Transcription
Society for Vascular Surgery (SVS) andSociety of Thoracic Surgeons (STS)Reporting Standards for Type BAortic DissectionsJoseph V. Lombardi, MD (SVS Co-Chair), G. Chad Hughes, MD (STS Co-Chair),Jehangir J. Appoo, MD, Joseph E. Bavaria, MD, Adam W. Beck, MD,Richard P. Cambria, MD, Kristofer Charlton-Ouw, MD, Mohammad H. Eslami, MD,Karen M. Kim, MD, Bradley G. Leshnower, MD, Thomas Maldonado, MD,T. Brett Reece, MD, and Grace J. Wang, MDDivision of Vascular and Endovascular Surgery, Department of Surgery, Cooper University Hospital, Camden, New Jersey; Division ofCardiovascular and Thoracic Surgery, Duke University Medical Center, Durham, North Carolina; Division of Cardiac Surgery, LibinCardiovascular Institute, Foothills Medical Centre, Calgary, Alberta, Canada; Division of Cardiovascular Surgery, Hospital of theUniversity of Pennsylvania, Philadelphia, Pennsylvania; Division of Vascular Surgery and Endovascular Therapy, University ofAlabama at Birmingham, Birmingham, Alabama; Division of Vascular and Endovascular Surgery, St. Elizabeth's Medical Center,Brighton, Massachusetts; Department of Cardiothoracic and Vascular Surgery, University of Texas Health Science Center at Houston,Houston, Texas; Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania; Department ofCardiac Surgery, University of Michigan, Ann Arbor, Michigan; Division of Cardiothoracic Surgery, Emory University School ofMedicine, Atlanta, Georgia; Division of Vascular Surgery, New York University Medical Center, New York, New York; Department ofSurgery, Division of Cardiothoracic, University of Colorado, Denver, ColoradoThis Society for Vascular Surgery/Society of ThoracicSurgeons (SVS/STS) document illustrates and definesthe overall nomenclature associated with type B aorticdissection. The contents describe a new classificationsystem for practical use and reporting that includes theaortic arch. Chronicity of aortic dissection is also definedalong with nomenclature in patients with prior aorticrepair and other aortic pathologic processes, such asintramural hematoma and penetrating atheroscleroticulcer. Complicated vs uncomplicated dissections areclearly defined with a new high-risk grouping that willundoubtedly grow in reporting and controversy. Followup criteria are also discussed with nomenclature for falselumen status in addition to measurement criteria anddefinitions of aortic remodeling. Overall, the documentprovides a facile framework of language that will allowmore granular discussions and reporting of aorticdissection in the future.(Ann Thorac Surg 2020;-:---)Ó 2020 by The Society of Thoracic Surgeons and theSociety for Vascular SurgeryDr Charlton-Ouw has a financial relationship withMedtronic and W. L. Gore & Associates.This article has been copublished in The Annals of Thoracic Surgery and theJournal of Vascular Surgery.The Society of Thoracic Surgeons requests that this document be citedas follows: Lombardi JV, Hughes GC, Appoo JJ, Bavaria JE, Beck AW,Cambria RP, Charlton-Ouw K, Eslami MH, Kim KM, Leshnower BG,Maldonado T, Reece TB, Wang GJ. Society for Vascular Surgery (SVS) andSociety of Thoracic Surgeons (STS) Reporting Standards for Type B AorticDissections. Ann Thorac Surg. 2020 (in press).Independent peer-review and oversight has been provided by the members of the STS and SVS Document Oversight Committees. STS OversightCommittee: Jennifer S. Lawton, MD (Chair), Anders Ahlsson, MD, PhD,Mark F. Berry, MD, Justin D. Blasberg, MD, Traves D. Crabtree, MD, JoelDunning, FRCS, PhD, Melanie A. Edwards, MD, Michael P. Fischbein,MD, PhD, Mario F.L. Gaudino, MD, Michael E. Jessen, MD, Michael S.Ó 2020 by The Society of Thoracic Surgeons andthe Society for Vascular SurgeryPublished by Elsevier Inc.Kent, MD, Onkar V. Khullar, MD, R. Scott McClure, MD, SM, GaetanoPaone, MD, MHSA, Daniel P. Raymond, MD, Thomas A. Schwann, MD,MBA, Craig H. Selzman, MD, A. Laurie W. Shroyer, PhD, MSHA,Matthew L. Williams, MD, Stephanie G. Worrell, MD, Moritz C. Wylervon Ballmoos, MD, PhD. SVS Oversight Committee: Thomas Forbes, MD(Chair), Ruth Bush, MD, JD, Ronald Dalman, MD, Mark Davies, MD, PhD,Mahmoud Malas, MD, MHS, Cynthia Shortell, MD, Keith Calligaro, MD,Gregory Landry, MD, Katherine McGingle, MD, MPH, Marc Schermerhorn, MD, Neal Barshes, MD, MPH, Alik Farber, MD, MBA, SheppardMondy, MD, Yazan Duwayri, MD.Address correspondence to Dr Lombardi (SVS Co-chair), Division ofVascular and Endovascular Surgery, Department of Surgery, CooperUniversity Hospital, 3 Cooper Plaza, Ste 411, Camden, NJ 08103; email:lombardi-joseph@cooperhealth.edu.0003-4975/ 005
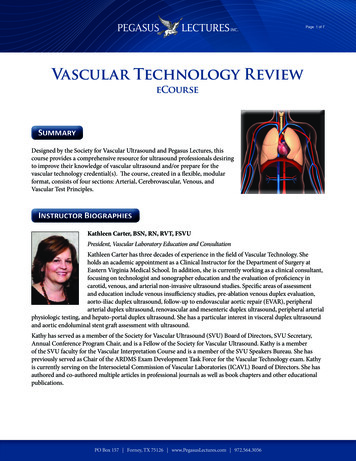
2REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONSSection 1. IntroductionPurpose of the DocumentAcute aortic dissection is the most common emergencyaffecting the human aorta, with high mortality andmorbidity without appropriate and time-sensitive treatment. Based on data from the International Registry ofAcute Aortic Dissection (IRAD),1,2 patients with acutetype B dissection composed approximately 33% of alldissection patients enrolled in the registry across a 17year period. Management of acute type B dissection hasevolved over time and now includes medical, surgical,and endovascular therapies performed by several specialties, including vascular surgery, cardiothoracic surgery, interventional radiology, and cardiology.With the recent blanket U.S. Food and Drug Administration (FDA) approval of endovascular stent grafting fortype B aortic dissection (TBAD) as well as our maturingunderstanding of the anatomy and pathophysiology ofthe disease, there has been an explosion of literature inmultiple specialty journals regarding TBAD presentation,treatment, and outcomes. As such, the purpose of thisdocument is to provide structure to the reporting ofTBAD, with particular attention to those attributes ofTBAD that, based on the best available evidence to date,would appear to have an impact on outcomes. Priorreporting standards from the Society for Vascular Surgery(SVS) have addressed thoracic endovascular aortic repair(TEVAR) in a more general sense,3 although these earlierstandards did not specifically address aortic dissection.Given the complexity of the topic, it is believed to warranta separate publication. This combined effort by the SVSand the Society of Thoracic Surgeons (STS) provides aunified consensus on reporting, nomenclature, and classification of TBAD at this point in time.Organization of the Writing CommitteeThe committee was headed by two co-chairs, one eachfrom the SVS and STS, with each co-chair responsible forAnn Thorac Surg2020;-:---a group of six writers evenly balanced between the societies. Each group was then further broken down intothree dyads (one SVS and one STS) who were assigned aspecific section of the document, the content of which wasfurther refined by the co-chairs. The completed draftdocument was then approved by all members of theWriting Committee. The document was subsequentlyreviewed by the SVS and STS document committees andthe FDA, and it was available for societal public comments. The final document was approved by the SVS andSTS document oversight committees after final editing bythe Writing Committee’s co-chairs based on the feedbackreceived in the review process.Section 2. Anatomic Classification of ThoracicAortic DissectionClassification systems for thoracic aortic dissection allowcaregivers to communicate accurately when describingaortic disease and are critical for triage, treatment, andprognostic purposes. Historically, classification systemsrelied on the anatomic location of intimal entry tears andlongitudinal extent of the dissection flap. The originalDeBakey classification, first described in 1965, definesaortic dissection according to anatomic features. Themore widely adopted Stanford classification simplifiedthe earlier DeBakey classification and is based onwhether the ascending aorta is affected. In type A, theascending aorta is involved; whereas in type B, theascending aorta is spared, with the entry tear distal to theleft subclavian artery (Figure 1). Unlike the DeBakeyclassification scheme, the Stanford classification does notcharacterize the distal extent of dissection.4Importantly, neither classification scheme addressesaortic dissections that originate in the arch. In arch dissections, the dissection flap or intramural hematoma(IMH) typically involves the transverse arch and oftenspares the proximal ascending aorta (Figure 2). The entrytear may originate in the arch itself or distal to the leftFigure 1. DeBakey and Stanford classification systems for aortic dissection.
Ann Thorac Surg2020;-:---REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONS3Figure 2. (A) Threedimensional computed tomography angiography(CTA) reconstruction of anaortic dissection (arrow)involving the aortic arch.(B) Coronal CTA image ofthis same aortic dissectionclearly demonstrating thelocation of the primary tearin the arch (arrow).subclavian artery and extend retrograde to the level of theinnominate artery or even the distal ascending aorta.Often, the dissection extends into the great vessels themselves. A recent query of IRAD for all patients presentingwith acute type B dissection with an identifiable primaryintimal tear found evidence for retrograde arch extensionin 16.5%. This finding did not appear to have an impact onmanagement strategy or early and late death, suggestingthat retrograde arch extension may be analogous toTBAD.5 However, without a standardized method of classifying aortic arch dissections, reporting of outcomes inthese patients remains cumbersome and haphazard.Given these limitations, the Writing Committeethought a new classification system relevant to currenttreatment paradigms was necessary to more preciselydescribe aortic arch involvement in aortic dissection.Within the new SVS/STS classification scheme for aorticdissection, the distinction between type A and type B ispredicated on entry tear location alone. In a type Adissection, the entry tear originates only in zone0 (Figure 3). The distal extent of a type A aortic dissectionis then simply designated by zone. For example, a type A9dissection represents a dissection entry tear in zone0 with distal extension of the dissection into zone 9(Figure 4). Type B dissections include any aortic dissection with an entry tear originating in zone 1 or beyond.Type B dissections are further characterized by two subscripts (BP,D); subscript P describes the proximal zone ofinvolved aorta, and subscript D describes the distal zoneof involved aorta. Involved aorta includes both patent andthrombosed false lumen as well as IMH. For example, B1,9denotes a type B dissection with proximal involvement ofzone 1 and distal extension to the level of zone 9(Figure 5), although the primary entry tear may be anywhere between zones 1 and 9. TBAD may also involve theascending aorta, designated B0,D in that the primary entrytear originated in zone 1 or beyond yet extended proximally to zone 0 (Figure 6). If the entry tear origin is notidentifiable, the dissection will remain indeterminatewith the designation I. These dissections will alwaysinvolve zone 0 or otherwise would be sensibly designatedtype B. Indeterminate dissections will follow the sameformat for distal extent as type A. Therefore, an indeterminate dissection extending from zone 0 to zone 9 wouldbe designated I9 until further imaging or gross anatomicfindings at surgery identify the origin of the primaryentry tear; thus, the I designation may be impermanent. Idissections that are subsequently determined to be type B(ie, primary entry tear in zone 1 or beyond) may require adifferent treatment algorithm and may have a naturalFigure 3. Society for Vascular Surgery/Society of Thoracic Surgeons(SVS/STS) Aortic Dissection Classification System of dissectionsubtype according to zone location of primary entry tear.
4REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONSAnn Thorac Surg2020;-:---Figure 4. An aortic dissection with an entry tear in zone 0 is classified as type A. In the example illustrated, the dissection processextends distally to zone 9, such that the dissection is fully classifiedas A9.Figure 5. An aortic dissection with an entry tear in zone 1 or beyondis classified as type B. In the example illustrated, the entry tear is inzone 3 and the dissection process involves zone 1 proximally andextends distally to zone 9; the dissection is fully classified as B1,9.history that differs from true type A dissection. As such,the Writing Committee thought a separate I classificationwould allow more precise description of dissection typefor future research reporting of outcomes for aorticdissection involving zone 0 with differing entry tearorigins.Using this new SVS/STS classification system will allowclinicians to conceptually project a precise image of entrytear location and proximal and distal dissection extentwith one simple designation (Figure 7). It is not necessarily the intent of the Writing Committee that the newclassification system should completely replace the current Stanford and DeBakey systems for everyday clinicaluse, especially for practitioners who are not subjectmatter experts in aortic disease. This classification systemis intended for research reporting, such as comparativeeffectiveness studies, where it will allow more granulardescription of study populations and disease processesparticularly relating to arch involvement.Classification of new aortic dissection after priordissection with or without repair (ie, acute-on-chronicdissection) can be difficult. Patients with a history ofprior type A or type B dissection (repaired or unrepaired)now presenting with a new acute dissection should bereported both to historic dissection pathology, type ofprior repair (if any), and current “residual” anatomy. Forexample, patients who present with new acute disease ina medically managed chronic state may be classified asacute-on-chronic AD or BP,D. Similarly, patients with prioraortic surgery managed in the chronic phase and nowpresenting with acute disease would be described as residual acute-on-chronic AD or BP,D.Central repair of type A dissection, for instance, cancarry multiple surgical solutions, such as aortic valveresuspension with supracoronary ascending tube graft;aortic root replacement (eg, Bentall, valve sparing), withor without concomitant hemiarch or total arch replacement; and total arch replacement, also potentiallyincluding conventional or frozen elephant trunk repair.Residual arch and descending aortic disease after centralaortic repair (ie, remaining type B after type A repair) isthesubjectofongoinginvestigation.6Open
Ann Thorac Surg2020;-:---REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONS5Figure 7. Society for Vascular Surgery/Society of Thoracic Surgeons(SVS/STS) Aortic Dissection Classification System.Figure 6. Example of an aortic dissection with an entry tear in zone2, which classifies it as type B. The dissection process involves zone0 proximally and extends distally to zone 9. This dissection is fullyclassified as B0,9.false, lumen for blood flow is externally bound only bythe outer third of the media and adventitia. IMH, incontrast, lacks an identifiable direct communication between the true and false lumens, a condition that authorsin Asia have described as “closed thrombosed falselumen.”7 It is characterized by a hyperdense, crescentshaped hemorrhage within the aortic wall best seen onnoncontrast-enhanced computed tomography (CT) imaging (Figure 9).8 Several mechanisms for IMH have beenproposed, including spontaneous rupture of the vasavasorum, which causes bleeding and hematoma formation within the aortic wall (Figure 10).9 Others have suggested microscopic tears in the intima as the potentialcause.8,9 Differentiating aortic dissection and IMH can bechallenging, and the two conditions may coexist in thereconstruction, endovascular repair, and hybrid procedures should therefore describe zones of residual diseasewith defined proximal and distal anastomoses and landing zones. For instance, a patient with a prior type Aproximal aortic repair now presenting with a symptomatic chronic arch and descending thoracic dissectionextending to the iliacs may be referred to as a residualB1,11. Classifying this as a residual dissection infers thefact that this patient has undergone prior surgery. Weanticipate a significant amount of reporting for management of these situations in the future.Dissection vs IMHIn addition to aortic dissection, two other distinct yetrelated acute aortic diseases require further descriptionwith respect to proper reporting: IMH and penetratingatherosclerotic ulcer (PAU). Aortic dissection is definedby the presence of a tear in the intima that results in aseparation of the layers of the media and allows blood toflow through the false lumen (Figure 8). This separate, orFigure 8. Type B aortic dissection (TBAD) with visualization ofentry tear (arrow) in the descending thoracic aorta.
6REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONSAnn Thorac Surg2020;-:---Figure 9. Noncontrast-enhanced computed tomography (CT) scandemonstrating intramural hematoma (IMH) of the descendingthoracic aorta. Note that the IMH appears bright on nonenhancedimaging.same patient. IMH can also progress to frank aorticdissection.PAU is defined as an atherosclerotic lesion that penetrates the internal elastic lamina of the aortic wall and isoften diagnosed in the presence of an IMH. PAUs are alsoreferred to as ulcer-like projections, especially in Asia7(Figure 11, A). Approximately 20% of PAUs have noassociated IMH, presumably because of medial fibrosisfrom chronic atherosclerotic disease.9,10 PAU rupture riskis directly related to ulcer depth. However, PAU withIMH (Figure 11, B) has a higher risk of aortic rupture andportends a worse clinical course compared with a similarsized PAU without IMH.11,12 It is important to distinguishbetween true aortic dissection and IMH in reportingas treatment algorithms and outcomes may differ significantly. The extent of IMH should be reported accordingto zone, as with aortic dissection, and reporting shouldinclude the maximal thickness of the aorta in the zone ofIMH. PAU is best characterized by ulcer dimensions(saccular depth and diameter of aortic origin) and location by zone. When pathologic processes coexist with oneanother, we suggest using the predominant disease forclassification purposes. Patients with multiple PAUsshould be subscripted with their zone locations (eg, forPAU involving zones 3 and 5, PAU3,5). If concomitantIMH is present, one would add subscripted proximal anddistal extent, IMHP,D, as described before. Thus, for apatient with IMH extending from zones 2 to 9 presentingwith concomitant PAU in zones 3 and 5, it would bedescribed as IMH2,9 with PAU3,5.Chronicity Classification of Aortic DissectionThe historical chronicity classification of aortic dissectionoriginated from the investigations of Hirst and colleagues,13 who observed that mortality in patients withtype A and type B aortic dissection significantly decreasedafter 14 days. Using this time point, the authors definedacute aortic dissection as 14 days from symptom onsetand chronic aortic dissection as 14 days from symptomonset. Since this original report, there have beenFigure 10. Example of the gross pathologic appearance of anintramural hematoma (IMH), in this case of the ascending aorta, asseen during central repair for acute type A IMH.significant advancements in diagnostic imaging, medicaltreatment, and endovascular and surgical therapy and animproved understanding of the pathophysiologic mechanism of aortic dissection. Therefore, a reappraisal of thisclassification system is warranted.A key motivation to re-evaluate the chronicity classification system is the application of endovascular therapyto TBAD. TEVAR was initially described in the treatmentof TBAD in 1999 and has transformed the management ofthis disease during the past 20 years.14 TEVAR, along withhigh-resolution CT scans and intravascular ultrasound,has afforded a more sophisticated understanding ofdissection flap properties with respect to the chronicity ofthe dissection. In the acute phase, the dissection flap isthin and highly compliant, with a curvilinear appearanceon CT scan. As the dissection flap ages, it becomes thickerand less compliant and has a straightened appearance onCT (Figure 12).15 This enhanced understanding ofdissection flap pathophysiology has implications for theclassification of the chronicity of TBAD, and therefore anyclassification system should incorporate these morerecent observations pertaining to intimal flap remodeling.These lessons learned from contemporary reports inthe endovascular era have prompted a reassessment ofthe traditional chronicity classification system. In a studysimilar to the initial work of Hirst, Booher and
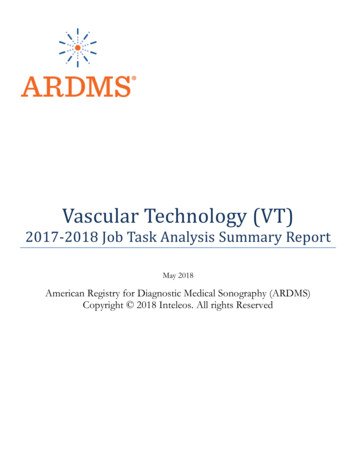
Ann Thorac Surg2020;-:---REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONS7Figure 11. (A) Penetrating atherosclerotic ulcer(PAU) without intramuralhematoma (IMH). (B) PAUwith associated IMH andleft pleural effusion.colleagues16 examined mortality from the time of symptom onset in 1800 patients (TBAD n ¼ 655) from the IRADdatabase. In this cohort, Kaplan-Meier survival curvesdemonstrated distinct strata of mortality risk that variedby chronicity following presentation with aortic dissection. In addition, several studies examining various aorticremodeling outcomes in patients with TBAD treated withTEVAR at different time points have suggested theestablishment of an additional subacute classification.17,18The subacute phase of TBAD was defined as 15 to 30 daysby an SVS report on early outcomes after TEVAR forcomplicated TBAD.19 However, the most recent EuropeanSociety of Cardiology guidelines on the diagnosis andtreatment of aortic disease defined the subacute phase as15 to 90 days.20 In a study analyzing patients who underwent TEVAR within 3 months of the time of dissection, there was no significant difference in remodelingresults of the thoracic aorta between those patientstreated at 14 days and those treated between 15 and90 days.21 The cumulative data from these reports has ledthe Writing Committee to develop the followingclassification system of dissection chronicity, which incorporates both the IRAD and European Society of Cardiology findings: hyperacute, 24 hours; acute, 1 to14 days; subacute, 15 to 90 days; and chronic, 90 days(Table 1).Section 3. Causes and Risk FactorsVarious causes and risk factors for acute TBAD have beennoted in the literature, several of which influencedecision-making and affect short- and long-termmorbidity and mortality. Included here are the morecommon causes reported in studies on acute TBAD, theincidence of which among the study population should bedescribed in any reports on TBAD.HypertensionHypertension was present in 80.9% of patients who presented with acute TBAD in the IRAD database.2 In previous reports summarizing the experience at a tertiarycare center, 71% of patients with acute dissection wereFigure 12. Changing morphology of a type B dissection over time by computed tomography in a single illustrative patient with multiple goodquality images at the same aortic level. Please note: 1) marked early increase in aortic diameter (orange arrow); 2) intimal thickening over time(orange star); 3) decreased flap motion over time (orange triangles); 4) flap straightening over time (green star); and 5) increased false lumenthrombosis over time (yellow star). Evolution of aortic dissection flap morphology over time demonstrating transition from acute to subacute tochronic dissection. (From Peterss S, Mansour AM, Ross JA, Vaitkeviciute I, Charilaou P, Dumfarth J, and colleagues. Changing pathology of thethoracic aorta from acute to chronic dissection: literature review and insights. J Am Coll Cardiol 2016;68:1054-65. Reproduced with permission.)
8REPORTLOMBARDI ET ALSTANDARDS FOR TYPE B AORTIC DISSECTIONSTable 1. Society for Vascular Surgery/Society of ThoracicSurgeons (SVS/STS) Chronicity Classification of AorticDissectionChronicityTime From Onset of SymptomsHyperacuteAcuteSubacuteChronic 24 hours1-14 days15-90 days 90 daysnoted to have a history of hypertension,22 whereas inmore contemporary reports, 62% of patients with acuteTBAD were taking antihypertensive medications at presentation.23 However, the use of antihypertensive medications as a surrogate for the diagnosis of hypertension isalmost certain to underestimate the true incidence of thisrisk factor in the TBAD population, given that TBAD isoften a disease of the socioeconomically disadvantagedwho are less likely to comply with risk factormodification.24Patients who are reported as having hypertensionshould meet the definition according to the 2017 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults,25 whichcategorizes hypertension into two stages. Stage 1 isdefined as systolic blood pressure of 130 to 139 mm Hg ordiastolic blood pressure of 80 to 89 mm Hg. Stage 2 isdefined as systolic blood pressure 140 mm Hg or diastolic blood pressure 90 mm Hg.Genetically Triggered Aortic DiseaseGenetically triggered aortic diseases are due to mutationsthat affect the aorta and its branches and include disorders affecting mainly the aorta (nonsyndromic) as well assyndromic conditions (associated with abnormalities ofother organ systems).26,27 Many of the syndromic conditions are well-characterized connective tissue disorders(CTDs) with altered phenotypic tissue of multiple organs,including the cardiovascular system, leading to increasedrisk of aortic aneurysm formation and aortic dissection.Various syndromes have been described, with causativegenetic mutations identified for some. The most wellknown CTDs include Marfan syndrome (MFS), LoeysDietz syndrome (LDS), and Ehlers-Danlos syndrome.Patients reported as having MFS should meet criteria ofthe revised Ghent nosology,28 an expert panel’s revisionof the Ghent nosology from 1996 that outlines combinations of clinical features, family history, and genetictesting diagnostic of the disorder. Of note, the presence ofan FBN1 gene mutation is not, in and of itself, enough toestablish the diagnosis. Reporting patients with CTD isimportant because these syndromes have been shown tomediate outcomes of aortic dissection. For example, inhospital mortality of patients with MFS and acute TBADis lower compared with that of patients without CTD.MFS patients also have better outcomes after open surgery for TBAD, although they have higher reinterventionrates.1Ann Thorac Surg2020;-:---LDS, as originally described, is characterized by heterozygous mutations in the type 1 or type 2 subunit of thetransforming growth factor (TGF) b receptor. Patientsmay exhibit a clinical triad of hypertelorism, bifid uvulaor cleft palate, and arterial tortuosity with ascendingaortic aneurysm or dissection.29 Emerging data suggestsignificant heterogeneity in the severity of aortic diseaseamong patients with LDS, and patients with TGFBR2mutations (LDS type 2) appear to have more severe disease requiring aortic surgery at younger ages.30 As such,reports of series including LDS patients should includespecific details of the mutations present in each patient toallow comparison across studies. An expanded definitionof LDS has also been proposed, as follows: type 1, TGFBR1mutation; type 2, TGFBR2 mutation; type 3, SMAD3 mutation; and type 4, TGFB2 mutation.31Vascular Ehlers-Danlos syndrome is caused by mutations in COL3A1 gene encoding type III collagen. Whereasdissection or rupture typically occurs in medium-sizedarteries, aortic involvement has also been reported.29Outcomes in this population are particularly poor, givensevere vessel fragility that complicates any attempt atsurgical repair, whether open or endovascular, and themedian age of death is 48 years.32Familial thoracic aortic aneurysm and dissection(FTAAD) represents a heterogeneous group with thoracicaortic disease predominating. Genetic mutations inACTA2 are most commonly identified (10%-14% ofFTAAD), but mutations in FBN1, TGFBR1/2, and MYH11have also been found.29In total, at least 29 genes have been identified to datethat are associated with the development of thoracicaortic aneurysm and dissection, with many more likelyto be discovered in the future.27 As such, all reportspertaining to TBAD should include a description of theincidence of these disorders among the studypopulation.CongenitalSeveral congenital anomalies are associated with anincreased risk of aortic dissection. Bicuspid aortic valve,the most common congenital cardiac malformation, occurs in up to 2% of the population and can be found inconjunction with genetic syndromes (eg, MFS, LDS,FTAAD) or in isolation. An increased prevalence ofthoracic aortic aneurysm and dissection in patients withbicuspid aortic valve may have a genetic basis related tomutations in any one of several genes, includingNOTCH1, ACTA2, KCNJ2, and GATA, but a unifying genetic mutation has not yet been identified.33Coarctation of the aorta, a narrowing near the ductusarteriosus/ligamentum arteriosum, occurs in 6% to 8% ofpatients with congenital heart disease and is the mostfrequent congenital anomaly found in patients withTurner syndrome (45,XO). It is also associated with aorticmedial degeneration, dilation or aneurysm of the aorticroot and ascending aorta, and aortic dissection. Coarctation has been found in 2% of patients with aortic dissection,34 and there are multiple case reports in the literature
Ann Thorac Surg2020;-:---dating to the 1960s of coarctation and aortic dissectionpresenting simultaneously.Kommerell diverticulum, the term given to aneurysmal dilation of the proximal segment of an aberrantsubclavian artery, was first described by the radiologistBurckhard Kommerell in 1936.35 He observed, onbarium swallow study, the dela
Houston, Texas; Division of Vascular Surgery, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania; Department of Cardiac Surgery, University of Michigan, Ann Arbor, Michigan; Division of Cardiothoracic Surgery, Emory University School of