Transcription
Vascular Technology (VT)2017-2018 Job Task Analysis Summary ReportMay 2018American Registry for Diagnostic Medical Sonography (ARDMS)Copyright 2018 Inteleos. All rights Reserved
Page 2ContentsACKNOWLEDGEMENTS . 3EXECUTIVE SUMMARY . 4BACKGROUND OF STUDY . 4METHODOLOGY . 4Job Task Analysis Working Group . 4Survey Questionnaire Development . 4Survey Process . 4Survey Administration Procedure . 4Response Rates. 42nd Mini JTA Survey. 4Data Analysis. 5SURVEY RESULTS . 6Demographics and Backgrounds of Participants . 6Gender . 6Race and Ethnicity . 6Location of Practice . 6Education . 7Work Experience . 8Work Environment . 9Breakdown of Time. 10Conclusion . 13Discussion of Results . 13Final Approval by JTA Working Group . 13Approved VT Content Outline . 14
Page 3ACKNOWLEDGEMENTSThis study was completed through the work of many individuals at Inteleos, who worked together to construct the survey,administer the survey, and analyze the data. Eight subject matter experts also volunteered many hours to draft and reviewmaterials before and after the survey was administered. Thanks to the 1200 ARDMS sonographer registrants around thenation and other countries who took the time and interest to participate in the job task survey.
Page 4EXECUTIVE SUMMARYSurvey Questionnaire DevelopmentThe American Registry for Diagnostic MedicalSonography (ARDMS) is the globally recognized standardof excellence in sonography. ARDMS is responsible forthe preparation of valid and reliable certificationexaminations in the field of sonography. Conducting jobtask analyses (JTAs) at the national and international levelsfacilitates ARDMS in evaluating the current practiceexpectations and performance requirements of thespecialty. The 2017 Vascular Technology (VT) JTA wasdesigned to collect information on the sonography-relatedwork activities sonographer registrants perform in practice.The results of the JTA were used in updating the testcontent outline, which guides content distribution of theVT Examination. This report details the methodology,data collection and analysis, and survey results. It alsoincludes the test content outline that resulted from theJTA.ARDMS contracted with The Caviart Group, a certificationand testing consulting group, to facilitate a kick-offmeeting. During this meeting that was conducted on June22nd, 2017, the JTA Working Group developed the task listand demographic questions to include on the survey. Tasksand demographic questions from previous job task surveyswere used as a starting point in this development. The JTAWorking Group reached consensus on a list of 73 tasks tobe used in the survey. The survey questionnaire was pilottested with the eight members from the JTA WorkingGroup and six validation group members.BACKGROUND OF STUDYThe American Registry for Diagnostic MedicalSonography (ARDMS) recognizes that diagnostic medicalsonography is a valuable tool in the healthcare industry.There are several healthcare professions that are utilizingsonography in practice to increase the efficacy of theirpatient care.Successful mastery and demonstration of the knowledgeand skills required to hold ARDMS sonographercredentials will provide sonographers with an additionalsource of validation. This will support the veracity of thediagnostic medical sonography exams that thesepractitioners perform.Survey ProcessSurvey Administration ProcedureThe survey was made available to participants as a webbased survey through the survey platform Qualtrics . Aninvitation to participate in the survey was sent via email tothe prospective respondents.ARDMS sent the JTA survey to 2,546 registrantscredentialed since 2001. These registrants were selectedrandomly using a stratified sampling method so that thesample was representative of all ARDMS sonographerregistrants in terms of specialty, gender, and geographicregion. The survey was made available to the participantsfor two weeks between October 10th and October 24th,2017. All responses made by the participants were keptconfidential.Response RatesMETHODOLOGYA total of 1,350 (53% of those sampled) sonographersresponded to the survey. Of these, 1,258 (93% ofrespondents) reported that they currently perform vasculartechnology sonography. The data analysis was based onthe responses from the 1,258 sonographers currentlyperforming vascular technology sonography.Job Task Analysis Working Group2nd Mini JTA SurveyA JTA Working Group consisting of eight subject matterexperts (SMEs) led this project. The eight JTA WorkingGroup members were volunteers and some were membersof the Assessment Committee.A second survey was sent out to participants through thesurvey platform Qualtrics on February 9th, 2018 andremained open until February 23rd,, 2018. The survey wassent to 390 individuals and consisted of two tasks thatwere not included in the original JTA survey. The ratingsfrom these two tasks were aggregated with the originalsurvey. Among the 186 surveys that were started (for a
Page 5response rate of 48%), 163 respondents stated that theycurrently performed Vascular Sonography, and of thatgroup, 155 respondents rated both tasks that made up thebody of the survey.Data AnalysisRespondents were asked the following questions for eachtask: 1) How frequently do newly certified vascularsonographers perform this task? and 2) How important isthe task in affecting clinical decisions and patientoutcomes? The frequency and importance rating scaleswere scored 1-5. The response options for the frequencyscale were Never (1), Rarely (2), Occasionally (3), Often(4), and Always (5). The response options for theimportance scale were Not Important (1), SomewhatImportant (2), Important (3), Very Important (4), andCritically Important (5).The frequency and importance rating scales werecombined into a single measure of overall criticality(ranging from 0-16) using a hierarchical method in whichvalues on the importance scale outweigh or outrank allvalues on the frequency scale, with the exception of‘Never’ (see Table 1). Higher criticality values indicate themost critical tasks for a sonographer performing diagnosticmedical sonography examinations. These criticality valueswere averaged for each task and rank ordered andreviewed by the JTA Working Group. In addition, thecriticality values were summed within each domain. Thesum of criticality for each domain is divided by the overallcriticality score to determine the initial percentages of theexamination content in each domain.Survey Response OptionsImportanceCritically Important (5)FrequencyAlways (5)Overall CriticalityScore16Often (4)15Occasionally(3)Rarely (2)14Always (5)12Often (4)11Occasionally(3)Rarely (2)10Always (5)8Often (4)7Occasionally(3)Rarely (2)6Always (5)4Often (4)3Occasionally(3)Rarely (2)2Not Important (1)All options0All optionsNever (1)0Very Important (4)Important (3)Somewhat Important(2)Table 1: Construction of Overall Criticality Scale13951
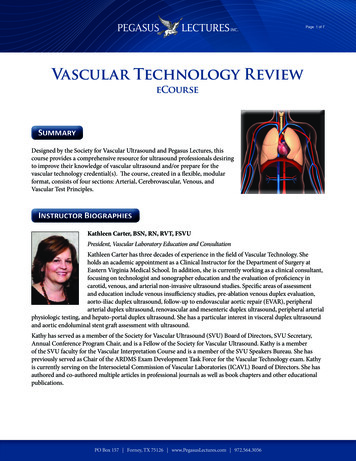
Page 6SURVEY RESULTSDemographics and Backgrounds ofParticipantsOf the 1,258 participants who were currently practicingvascular technology sonography, 1,095 completed thedemographics portion of the JTA survey, and this sectionis based on those 1,095 participants.GenderApproximately 84% of the respondents were female and16% were male (Figure 1). One (1) respondent selected‘Other’ and seven (7) declined to answer (see Figure 1).Figure 2Location of PracticeOf the respondents who reported the country in whichthey practice, 94% reported practicing in the United Statesand 3% in Canada, with the other 3% of respondentspracticing in 19 other countries (see Table 2).Table 2: Location of PracticeFigure 1Race and EthnicityApproximately 74% of respondents were white orCaucasian, 11% of respondents were Asian, 4% black orAfrican American, 7% Hispanic or Latino, and 1%American Indian. Additionally, 3% of respondentsmarked “other” (see Figure 2). Less than 1% ofrespondents selected Native Hawaiian or Other PacificIslander (not shown), and 2% of respondents selectedmore than one race/ethnicity.Location of PracticeUnited States of AmericaCanadaOtherCount10313830Percent94%3%3%
Page 7Among US residents who provided the US state theypractice in, over a third (37%) practiced in the southernregion of the United States (as defined by the US CensusBureau), followed by the Midwest where 26% of USresidents practiced (see Figure 3).Figure 4Figure 3EducationApproximately 41% of respondents had a Bachelor’sdegree and 41% had an Associate’s degree as their highestlevel of education (see Figure 4). Within sonographyspecific education, 45% of respondents had an Associate’sdegree and 32% of respondents had a certificate programas their highest level of education (see Figure 5).Figure 5
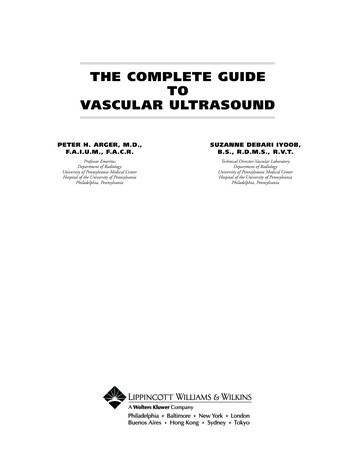
Page 8Almost all (94%) of respondents received the majority oftheir education in the United States, 3% in Canada, and theremaining 3% of respondents were educated in 17 othercountries around the world (see Table 3).Table 3: Location of EducationLocation of EducationUnited States of AmericaCanadaOtherCount Percent1030383094%3%3%A little over half of respondents (55%) had opportunitiesto continue their education provided by their employers(see Figure 6).Figure 7Around a third (31%) of respondents performed between26 and 50 vascular exams each month, and about a quarter(24%) performed more than 100 vascular exams a month(see Figure 8).Figure 6Work ExperienceApproximately 39% of respondents had been practicingsonography for 5 years or less, and 37% had beenpracticing for 6 to 10 years (see Figure 7).Figure 8
Page 9Seventeen percent (17%) of respondents reported thatthey were sonography educators (see Figure 9).The most common number of sonographers inrespondents’ labs was less than 5 (42%) followed by 6 to10 (31%) (see Figure 11).Figure 11Figure 9Work EnvironmentThe respondents were asked to indicate the type ofenvironment in which they perform most of theirsonographic examinations. The most common response(36%) was a non-university hospital (see Figure 10).Respondents were asked how many vascular exams theirlab performed each month, and 46% of respondentsreported that their lab performed over 200 vascular examsper month (see Figure 12).Figure 12Figure 10
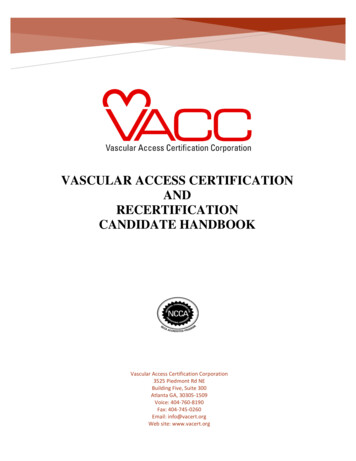
P a g e 10Breakdown of TimeRespondents were asked to elaborate how theirprofessional time is spent. A significant portion (195)responded that they spent 50% ( 5%) of their timeperforming vascular ultrasound, and 154 respondentsreported that they spent exactly 100% of their timeperforming vascular ultrasound. The mean percentage oftime that respondents spent performing vascularultrasound was 61%. 1027 respondents answered thisquestion (Figure 13).Figure 13Respondents who reported that they were sonographyeducators were asked what percentage of time they spentas a sonography educator, and the most common responsewas 30% ( 5%) with 41 respondents. The meanpercentage of time respondents who were sonographyeducators spent as a sonography educator was 43%. 156respondents answered this question and were only asked ifthey reported that they were a sonography educator(Figure 14)Figure 14
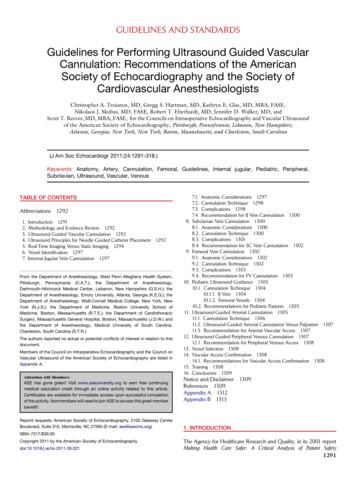
P a g e 11Respondents were asked the percentage of time they spentperforming research, and the most common response was0% with 205 respondents. More than half of therespondents (289 respondents) reported spending between0% and 5% of their time performing research. The meanresponse was 14%. 552 respondents answered thisquestion (Figure 14).
Figure 14Page 12 of 18
ConclusionWhen the survey concluded, Inteleos staff analyzed the results to determine criticality ratings of each of the task statements.These results were used to develop an initial list of tasks and domain weightings. This list was shared with the JTA WorkingGroup via a Qualtrics survey to allow JTA Working Group members to review and provide feedback prior to the“Discussion of Results” call.Discussion of ResultsA call was held March 20, 2018 to discuss the survey results with the JTA Working Group. Seven of the eight members of theJTA Working Group and seven Inteleos staff members were in attendance. The call was facilitated by The Caviart Group. Theoverall frequency, importance, and criticality statistics were presented in rank order of criticality by domain and subdomainbased on the survey data. Each task was reevaluated for inclusion in the final list based on the JTA Working Group’s opinionand criticality scoring from the survey participants. The JTA Working Group decided to lower the number of tasks from 75 to47, discarding tasks with low criticality ratings or other content issues and reducing redundant tasks.The JTA Working Group also reviewed the preliminary content outline based on the data and the outline based on their taskremovals/combinations to decide what percentage of the examination should be in each domain. The JTA Working Groupcould deviate 10% in each domain from the preliminary content outline based on the 47 tasks. Table 3 shows this processand the resulting domain weightings.Table 4: Content domain breakdown after the JTA Working Group review of survey resultsOrder Domain# TasksCriticalitySum% ormal Anatomy, Perfusion and1 FunctionPathology, Perfusion and2 FunctionSurgically Altered Anatomy and3 Pathology4 Physiologic examsUltrasound-guidedProcedures/Intraoperative5 AssessmentPhysical Principles,Instrumentation, Quality6 Assurance, and SafetyPreparation, Documentation and7 CommunicationTotalFinal Approval by JTA Working GroupAfter the call, the JTA Working Group completed an approval survey (administered April 18-April 25, 2018). Some questionswere raised, and minor edits proposed through the survey. The proposed edits were reviewed, clarified and minor edits weremade. There were no changes made to the final tasks and domain weightings. The Chair of the JTA Working Group approvedthese changes on a call held on April 27, 2018. The ARDMS council voted and approved this content outline on June 24,2018.Page 13 of 18
Approved VT Content Outline(Outline Summary)#DomainSubdomainNormal Anatomy, Perfusion, andFunctionEvaluate normal anatomy, perfusion, function12Pathology, Perfusion, and FunctionEvaluate pathology, perfusion, and functionSurgically Altered Anatomy andPathologyPhysiologic ExamsEvaluate surgically altered anatomy and ve AssessmentParticipate in ultrasound-guidedprocedures/intraoperative assessment6Quality Assurance, Safety, and PhysicalPrinciplesParticipate in quality assurance activities and monitorsafetyApply physical principles7Preparation, Documentation, andCommunication34Percentage21%Perform physiologic arterial examinationsPerform physiologic venous examinationsPrepare for examinationDocument and communicate findings32%6%12%7%14%8%(Detailed Outline)1.Normal Anatomy, Perfusion, and Function1.A.Evaluate normal anatomy, perfusion, andfunction1.A.1.1.A.2.Aortoiliac vasculatureUpper extremity .10.1.A.11.Lower extremity veinsNative upper extremity arteriesNative lower extremity arteriesMesenteric vasculatureRenal vasculatureHepatoportal systemInferior vena cava and/or iliac veinsExtracranial cerebrovascular systemIntracranial cerebrovascular exams(transcranial Doppler (TCD) andtranscranial imaging (TCI))Vein mapping1.A.12.Knowledge and/or skill related to normal anatomy,perfusion, and functionAbility to assess vasculatureAbility to assess organs related to vasculature (liver,kidney, spleen, pancreas, gallbladder, thyroid, etc.)Ability to recognize and apply proper scan technique inobtaining and documenting diagnostic imagesAbility to recognize, evaluate, and document congenitalanomaliesAbility to recognize and document normal vascular flowpatterns using spectral, color, and power DopplerKnowledge of hemodynamics as it relates to normalanatomyKnowledge of sonographic appearance of anatomy,landmarks, and vascular structuresPage 14 of 18
2.Pathology, Perfusion, and Function2.A.Evaluate pathology, perfusion, and function2.A.1.Aortoiliac disease (atherosclerosis, aneurysm,dissection, etc.)Venous insufficiencyUpper extremity venous disease (thrombosis,thoracic outlet syndrome, extrinsiccompression, etc.)Lower extremity venous disease (thrombosis,extrinsic compression, .9.2.A.10.2.A.11.2.A.12.2.A.13.2.A.14.3.Native upper extremity artery disease(atherosclerosis, aneurysm, dissection,thoracic outlet syndrome, etc.)Native lower extremity artery disease(atherosclerosis, aneurysm, dissection,extrinsic compression, etc.)Mesenteric vasculature disease(atherosclerosis, aneurysm, dissection,thrombosis, extrinsic compression, etc.)Renal vasculature disease (atherosclerosis,aneurysm, dissection, thrombosis,extrinsic compression, fibromusculardysplasia, etc.)Hepatoportal system disease (thrombosis,Budd-Chiari syndrome, portalhypertension, etc.)Knowledge and/or skill related to pathology,perfusion, and functionAbility to assess abnormal vasculatureAbility to assess organs related to abnormal vasculature(liver, kidney, spleen, pancreas, gallbladder, thyroid,etc.)Ability to identify pathologyAbility to identify anatomic variantsAbility to identify and communicate critical findingsAbility to recognize and document abnormal vascularflow patterns using spectral, color, and power DopplerAbility to recognize and apply proper scan technique inevaluating and documenting pathologyAbility to identify and document incidental findingsKnowledge of pathophysiology of vascular diseaseKnowledge of hemodynamics as it relates to pathologyKnowledge of sonographic appearance of abnormalanatomy and vascular structuresInferior vena cava and/or iliac vein disease(thrombosis, extrinsic compression, etc.)Extracranial cerebrovascular diseaseIntracranial cerebrovascular disease (TCD andTCI) (for stroke, for vasospasm, agitatedsaline for patent foramen ovale (PFO), forintraoperative emboli monitoring, etc.)Incidental findings (thyroid mass, Baker cyst,carotid body tumor, etc.)Critical findings (aneurysm, acute deep veinthrombosis, critical stenosis, etc.)Surgically Altered Anatomy and Pathology3.A.Evaluate surgically altered anatomy andpathology3.A.1.Dialysis accessKnowledge and/or skill related to surgically alteredanatomy and pathologyPage 15 of 18
2.5.5.A.5.A.1.5.A.2.5.A.3.5.A.4.Post intervention (endovascular aneurysmrepair (EVAR), inferior vena cava (IVC)filter, venous ablation, bypass grafts,transjugular intrahepatic portosystemicshunt (TIPS), stents, etc.)Transplanted organsPhysiologic ExaminationsPerform physiologic arterial examinationsManually calculate pressure indices (anklebrachial index (ABI), segmental pressures,etc.)Obtain appropriate diagnosticwaveforms/pressures with and withoutprovocative/exercise maneuversSelect the appropriate instrumentation(photoplethysmography (PPG) sensors,cuffs, presets, protocols, etc.)Perform physiologic venous examinationsObtain appropriate venousphotoplethysmography (PPG) diagnosticwaveforms (with and without tourniquets;plantar flexion and dorsiflexion)Select the appropriate venousphotoplethysmography (PPG)instrumentation (sensors, presets,protocols, etc.)Ultrasound-guidedProcedures/Intraoperative AssessmentParticipate in ultrasound-guidedprocedures/intraoperative assessmentParticipate in manual compression ofpseudoaneurysmsProvide guidance for thrombin injections ofpseudoaneurysmsProvide guidance for venous ablationproceduresObtain appropriate post-proceduraldiagnostic imagesAbility to evaluate post-procedural vasculature (afterEVAR, IVC filter, venous ablation, bypass grafts, TIPS,stents, etc.)Knowledge of sonographic appearance of surgicallyaltered anatomy/vasculatureKnowledge of hemodynamics as it related to surgicallyaltered anatomy and pathologyKnowledge of common causes of failure/rejection ofsurgically altered anatomy/vasculatureKnowledge of surgical procedures related to dialysisaccess, bypass grafts, stents, organ transplants, venousablation, etc.Ability to understand an operative report and its impacton sonographic appearance and techniqueKnowledge and/or skill related to physiologicexaminationsAbility to evaluate effects of limb size and cuff diameterKnowledge of provocative/exercise maneuvers and theireffect on circulationAbility to optimize recordingsAbility to evaluate effects of tourniquet onhemodynamicsKnowledge of placement of venous PPG sensors andtourniquetsKnowledge of effects of tourniquet on hemodynamicsKnowledge and/or skill related to ultrasound-guidedprocedures/intraoperative assessmentAbility to provide guidance during a procedureKnowledge of appropriate procedural imaging: preprocedure, during procedure, and post-procedureKnowledge of contraindications to a procedureKnowledge of expected post-proceduralfindings/potential complicationsKnowledge of instrumentation and its appropriate useKnowledge of sonographer's role during procedureKnowledge of procedure protocol and required resourcesPage 16 of 18
6.6.A.6.A.1.6.A.2.6.A.3.Quality Assurance, Safety, and PhysicalPrinciplesParticipate in quality assurance activitiesand monitor safetyAssess the appropriateness of the exam (perindications, by applying Appropriate UseCriteria, etc.)Compare exam findings to correlative studiesCollaborate regarding exam protocols(including discussions, optional images,modifications, timing, and diagnosticcriteria)6.A.4.Monitor patient condition (including safetyand comfort)6.B.6.B.1.Apply physical principlesIdentify artifacts related to vascular imaging,and document and/or modify the exam asneededCalculate, perform, and analyze resistiveindices and acceleration timesPreparation, Documentation, andCommunicationPrepare for examinationAdapt the exam to clinical setting and patientcondition (patient position, physicalenvironment, medications, etc.)Review and confirm patient information(patient identity, clinical history, previousimaging studies, lab findings,interventions, etc.), and communicateexam process to patient6.B.2.7.7.A.7.A.1.7.A.2.7.B.Knowledge and/or skill related to quality assurance,safety, and physical principlesAbility to provide appropriate patient careAbility to apply Appropriate Use CriteriaAbility to correlate vascular exam findings with otherimaging modalitiesAbility to utilize appropriate exam protocolsKnowledge of exam protocolsKnowledge of implications of various laboratory valuesKnowledge of other imaging modalities (MRI, CT,conventional angiography, etc.)Knowledge of scanning techniques andpatient/sonographer positioningKnowledge of contraindications to a vascular examAbility to adjust study to minimize artifactsKnowledge of artifacts, their causes, and theirimplications on the studyKnowledge and/or skill related to preparation,documentation, and communicationAbility to obtain and evaluate patient historyAbility to correlate information from various types ofimaging studiesAbility to establish rapport and interview patientAbility to interpret and follow patient identificationprotocolsAbility to synthesize information from various sources inthe patient's medical historyAbility to select correct instrumentation based onprotocol and patient body habitusAbility to modify exam based on patient condition andbody habitusKnowledge of appropriate preparations for the testKnowledge of implications of patient position, physicalenvironment, and patient condition on vascular exams(hydrostatic pressure, etc.)Knowledge of signs and symptoms pertaining to thevascular examKnowledge of potential effects of patient medications onexamKnowledge of appropriate indications andcontraindications for vascular examsDocument and communicate findingsPage 17 of 18
7.B.1.Document preliminary impression/findingsand technical limitations, and verifyimages are appropriately archived forinterpretationAbility to utilize resources, such as physicians, literature,or peersAbility to modify exam based on real-time findingsAbility to communicate professionally with patient andproviderAbility to document preliminary impression/findings andtechnical limitationsAbility to verify that exam is properly archivedKnowledge of technical limitations of vascular examsKnowledge of protocol for critical findings notificationPage 18 of 18
performing vascular ultrasound, and 154 respondents reported that they spent exactly 100% of their time performing vascular ultrasound. The mean percentage of time that respondents spent performing vascular ultrasound was 61%. 1027 respondents answered this question (Figur