Transcription
Report of the SpecialCommission onRACIALINEQUITIESIN MATERNALHEALTHCOMMONWEALTH OF MASSACHUSETTSSPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTHa
About the Special Commission on RacialInequities in Maternal HealthThe Special Commission on Racial Inequities in Maternal Health wascreated by a legislative act signed by Governor Charlie Baker in January2021. The 28-member body’s charge was to investigate and studymethods to reduce racial inequities in maternal health.This is the final report of the Special Commission on Racial Inequities inMaternal Health.The report, executive summary, and other information about theCommission are available on the General Court of the Commonwealthof Massachusetts website 9MAY 2022
TABLE OF CONTENTSSpecial Commission Members 02Acknowledgments03List of Acronyms04Executive Summary05Introduction 081 Family and Community Engagement10Family and Community Engagement, Call to Action222 Public Health Infrastructure26Public Health Infrastructure, Call to Action363 Healthcare Systems Improvement41Healthcare Systems Improvement, Call to Action52Conclusion53Sources54Appendices58A. Chapter 348 of Acts of 202059Family and Community Engagement, Task Force Call to Action 25B. Participants in Stakeholder Listening Sessions61C. Glossary of Terms 64D. Directory of Organizations 65E. H.2341/S1519 Fact Sheet 67F.H.3881 Fact Sheet 69
Special Commission on Racial Inequities in Maternal HealthHOUSE AND SENATE CHAIRSOF THE JOINT COMMITTEE ONPUBLIC HEALTHRepresentative Marjorie Decker,25th Middlesex DistrictSenator Jo Comerford, Hampshire,Franklin, and Worcester DistrictCHAIR OF THE MASSACHUSETTSBLACK AND LATINO LEGISLATIVECAUCUS (DESIGNEE)Representative Liz Miranda,5th Suffolk DistrictCOMMISSIONER OF THEDEPARTMENT OF PUBLICHEALTH (DESIGNEE)Dr. Hafsatou Fifi Diop, MD, MPHEXECUTIVE DIRECTOR OF THEHEALTH POLICY COMMISSION(DESIGNEE)Jasmine Bland, MPHAPPOINTMENTS BY THE HOUSEAND SENATE CHAIRS OF THEJOINT COMMITTEE ON PUBLICHEALTHMember of the MassachusettsMaternal Mortality and MorbidityReview CommitteeDr. Allison Bryant, MD, MPHMember of the MassachusettsMedical Society who shall specializein childbirth or maternal health,including, but not limited to,obstetrics and gynecology, maternalfetal medicine, or family medicineDr. Charles Anderson, MD, MPH,MBA, President & CEO,Dimock Center02MAY 2022 REPORTMember of the MassachusettsChapter of the American College ofObstetricians and Gynecologistswho shall specialize in childbirthor maternal health, including,but not limited to, obstetricsand gynecology, maternal-fetalmedicine, or family medicineDr. Teju Adegoke, MDMember of the Massachusettsaffiliate of American College ofNurse-MidwivesSusan J. Hernandez, CNM, MSN,FACNMMember of the Perinatal-NeonatalQuality Improvement Network ofMassachusettsDr. Audra Meadows, MD, MPH,FACOG, Co-Director, PNQIN MAMember of the Ellen StoryCommission on PostpartumDepressionDr. Leena P Mittal, MD, FACLPMember of the MassachusettsCOVID-19 Maternal Equity Coalitionwho is a public health professionalspecializing in racial inequities inmaternal healthDr. Ndidiamaka AmutahOnukagha, PhD, MPH, Founder andDirector, MOTHER Lab Medical professional who practicesin a birthing center working withwomen who experience highor disparate rates of maternalmortality or severe maternalmorbidityGinny Miller, CNM, Co-owner, SevenSisters Midwifery and CommunityBirth Center. She services asignificant number of Medicaidclients and many birthing peoplewho despite being low risk, typicallyexperience higher rates of maternalmortality or severe morbidity.Through the midwifery model ofcare, evidence-based practice andawareness of the diverse needsof the community, her practice isworking to demonstrate that betteroutcomes are achievable.Doula from the Birth SistersProgram at Boston Medical CenterLinda SpencerCertified Professional Midwife fromSister Soul Midwifery, LLCStephanie Johnson, DEM, CLC, CBERepresentative of the Bridgesto Moms Program at HealthcareWithout Walls, Inc.Dr. Jo-Anna Rorie, PhD, MSN, MPH,CNMRepresentative of the ResilientSisterhood Project, Inc.Lilly Marcelin, Executive DirectorRepresentative of Quietly United inLoss Together CorporationNneka Hall, FounderRepresentative of theCommonwealth Mental Health &Wellness Center, Inc.Leah Randolph, Executive DirectorA person who identifies as a fatherwho belongs to a community thatexperiences high or disparate ratesof maternal mortality or severematernal morbidityDr. Charles C. Daniels, Jr., LICSW,M.Div., PhD, Co-founder & CEO,Fathers’ Uplift, Inc.A parent whose partner hasexperienced maternal mortalityor severe maternal morbidityand belongs to a community that
experiences high or disparate ratesof maternal mortality or severematernal morbidityRobert SabaMember of the MassachusettsCOVID-19 Maternal Equity Coalitionwho is a maternal peer recoverycoach working with women whoexperience high or disparate ratesof maternal mortality or severematernal morbiditySoraya DosSantos,a member of theSouthcoast Massachusetts regionthat is an expert in maternal healthand postpartum careMember from communities thatexperience high or disparate ratesof maternal mortality or severematernal morbidityGlorimar Irizarry, Program Directorfor Children and Adolescents,Holyoke Health CenterMember from communities thatexperience high or disparate ratesof maternal mortality or severematernal morbidityMorgan Taylor, MPA, AssistantDirector of the Boston HealthyStart InitiativeMember from communities thatexperience high or disparate ratesof maternal mortality or severematernal morbidityDr. Craig S. Andrade, RN, MPH,DrPH, Associate Dean for Practice/Activist Lab Director at BostonUniversity School of Public HealthMedical professional who shallspecialize in pediatricsDr. Renée Boynton-Jarrett,MD, ScD, Associate Professor ofPediatrics, Boston Medical Center/Boston University School ofMedicine and Founding Director,Vital Village NetworksAPPOINTMENTS BY THEGOVERNORA person who has lost an immediatefamily member because ofmaternal mortality and belongsto a community that experienceshigh or disparate rates of maternalmortality or severe maternalmorbidityDonnette McManusA person who has experiencedsevere maternal morbidity andbelongs to a community thatexperiences high or disparate ratesof maternal mortality or severematernal morbidityAngela MiddletonCORE WORKING GROUPDr. Ndidi Amutah-OnukaghaDr. Renée Boynton-JarrettSen. Jo ComerfordDr. Charles DanielsRep. Marjorie DeckerDr. Hafsatou Fifi DiopDr. Audra MeadowsAngela MiddletonRep. Liz MirandaFamily and Community EngagementWorking GroupDr. Renée Boynton-JarrettDr. Charles Daniels, Jr.Soraya DosSantosDonnette McManusRep. Liz MirandaMorgan TaylorRobert SabaPublic Health InfrastructureWorking GroupDr. Craig AndradeSen. Jo ComerfordDr. Hafsatou Fifi DiopSoraya DosSantosDr. Leena MittalLeah RandolphMorgan TaylorHealthcare Systems ImprovementWorking GroupDr. Teju AdegokeDr. Ndidiamaka Amutah-OnukaghaDr. Charles AndersonJasmine BlandDr. Allison BryantSusan HernandezGlorimar IrizarryDonnette McManusDr. Audra MeadowsAngela MiddletonDr. Leena MittalGinny MillerLeah RandolphDr. Jo-Anna RorieLinda SpencerACKNOWLEDGEMENTSThe Special Commission on RacialInequities in Maternal Health isgrateful to the many individualsand organizations that contributedtheir time, talents, expertise, andresources:Dr. Vanessa Nicholson, DrPH,MPH, Chief Report Editor andLead Technical WriterOlga Vanegas, Report DesignerDr. Sharma Joseph, MDStaff of Representative MarjorieDecker, Senator Jo Comerford,and Representative Liz MirandaKate Alicante, MPH, ResearchAnalyst for the Joint Committee onPublic Health and Staff Lead for theCommissionLegislative Information ServicesReproductive Equity Now, formerlyNARAL Pro ChoiceMaternal Health Working Groupled by the Boston Public HealthCommissionSPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTH03
LIST OF ACRONYMS04ASLAmerican Sign LanguageCBHCCommunity Behavioral Health CenterASD/IDDAutism Spectrum Disorder/Intellectual or Developmental DisabilityCAPTAChild Abuse Prevention and Treatment ActCARAComprehensive Addiction and Recovery ActCDCCenters for Disease Control and PreventionCNMCertified Nurse MidwifeCPMCertified Professional MidwifeL&DLabor and DeliveryMDPHMassachusetts Department of Public HealthMMMRCMaternal Mortality & Morbidity and Review CommitteeMPQCMassachusetts Perinatal Quality CollaborativeNeoQICNeonatal Quality Improvement CollaborativePELLPregnancy to Early Life Longitudinal data systemPNQINPerinatal Neonatal Quality Improvement Network of MassachusettsPOCPeople of ColorPRAMSPregnancy Risk Assessment Monitoring SystemSMMSevere Maternal MorbidityMAY 2022 REPORT
Executive SummaryCURRENT STATE OFRACIAL EQUITY INMATERNAL HEALTH INMASSACHUSETTSThe purpose of this report is to highlight the need to improve maternal health outcomes and experiencesfor the historically and currently most vulnerable residents in the state of Massachusetts, with a particularattention on racial inequities. Racial inequities are apparent on a multi-systems level and have over timeexacerbated maternal health disparities. These inequities are widening the gap between White birthing peoplecompared to Black and People of Color (POC) birthing people in the same state. Throughout the report,commission members have included findings, recommendations, and established calls to action. The callsto action prompt legislative leaders to implement and enforce these changes to optimize maternal health.Personal stories and commentary are also featured as they provide further insight into some of the challengesthat birthing people (including birthing mothers), their partners, and providers have witnessed and endured atall stages of pregnancy, including postpartum. Some have been burdened with years-long lasting effects ofthese traumatic experiences.Over a one-year period, stakeholders including elected officials, experts in the maternal health field, andcommunity members came together to discuss the current state of racial equity and inequity regarding maternalhealth in the state of Massachusetts (See Appendix A). The purpose of these meetings was to identify andunderstand the magnitude of maternal health inequity associated with structural racism and to collaborativelyestablish suggested solutions that would help inform policy initiatives. The meetings were conducted in theform of listening sessions as people and families shared their personal stories on their birthing experiences(See Appendix B). The working group structure for the commission is based on the framework of factors thatinfluence care experiences and outcomes related to health systems, community and provider factors, individualand family factors, and societal factors. The framework recognizes and asserts that the target of interventionsshould not be individuals but instead systems of care in health, public health, and communities. As the frameworkapplies to the maternal health crisis, natural workgroups emerged that included family and communityengagement, public health infrastructure, and healthcare improvement.Dr. Vanessa J. Nicholson, DrPH, MPH, Chief Report Editor and Lead Technical WriterAssistant Professor, Department of Public Health & Community MedicineTufts University School of MedicineBoston, MASPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTH05
FIGURE 1 Factors that Influence Maternal Care Experience, Outcomes, and InequitiesHealth System FactorsBirthing Individual/Family eInstitutional RacismCommunity and CareProvider Factors»»»»Knowledge, Skills & TrainingPersonal BiasCompeting DemandsInternalized andInterpersonal RacismWork and Living ConditionsHealth StatusCulture & CommunicationPreferencesSocial ResourcesInternalized RacismSocietal Factors»»»»»»Public Health and SafetyNeighborhood and PhysicalEnvironment (Housing,Transportation, CommunityContext)Economic StabilityFoodEducation & EmploymentSystemic RacismSources: 1. Byrd, WM, Clayton, LA. An American Health Dilemma.Race, Medicine, and Health Care in the United States. 1900-2000. New York: Routledge, 2002.2. Smedley, BD. Stith, AY. Nelson, AR (2003). Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care.3. Byrd WM. Clayton, LA. Racial and Ethnic health and health care disparities. Historical and contemporary issues. A Two-Part Seminar. CommonwealthFund Lecture Series. Harvard Medical School/Harvard School of Public Health. 2014.Findings were established via the use of peer-reviewed articles that include evidence-based literatureand four primary data surveillance systems: the Pregnancy Risk Assessment Monitoring System (PRAMS),the Pregnancy to Early Life Longitudinal (PELL) data system, the Maternal Mortality Review InformationApplication (MMRIA), and the Perinatal-Neonatal Quality Improvement Network of Massachusetts(PNQIN). PRAMS is an ongoing survey by most states in partnership with the CDC. The survey assessesattitudes, behaviors, and experiences before, during, and shortly after pregnancy. PRAMS collects severalstate-specific data including, but not limited to, responses to racism, maternity leave, disability status, aswell as race and ethnicity. PELL links delivery records to their corresponding hospital discharge recordsfor the delivery event for mothers and their infants, and to any non-birth-related inpatient admissions,observational stays, and emergency department visits over time, as well as death data for birthing peopleand their children. More than 99% of all deliveries in MA from 1998-2019 have been linked in PELL. The PELLlinkage allows children born to the same person to be linked together, and multiple hospitalization recordsbelonging to the same people or children to be attributed as such. MMRIA is a data system available to allMaternal Mortality and Morbidity Review Committees (MMMRC) to support essential review functions.PNQIN collects hospital specific data used for quality improvement activities among participating hospitals.PNQIN of Massachusetts is an umbrella collaborative that unites the efforts of the Neonatal QualityImprovement Collaborative (NeoQIC) and the Massachusetts Perinatal Quality Collaborative (MPQC).06MAY 2022 REPORT
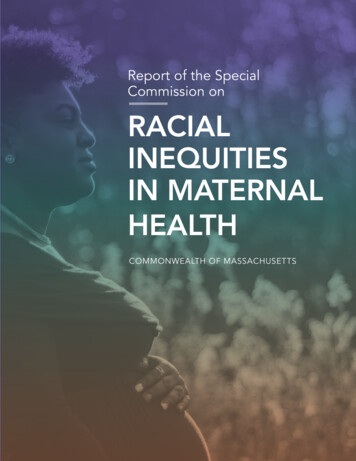
Findings and recommendations of this report conclude that efforts and enforcements towards racialequity will likely significantly improve overall maternal health outcomes for Massachusetts residents. Racialinequities are present at multiple levels (i.e. within communities, public health, and in healthcare settings);thus, the achievement in reducing SMM and maternal mortality will be dependent upon the redesigningof health delivery infrastructures and the standardization of collaboration within and across communitysettings, education, mental health assistance, housing, support of doulas and certified nurse midwives,improved competency among providers, improved access for birthing moms, and enactment of lawspertaining to maternal health delivery.The following graphic provides a context that highlights the overall maternal health disparity betweenBlack birthing persons and their peer groups as measured by the outcome of severe maternal morbidity inMassachusetts using PELL data.FIGURE 2 Severe Maternal Morbidity (Blood Transfusion not Included) among Deliveries inMassachusetts, 2009-2018HispanicWhite non-HispanicBlack non-HispanicAsianOthersSource: Massachusetts Department of HealthSevere maternal morbidity (SMM) as defined by the Centers of Disease Control (CDC)includes unexpected labor and delivery outcomes that result in significant short-or-long termconsequences to a woman’s health. Figure 1 shows that between 2009 and 2018, Black birthingpersons have experienced the highest rate of SMM compared to their peer groups. Overtime, data show that the rate at which Black people have experienced SMM compared to theirwhite counterparts has doubled, and the disparity gap has increased and widened overtime.SPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTH07
INTRODUCTIONMaternal racial health inequities in the U.S remain unsettlingly prevalent. Racism, not race, is a primarydriver of the social determinants of health. It drives inequities in housing, income, and education, especiallyamong communities of color. Racism is powerful as it acts as an underlying structural determinant that setsthe foundation for all other social determinants. Despite being a country that continuously ranks highly intechnology and innovation, the U.S. continues to rank the lowest in maternal health outcomes for birthingpersons of color. Racial disparities persist as Black birthing persons are three times more likely to die froma pregnancy-related cause than white birthing persons A range of factors contribute to these unfortunateoutcomes including variations in the quality of care, underlying chronic conditions, implicit bias, and structuralracism. Historically, many people from racial and ethnic minority groups including Black birthing personshave been prevented from having fair opportunities for economic, physical, and emotional health (Centers forDisease Control, 2022).The outcomes have gotten worse over time. For example, in 2020, 861 women were identified as having diedof maternal causes in the U.S. compared with 754 in 2019. The maternal mortality rate for 2020 was 23.8deaths per 100,000 live births compared with a rate of 20.1 in 2019 (Centers for Disease Control, 2020). In2020, the maternal mortality rate for non-Hispanic Black women was 55.3 deaths per 100,000 live births, 2.9times the rate for non-Hispanic White women (Hoyert, 2020).Since 1998, rates of pregnancy-associated mortality in Massachusetts have steadily risen (Figure1). Massachusetts is consistently among the ten healthiest states in the country, but hidden in thataccomplishment is the fact that racial and ethnic health inequities do exist and have persisted for decadesdespite efforts to improve outcomes. Data from the Massachusetts Department of Public Health (MDPH)indicate that Black non-Hispanic women are 1.9 times more likely to die during pregnancy or within oneyear postpartum compared to white non-Hispanic women. MDPH data also confirm alarming trends ofrising severe maternal morbidity (SMM), defined by the Centers for Disease Control (CDC) as unexpectedFIGURE 3 Trends in Pregnancy-Associated Mortality: Massachusetts 1998-201945PAMR (/100,000 Live Births)4035302520151050Source: Massachusetts Department of Health08MAY 2022 REPORTPAMRJoinpointAPC 1.06,p 0.24
TABLE 1Number of live births, maternal deaths, and maternal mortality rates, by race and Hispanic originand age: United States, 2018–20202018Race and Hispanicorigin and ageLive birthsMaternaldeathsNumberTotal2Under 2525–3940 and overNon-Hispanic White3Under 2525–3940 and overNon-Hispanic Black3Under 2525–3940 and overHispanicUnder 2525–3940 and 05579,5537259,696176,24317,510275,55331,104Live ve 7.65996.855.3464928.856.3263.1202718.27.719.286.0* Rate does not meet National Center for Health Statistics standards of reliability.1Maternal mortality rates are deaths per 100,000 live births.2Total includes race and origin groups not shown separately, including women of multiple races and origin not stated.3Race groups are single race.NOTES: Maternal deaths are those assigned to code numbers A34, O00–O95, and O98–O99 of the International Classification of Diseases, 10th Revision. Maternal deathsoccur while pregnant or within 42 days of being pregnant.SOURCES: National Center for Health Statistics, National Vital Statistics System, Mortality and Natality.Source: ality/2020/maternal-mortality-rates-2020.htm#Table from https://dx.doi.org/10.15620/cdc:113967outcomes of labor and delivery such as hemorrhage, blood clot, kidney failure, stroke, heart attack, and other severecomplications (Crear-Perry, 2021; Megibow, et. al 2021; Chambers, et al. 2021; Chambers, 2020). SMM is 50 to100 timesmore common than maternal death, and racial/ethnic inequalities in SMM exist: Black women have a 70% greaterrisk of SMM than their white counterparts. These racial inequities are worthy of being addressed as maternal healthinequities reflect structural and systemic fragmentation in the health care systems. Action is required at multiplelevels ,as systemic challenges call for systemic solutions, particularly at the health care systems, community, andpolicy levels.Evidence to Support ImprovementsBelow is a summary of the Commission’s key findings and recommendations in response to its charge. The findingsand recommendations correspond to three domain areas— family and community engagement, public healthinfrastructure, and healthcare systems improvement. To streamline the various focus areas, each domain wasaddressed by an assigned working group.SPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTH09
Section 1FAMILY ANDCOMMUNITYENGAGEMENTThe Family and Community Engagement working group investigated the social, structural, andcontextual factors that influence poorer maternal health outcomes for Black birthing persons andtheir families, along with strategies to counteract those factors. These strategies include developingprocesses that are inclusive of the perspectives, experiences, assets, and ideas of individuals, familiesand communities most impacted by maternal health inequities and creating partnerships withcommunities, residents, and community-based organizations. Specific areas of investigation included: 10MAY 2022 REPORTCulturally responsive and affordable doula supportTargeted support and health literacy for partnersAccessible and affordable birthing centersDiversity of healthcare providers and community health workersCultural competency of providers as it influences obstetric racismBarriers to medical and community careHistoric and current forms of racism
I. Culturally competent and affordable doulasupportA doula is a non-medical companiontrained to provide informational,emotional, and physical supportto another person and theirfamily during a significant healthexperience such as childbirth.Doulas help pregnant and birthingpeople experience care that isindividualized, safe, and equitable.Doulas can play a key role inenhancing communication betweenthe birthing person and theirmedical providers by assisting andempowering pregnant persons orthose who are giving birth to express their values and preferences, and advocatefor their needs. Doula services are also associated with decreased risk ofpostpartum depression.Previous research has demonstrated that birthing persons experience lowerrates of preterm birth and decreased risk for cesarean birth with the presenceof a doula who can provide continual emotional and relational supportthrough birth (Gruber, Cupito, Dobson, 2013). Despite this, few Black women inMassachusetts are offered or have access to their services. Studies have shownthat this type of personalized and consistent support for birthing personsimproves not only the birth experience and the physical and psychologicaloutcomes for a mother and baby, but also has a positive impact on the wellbeing of a whole family (Mather, 2021).One of the major barriers to accessing a doula is cost, as few health plans coverthe cost of doulas which can range from 800 to 2000. This makes doulasupport out of reach for many birthing people, including Black birthing personswho are the most impacted by SMM and maternal mortality (Kozhimannil,Attanasio, 2014). Boston Medical Center’s Healthy Start Program provides healthinsurance in order to improve access to early, comprehensive, and continuousprenatal care to improve the health of newborns and their mothers. The programserves only very low-income, uninsured pregnant women and does not coverdoulas. To qualify for Healthy Start, family group income must be at or below200% of the federal poverty level. For a family of four, this is equivalent to anannual income of 53,000 (Healthy Start Program, 2022). To see program impacton Black maternal mortality rates, broader eligibility would be required. TheBoston Healthy Start Initiative whose aim is to reduce racial inequities in infantmortality and poor birth outcomes has broader eligibility with no explicit incomerestrictions; however, does not offer doulas. Instead, the program offers FamilyPartners who essentially operate as community health workers, using prenatalKEY FINDINGS»»There is a lack of culturalcompetence amongcertain maternal healthprofessionalsBirthing resources suchas doula care may not beoffered or accessible toparents in need, causingstress and potential harmRECOMMENDATIONS»»»»Offer integrated culturallycompetent doula, social work,and maternal mental healthprofessionals at all stages ofthe birthing processIntegrate consultations witha doula and mental healthprofessional into prenatalvisits, especially during highrisk pregnancies Educate for birthingpersons on services andsupport provided bydoulas, midwives, mentalhealth professionals andobstetricians Ensure that all pregnant andpost-partum people enrolledin Medicaid who want accessto a doula will have one. See:Doula Medicaid Projectour healing sessions,“it Duringwas confirmed that womenof color don’t feel like they areheard after their losses and thatthis feeling of being unheardcan start way before a loss evenoccurs. Many, many mothers,especially women of color donot feel safe to advocate forthemselves during pregnancy,childbirth and beyond.”- STEPHANIE CRAWFORD,DOULA AND GRIEF SUPPORTFACILITATORSPECIAL COMMISSION ON RACIAL INEQUITIES IN MATERNAL HEALTH11
“As a doula I havesupported black motherswho have struggled tounderstand what happenedduring birth and whydecisions were made abouttheir bodies without themand are afraid that this willhappen again. And thennext pregnancy, they oftenfeel rushed to decide andtheir partners feel helplessand confused during theprocess. My job as a doulahas been to ensure thatthey know what to expect,and the outcomes thatmay arise, so that they canmake informed decisions.I also stay close during thepostpartum stage for issuesthat may come up.”– STEPHANIE CRAWFORD,DOULA AND GRIEF SUPPORTFACILITATORand well-child visits as a gateway to connect families to resources, healtheducation, care coordination and advocacy. The current limitations highlighta need for community-based doulas to collaborate with similar programs andinitiatives that extend support outside of the health centers and in chosenenvironments to birth by families (Boston Public Health Commission). States suchas Oregon and Minnesota have already expanded Medicaid to support doulaservices (Kozhimannil, Hardeman, 2016).Doula care can vary significantly depending on training and approach.Traditional structures have historically not centered the voices or experiencesof people of color or low-income communities. Community-based doulas andcommunity-based doula programs focus on cultural humility, and providingculturally appropriate, and kindred spirited non-clinical, emotional, physical, andinformational support before, during, and after birth. Furthermore, communitybased doula programs identify and train women who are trusted members of thecommunity to provide doula services at low or no cost. These programs help toimprove prenatal care, raise breastfeeding rates, decrease unnecessary medicalinterventions, increase positive birth experiences, improve parenting skills,and boost referrals for needed health services (Kozhimannil, Attanasio, 2014).The programs play a vital role in combating the discrimination, racism, and lossof autonomy that Black people who give birth frequently report experiencing(Wint, Elias, et.al. 2019). Also unique to community-based doula practice is thecollaboration with social service providers when necessary to facilitate resourcesfor transportation, housing stability, food insecurity, alcohol, tobacco, and otherdrug (ATOD) cessation, and intimate partner violence. Community-based doulasare trained to help those who are pregnant or giving birth to feel empowered toadvocate for themselves.Community-based doula training programs emphasize the historical andeducational cultural context on how race, institutional and interpersonal bias,and other social determinants play an integral role in birth disparities affectingBlack and minority populations. The support, advocacy, and continuity of carecommunity-based doulas provide may be central to reducing health disparitiesand improving maternal health equity for women of color and women from lowincome and underserved communities in Massachusetts.12MAY 2022 REPORT
II. Support & Health Literacy for PartnersIn addition to the birthing persons having the support of a doula pre-labor, labor,and postpartum, commissioners also suggest support for partners and families.The following story from Commissioner Saba and his wife Timoria McQueenSaba demonstrates how the partners of Black mothers deeply desire to supportthem, and how their inability to properly assist their partner is a burden.Although the couple has had their own unique experience, it’s important to notethat these stories highlight the necessar
Robert Saba Member of the Massachusetts COVID-19 Maternal Equity Coalition who is a maternal peer recovery coach working with women who experience high or disparate rates of maternal mortality or severe maternal morbidity Soraya DosSantos,a member of the Southcoast Massachusetts region that is an expert in maternal health and postpartum care