictable path fromthe great vessels to the parenchymaof the white and gray matterthroughout the spinal cord (Figure 1).Segmental vessels originate from thegreat vessels of the neck, thorax,and abdomen at each segmentallevel and, with few exceptions, arepaired bilaterally. Although thesegmental vessel typically dividesinto an anterior and posteriorramus, the posterior ramus is thedominant vessel and divides furtherinto a muscular branch and a spinalbranch. The spinal branch becomesan anterior radicular artery anda posterior radicular artery as ittraverses the neuroforamen alongsidethe segmental nerve root. There are31 paired radicular arteries, one foreach segmental level, but relativelyfew of them contribute meaningfullyto the spinal cord. Most end withinthe nerve root, dura, or pial plexus.The radicular arteries that do contribute to the longitudinally orientedsingle anterior spinal artery (ASA),and therefore to the anterior twothirds of the spinal cord parenchyma,are named anterior radiculomedullary vessels. Gao et al1 demonstratedthe presence of 72 of these vesselsacross 20 human specimens, for anaverage of 3.6 per specimen. Conversely, Martirosyan et al2 cited anaverage of 10 (range, 2 to 17)throughout the spinal cord. Anteriorradiculomedullary arteries are usually not paired at any given level.Their end recipient vessel, the ASA,is mostly in continuity throughoutthe entire cord3,4 and experiencesboth anterograde and retrogradeflow, depending on the functionaldemand and location of dominantradiculomedullary feeder vessels.The ASA gives off many central arteries, which project and oftenbifurcate in the sagittal plane,October 2015, Vol 23, No 10Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.581
Spinal Cord Blood Supply and Its Surgical Implicationsischemic functional deficits whendisrupted. As opposed to the terminalbranches of the anterior system, thePSAs supply the cord matter ina centripetal pattern. Most anatomicstudies have not identified directanastomotic connections between theanterior and posterior systems,2whereas others have observed a connection in certain anatomic areas,such as around the conus medullaris.1In any case, significant overlap andredundancy does occur between theterminal supply branches of these twosystems within the parenchyma of thespinal cord itself.Figure 1Illustration of typical spinal cordblood supply under normalconditions. One radiculomedullaryvessel is shown, which supplies theanterior spinal artery througha hairpin loop.heading to the center of the cordmatter. These central arteries aremost dense in the lumbosacralregion, followed by the cervical andthoracic regions. These terminate incentrifugally oriented, inside-tooutside capillary beds, which arefive times as dense in gray as in whitematter.5The posterior one third of the cordparenchyma is supplied by pairedposterior spinal arteries (PSAs), whichare fed by the posterior radicular arteries. This arterial supply is moresimilar to an arterial plexus than to theoften-envisioned two longitudinalpaired arteries.6 Generally, these arteries are much smaller than the ASAand are less consequential in regard toStructure Unique to theCervical SpineThe ASA in the cervical spine takes itsorigin from two intervertebral arteries at the very upper end of thecervical spine, where it is largest, andslowly tapers to a constant diameterfor the remainder of the cervicalregion and into the thoracic region.7In the cervical spine, segmental vessels originate from the vertebral arteries in the upper portion and, in theremainder of the cervical spine, fromthe vertebral arteries and deep cervical, costocervical, or ascending cervical branches. The segmentals thengive off anterior and posterior radiculomedullary arteries, the former ofwhich supply the ASA, as in otherregions of the spine. There are typically from one to several dominantunilateral anterior radiculomedullaryvessels in the cervical spine.1,2Although the blood supply to thecervical spinal cord is generallythought to be redundant and wellcollateralized, significant variationexists in the number of dominantsupply vessels to the ASA, and theirnumber and distribution should bewell documented before consideringsurgical disruption.Structure Unique to theThoracic SpineIn the thoracic spine, the segmentalvessels come from the aorta or thesubclavian artery and continue on asintercostal arteries. The number ofradiculomedullary arteries in thethoracic spine is fewer than in otherareas (average, one to four), and theyare more spread out.3 There is poorcollateral potential in this region,and there is virtually no directcommunication between the central(anterior) and peripheral (posterior)systems.4 The ASA of the thoracolumbar spine is fed by one or twoanterior radiculomedullary vessels,the most dominant of which istermed the artery of Adamkiewicz(AA).8 This feeder vessel of the ASAcan be up to 1.3 mm in diameter andoccurs on the left side between T9and T12 in 75% to 80% of cases.9,10The AA gives off a dominant descending branch in a “hairpin”configuration and a much smallerascending branch as it joins the ASA.The ASA is typically continuousthroughout the thoracic spine, but itscaliber is significantly attenuated,especially as it approaches theAA.9,11-13 These factors are thoughtto be responsible for the sensitivity ofthe thoracic region to ischemic insultDr. Hornicek or an immediate family member has received research or institutional support from Stryker; has received nonincome support(such as equipment or services), commercially derived honoraria, or other non-research–related funding (such as paid travel) from Biomet;and serves as a board member, owner, officer, or committee member of the American Association of Tissue Banks and the InternationalSociety of Limb Salvage. Dr. Schwab or an immediate family member is a member of a speakers’ bureau or has made paid presentations onbehalf of Synthes and Stryker Spine; serves as a paid consultant to and serves as a board member, owner, officer, or committee member ofBiom’up; and has received nonincome support (such as equipment or services), commercially derived honoraria, or other non-research–related funding (such as paid travel) from Globus Medical and Stryker. Neither Dr. Colman nor any immediate family member has receivedanything of value from or has stock or stock options held in a commercial company or institution related directly or indirectly to the subject ofthis article.582Journal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
Matthew W. Colman, MD, et alof the anterior part of the spinalcord.Structure Unique to theLumbar and Sacral SpineThe tip of the conus medullaris maybe nourished by the descending termination of the ASA directly, but therealso exists a highly collateralizedanastomotic network at this locationtermed the anastomotic loop of theconus.7 The lower lumbar and sacralradicular arteries contribute to thishighly collateralized anastomoticnetwork rather than to the morecephalad ASA directly. Thus,although ligating a single artery ormultiple sacral or lumbar radiculararteries usually does not have ischemic consequences for the conus or thecephalad spinal cord, these vessels dosupply end arterioles to these regions.In fact, particulate matter cloggingthese end arterioles has resulted inlower extremity paraparesis, such aswith inadvertent intravascular particulate steroid injection in the lowerlumbar or sacral spine.14Spinal Cord IschemiaDuring PathologicConditionsSpinal cord perfusion pressure issimply a function of the distal aorticperfusion pressure (or mean arterialpressure) less the extrinsic cord pressure (or cerebrospinal fluid pressure).The blood supply to the spinal cordmay be interrupted iatrogenicallyduring many different types of surgical intervention, including aorticaneurysm repair, tumor resection,and spinal deformity surgery. Themechanism of spinal cord injury mayinvolve global hypoperfusion, as withaortic cross clamping or systemichypotension; selective ischemia fromligation of dominant segmental vessels; or secondary insult, such aswith reperfusion injury. The clinicalpresentation of cord ischemia rangesfrom complete paraparesis to asymptomatictransientabnormalitiesdetectable only by neuromonitoring.The key clinical question drivingmuch of the anatomic research inspinal cord ischemia during surgicalinterventions is which key vesselsmust be preserved to maintain spinalcord perfusion pressure and thereforespinal cord blood flow to avoid functional deficits.Thoracoabdominal AorticAneurysm RepairAlthough thoracoabdominal aorticaneurysm (TAAA) repair does nothave direct relevance for the orthopaedic surgeon, its related literature isthe most robust repository availablefor reports of ischemic spinal corddamage resulting from vascular interruption. In fact, TAAA repairs havebeen described as “Russian roulettefor the vascular surgeon”15 becauseof a reported high incidence of spinalcord ischemia, with rates of 16% to32%, depending on the location andextent of the aneurysm.16,17The mechanism of cord ischemia ismultifactorial but involves the extent ofdisruption of segmental vessels duringaortic mobilization and aneurysmrepair. Several studies have highlightedthe importance of preserving the dominant anterior radiculomedullary arteryto the thoracolumbar spine or theAA.18,19 In one study of open TAAArepairs, preoperative angiographicvisualization of the AA outside therepair or aortic clamp area resulted inno spinal cord injury. In addition, whenthe AA was located within the clampedsection, microrevascularization of theAA during the open procedure resultedin a 5% rate of cord ischemia compared with 50% when revascularization was unsuccessful.18However, because of the confounding effect of global hypoperfusionduring aortic cross clamping, studiesinvolving open TAAA repair may notbe the best model for examining theanatomic causes of spinal cord ischemia. Endovascular techniques, such asthoracic endovascular aortic repair,which selectively excludes specific segmental vessels by way of intra-aorticstents, may be a better model forexamining the effect of segmental vesselsacrifice on cord ischemia. In 71 patients undergoing TAAA endovascularrepair, Kawaharada et al20 observedless spinal cord injury in a group inwhom the AA was not occluded by thestent (none) compared with the groupin whom the AA was occluded (10%),but the difference was not significant,and the overall event rate was low(3.6%). Schurink et al21 analyzed 13patients undergoing stent grafting ofaneurysms at or below T8, 8 of whomhad four or more segmental levelsoccluded by the stent, and 6 of whomhad the segmental artery feeding theAA itself occluded. The authorsobserved two cases of intraoperativetransient motor evoked potentialabnormality correctable by raising themean arterial pressure, and no cases ofpostoperative paraplegia.21Although these and other studiesindicate that the AA can be safely andpermanently occluded at its moreproximal segmental supply, it isimportant to remember that the aorticand microvascular structures of patients with TAAA are chronicallydegenerative in nature and thus are notnormal. Chronic occlusion of segmental vessels may allow time for thedevelopment of collateral systems thatsupply the radiculomedullary vessels,thereby making sudden occlusion lesslikely to cause a catastrophic ischemicevent.22,23 A more rigorous model ofcritical cord blood supply may befound in other clinical scenarios.Spinal DeformityStudy of the neurologic effects of segmental vessel sacrifice demonstratesOctober 2015, Vol 23, No 10Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.583
Spinal Cord Blood Supply and Its Surgical Implicationsthat segmental vessels must be ligatedfor exposure during anterior thoracolumbar spine exposure and deformity correction; early reports raisedconcerns that sacrifice of segmentalvessels supplying dominant radiculomedullary vessels can lead to paraparesis. Apel et al24 reported on threecases of congenital kyphoscoliosis inwhich complete loss of somatosensoryevoked potential (SSEP) tracings wasobserved within 5 minutes after ligation of segmental vessels around thecurve apex from T3 to T9. Each caseresulted in postoperative paraparesis.This prompted the authors to institutea protocol in 44 patients wherebysegmental vessels being considered forligation were temporarily occludedbefore permanent ligation. In sevencases, SSEP amplitude changes of.50% were observed within 5 minutes of temporary occlusion of a segmental vessel at the curve apex; all ofthese returned to baseline within 5 to19 minutes after removal of theocclusive clamp and preservation ofthe vessel. No cases of postoperativeparaparesis were observed.24A temporary occlusion protocolbefore permanent segmental vesseldivision has been advocated by otherauthors.25 However, the importanceof this has also been brought intoquestion.4,26,27 Bassett et al4 studied15 patients undergoing anterior spinal surgery for kyphoscoliosis. Usingangiography, the authors identified32 total dominant radiculomedullary vessels supplying the thoracolumbar ASA in their population.Nine of these vessels in eight patientswere within the surgical field andwere temporarily occluded with noSSEP changes. However, in seven ofthese eight patients, other radiculomedullary vessels outside the surgical field were not occluded. Theeighth patient had no changes afterocclusion of the one dominant segmental vessel supplying the loneradiculomedullary vessel, but it waslocated at L1, an area known for584its rich perimedullary collateralsupply.4Another study retrospectively analyzed 1,197 patients who underwentanterior spinal surgery for kyphoscoliosis without using a regular temporary occlusion protocol beforedividing segmentals. There were nocases of postoperative paraplegia.However, in one patient, revision surgery on the convex side of the deformity was undertaken after priorsurgery on the concave side. In thispatient, the authors did temporarilyocclude the segmental vessels in thesurgical field, and for one vessel, therewere immediate SSEP changes; thus,the vessel was preserved.26 In additionto standard neuroprotective measures,such as avoidance of intraoperativehypotension, these and other authorsadvise dividing segmentals as far fromthe neuroforamen as possible, dividing segmentals unilaterally on theconvex side of the deformity only(which may play a lesser role in vascularization of the cord as a result ofchronic vessel tension), and considering temporary occlusion or “softclamping” when a thoracic-onlydeformity with intraspinal abnormality at the same levels is encountered.Oncologic Resection ofIntraspinal NeoplasmsResection of malignant neoplasms ofthe spinal axis using the technique oftotal en bloc spondylectomy presentsa distinct challenge with regard tomaintenance of spinal cord bloodsupply. Typically, a more extensive,often 360 exposure is required overat least two spinal motion segmentsto isolate the resection level for univertebral disease. Also, the tumorextent may make it impossible tosafely preserve certain vessels, even ifthere is preoperative concern for theircritical role in cord blood supply.Based on an early report that up tofour unilateral nerve roots and theiraccompanying radicular vessels canbe sacrificed in dogs without cordischemia,28 Nambu et al29 and Uedaet al30 undertook extensive experimental work investigating theimportance of preserving cordsupplying vasculature during totalen bloc spondylectomy. In severalinitial reports, these authors showedonly modest decreases (15% to25%) in spinal cord blood flowwithout change in motor evokedpotentials (MEPs) or spinal cordevoked potentials (SCEPs) afterbilateral three-level segmental vesselligation at T11-T13.29,30 This area indogs corresponds to the thoracicwatershed area in humans where theAA is most often located. In followup studies that sought to define thelimits of segmental vessel sacrifice inthis area without effect on cordhealth, these authors observed bloodflow to the cord dropping to lessthan half of normal only in dogs thathad bilateral five-level (44%) andseven-level (25%) segmental vesselsacrifice; in addition, only in dogswith five or more bilateral levelsligated were any MEP, SCEP, orneurologic examination abnormalities detected.31 In a refinement, thegroup studied segmental sacrificeover multiple levels that specificallyincluded the canine equivalent of theAA based on preoperative angiogram; only dogs with greater thanthree-level bilateral segmental vesselligations including the AA wereabnormal with regard to MEP, SCEP,and neurologic examination.32 It ison the basis of these studies that thisgroup currently advocates for safe,bilateral three-level segmental sacrifice, including the AA, in humans.These authors have retrospectivelyreported on their experience with 180cases of total en bloc spondylectomy inhumans; 15 had the AA involved at theresection level and underwent targetvertebra preoperative embolizationand three-level segmental vessel sacrifice, including the AA. There were noJournal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
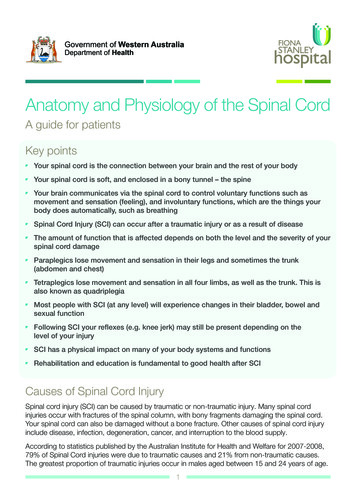
Matthew W. Colman, MD, et alFigure 2A through D, Illustration of disrupted spinal cord supply following ligation of a key segmental artery (shown in gray) (A) withthree possible compensatory mechanisms for reconstitution of the anterior spinal artery (ASA). Without direct supply to theASA via the typical flow from the segmental artery to the radiculomedullary artery (RMA), the ASA may be reconstituted bycollaterals emanating from an adjacent segment radicular artery (B), communication between the posterior spinal arterialsystem and the ASA system via the pial plexus and areas of spinal cord parenchymal overlap (C), or compensatory dynamicreversal of flow in the ASA itself using supply from distant RMAs or the anastomotic loop of the conus (D).cases of neurologic deterioration orparaplegia after surgery.33 Other authors have also suggested that ligatingthe AA may be safer than previouslythought and have demonstrated postoperative development of new collaterals to the ASA after AA ligation.34,35The explanations given for thesomewhat counterintuitive finding ofnormal spinal cord function afterligation of the dominant anterior radiculomedullary vessel to the ASA aretheoretical. Tomita et al36 claim thatthere must be anastomotic communication between the posterior spinalartery and anterior spinal artery systems through the intercanal, dural, orpial plexus (Figure 2, C). Some authors have corroborated this in a limited fashion in anatomic dissectionsby demonstrating communication atthe conus medullaris level,1 whereasothers have claimed that no functionalcommunication exists.2 Kawaharaet al37 have demonstrated that spinalshortening during total en blocspondylectomy may increase bloodflow to the cord. Other anatomicexplanations are that proximal ligation of a segmental artery or even ofan anterior radiculomedullary arteryitself does not disrupt the afferentsupply to the ASA because of preexisting, more distal contributions to thecritical anterior radiculomedullaryartery (Figure 2, B). These more distalcontributions may not be seen ona preoperative angiogram becausethey are dynamically recruited onlyafter the pathologic condition isinitiated. Finally, it is possible thatanterograde or retrograde flow dynamics through the ASA itself fromdistant cephalad or caudad anteriorradiculomedullary vessels compensatefor a given anterior radiculomedullarydivision (Figure 2, D).Monitoring and TimingFollowing the sacrifice of key spinalcord supply vasculature, the optionsfor intraoperative monitoring of deficit include SSEPs, continuous electromyographic monitoring (EMG),MEPs, and the intraoperative Stagnara wake-up test. SSEP monitoringremains the preferred method and isunlikely to be affected by anesthetics,but because it predominantly monitors the dorsal columns, it is at bestan indirect measure of the lateralcorticospinal tracts and the motorneurons, which are supplied by theASA. False-negative readings canoccur, with rates as high as 9%.38,39Free-running or continuous EMGmonitoring, like SSEP monitoring, isa good measure of individual nerveroot irritation during surgery andhas the benefit of detecting spontaneous nerve root activity in responseto stretch or compression. In contrast to both, transcranial MEPsdirectly measure the anterior cordmotor pathways. However, they aresusceptible to the anesthetic effectsof halogenated compounds, nitrousOctober 2015, Vol 23, No 10Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.585
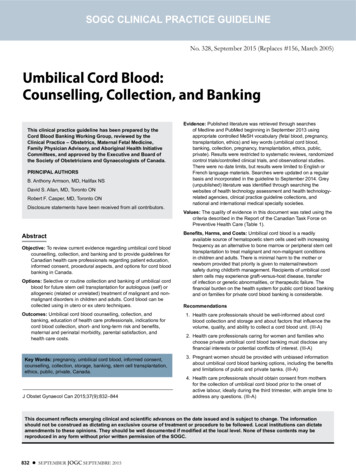
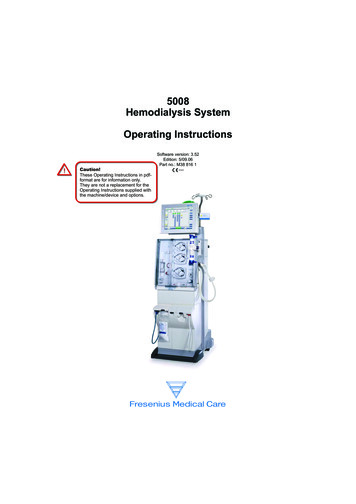
Spinal Cord Blood Supply and Its Surgical ImplicationsFigure 3Figure 5Midsagittal T2-weighted (A) and axial T1-weighted (B) postcontrast magneticresonance images of the spine in a 58-year-old woman with a history of smallcell osteosarcoma of the right hemipelvis depicting the tumor extent, withpathologic collapse of the vertebra and extraosseous epidural tumor extension.She presented with a solitary L1 metastasis 3 years after local and systemictreatment of her pelvic disease.Figure 4A and B, Spinal arterial angiography images with overlying radiograph of thesame patient shown in Figure 3, depicting the left-sided dominant thoracolumbarradiculomedullary artery, or artery of Adamkiewicz (black arrow). Filling of theanterior spinal artery is also seen (white arrow).oxide, or neuromuscular blockadeand are associated with complications from muscle contraction,intraoperative movement, and aberrant electrical signals affecting thebrain or cardiac systems.40 Mostauthors feel that a combinedapproach using SSEP and MEP is thesafest configuration, with a sensitivityand specificity for detecting cord586ischemia of 100% and 91%, respectively.41 The Stagnara wake-up test iseffective but used less commonlytoday because a relatively long lagtime is required to reverse anesthesiaand make an accurate determinationof cord function clinically.42Many authors have commented onthe timing of neurophysiologic monitoring changes after maneuvers thatSpinal arterial angiography image withoverlying radiograph depicting thecomparatively minor contribution ofa second radiculomedullary arterylocated on the left side at T10 in thesame patient shown in Figures 3 and 4.affect cord blood flow, but theduration is variable. MEP and SEPchanges have been reported to occurwithin 5 to 10 minutes after temporary or permanent occlusion ofkey segmental vessels and to returnto baseline in reversible scenarios,such as “soft clamping,” within 5 to19 minutes of clamp gic monitoring isthought to be an adequate proxyfor clinical motor function, thecorrelation is not perfect. Irreversible SSEP/MEP changes may indeedbe accompanied by postoperativeparaplegia, but not always, and thereverse is true, as well, wherebyfalse-negative readings occur.39 Thereport by Svensson et al16 of 1,509TAAA procedures had a 16% clinicalpostoperative neurologic deficit rate,but only 21% were observed in theimmediate postoperative period;32% were not observed for severaldays after surgery, and the range ofonset was 1 to 21 days.16 Neurologicdamage from altered blood supply iscomplex and may be related to localischemia, global perfusion dynamics,Journal of the American Academy of Orthopaedic SurgeonsCopyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
Matthew W. Colman, MD, et alreperfusion injury, or a combinationof the three.Figure 6Protective ManeuversStandard neuroprotective maneuversfor any surgical procedure involvingthe spinal cord include maintenanceof hemostasis, maintenance of meanarterial pressure, maintenance ofend-tissue oxygenation, and avoidance of mechanical stressors such asdistraction or rapid deformation.However, because spinal cord perfusion pressure is simply a function ofmean arterial pressure minus thecerebrospinal fluid pressure, othermethods have been developed tobalance this equation in a favorableway. One example is controlledcerebrospinal fluid drainage vialumbar cannulation of the intrathecalspace. A recent Cochrane review ofthree large trials investigating cerebrospinal fluid drainage in the settingof TAAA repairs found evidence,albeit limited, that cerebrospinal fluiddrainage improves neurologic outcome in open TAAA.44 Although lessgermane to tumor resection ordeformity surgery, another neuroprotective maneuver used duringTAAA repair involves distal aorticperfusion during cross-clamping ofthe aorta to maintain distal aorticperfusion pressure. A Cochranereview found no high-quality randomized studies to support thistechnique but did highlight severalobservational studies that suggesta neuroprotective effect withimproved outcomes.45 In addition,other authors have reported lowrates of neurologic complicationsduring TAAA using a protocol thatinvolves reimplantation of segmentalvessels previously divided for exposure;46-49 however, this protocol hasbeen called into question by others,19who have reported low rates ofneurologic compromise without reimplantation, and it is not commonlyPostoperative PA (A) and lateral (B) radiographs depicting the spinalreconstruction in the same patient shown in Figures 3 through 5, followingtotal spondylectomy of L1, with partial spondylectomies of T12 and L2, includingposterior segmental fixation, femoral allograft interbody reconstruction, Kanedatype rod fixation of the anterior vertebrae, and linkage of the posterior andanterior systems via a crosslink device.Figure 7A, Axial short tau inversion recovery (STIR) magnetic resonance image of thecervical spine in a 30-year-old woman who presented with a 2-year history of leftperiscapular shoulder pain demonstrating tumor encasement of the left vertebralartery and extensive left neuroforaminal involvement. B, Left-sagittal STIRmagnetic resonance image demonstrating the tumor extent across multiplesegments in the midcervical spine.October 2015, Vol 23, No 10Copyright ª the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.587
Spinal Cord Blood Supply and Its Surgical Implicationslimited support available for the useof cerebrospinal fluid drainage, evidence for most modalities is lacking.Figure 8Common Protocols at theAuthors’ CenterStandard (A) and reversed (B) spinal angiogram images in the same patientshown in Figure 7, demonstrating the lone dominant C5 radiculomedullary arteryand its contribution to the anterior spinal artery.Figure 9Postoperative AP (A) and lateral (B) radiographs of the cervical spinereconstruction, in the same patient shown in Figures 7 and 8.done at our center. Other potentiallyclinically useful maneuvers includeepidural or systemic cooling;50 also,recent experimental evidence in ani-588mals has demonstrated a neuroprotective effect of intravascularinjection of a direct free-radicalscavenger agent.51 Aside from theCurrently, to minimize the risk ofacute or postoperative ischemicinjury to the spinal cord during tumorresection, our group uses severalmethods in the preoperative, intraoperative, and postoperative stages.Preoperatively, we use angiographyto identify critical anterior radiculomedullary vessels, and we favora multidisciplinary approach to thepreoperative planning involving thoracic surgery, vascular surgery, andneurointerventional radiology. Wefrequently use preoperative embolization of the tumor levels, dependingon the presence of visualized collateral supply to the cord.Intraoperatively and postoperatively, we maintain the mean arterialpressure at .90 mm Hg; however,relatively higher pressures must bebalanced with intraoperative bleedingrisk. We use combined SSEP/MEPmonitoring for every case. In high-riskpatients, such as those with comorbidrisk factors for ischemia (eg, old age,peripheral vascular disease, kidneydisease) or with disease-related riskfactors (eg, planned sacrifice of majorradiculomedullary vessel or vertebral artery), we occasionally insertprophylacticcerebrospinalfluiddrains, which are initially clampedand used simply to monitor cerebrospinal fluid pressure. Depending onthe patient r
Spinal Cord Ischemia During Pathologic Conditions Spinal cord perfusion pressure is simply a function of the distal aortic perfusion pressure (or mean arterial pressure) less the extrinsic cord pres-sure(orcerebrospinalfluidpressure). The blood supply to the spinal cord may be interrupted iatrogenically during many different types of surgi-