Transcription
ACO OVERVIEWMAKING SENSE OF THE FINALMEDICARE SHARED SAVINGS PROGRAM REGULATIONSHealthcare Financial Management AssociationSummer InstituteJuly 27, 201207/27/20121
IntroductionListJohn Redding, MD, MBAManagerBlue & Co., LLCHealthcare Consulting Practicejredding@blueandco.com(312) 504-1624John Redding, MD is a Manager at Blue Consulting Services. John brings over 15years of healthcare experience to HCS and has served as a trusted advisor toproviders and healthcare executives for the last 6 years. In his role at Blue, John workswith health systems, hospitals, and physician organizations to develop collaborativephysician-hospital working relationships and business ventures. John has extensiveexperience leading and supporting a broad spectrum of physician-hospital alignmentinitiatives, from developing and implementing physician employment strategies toproviding interim management for a Clinically Integrated Physician Network /Accountable Care Organization.2
Objectives1.Present a high level overview of the Medicare SharedSavings Program and the requirements to participate inthe Program as an ACO.2.Describe key characteristic of ACOs that will increasetheir probability of realizing an ROI from their initial andongoing ACO-related investments.3.Enable participants to evaluate the short-term and longterm fit of the ACO model for their organization andidentify alternative strategies to short-term adoption ofthe ACO model.3
ipated ImpactACO ActivityACO InsightsQuestions & Answers4
Definitions“Like unicorns. No one hasever really seen one locally,but everyone seems to knowwhat they look like.”Jim Fitzpatrick, VP MA Hospital Association5
Technical DefinitionCenter for Medicare & Medicaid ServicesMedicare Shared SavingsProgramAccountable CareOrganization“A shared savings programthat promotes accountabilityfor a patient population,coordinatesitemsandservices under Medicare PartA and B, and encouragesinvestment in infrastructureandredesignedcareprocesses for high qualityand efficient care.”“An organization of healthcare providers that agrees tobe accountable for thequality, cost, and overall careof Medicare beneficiaries whoare enrolled in the traditionalfee-for-service program whoare assigned to it.”*Center for Medicare and Medicaid Services.6
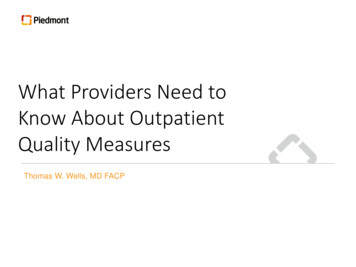
Practical DefinitionMedicare Shared Savings ProgramFor practical purposes, the Medicare Shared Savings Program(MSSP) can be considered a hybrid shared savings / pay forperformance incentive modelForecastEstimated savingsX50% – 60% shareActual(max 10% - 15% forecast expenditures)XOrganizational quality score Annual shared savings distribution to ACOY (-3)Y (-2)(Y-1)Y0Y1Y2Y37
Eligibility8
EligibilityFormationACOs can be formed by one or moreof the following participants:1.2.3.4.5.6.7.ACO professionals in group practicearrangementsNetworks of individual practices of ents between hospitals andACO professionalsHospitals employing ACO professionalsCAHs that bill under Method IIRHCsFQHCsLegal entity under State, Federal orTribal lawMay not participate in a duplicativeshared savings program9
EligibilityParticipationMust include enough primary careprofessionals to cover at least 5,000Medicare beneficiariesACO participants upon whombeneficiary assignment is determinedmust be exclusive to one ACOMust provide list of TINs & NIPsMust notify when adding or removingACO providers or suppliers within 30daysMust describe how shared savings willbe distributed10
EligibilityGovernance75% ACOParticipantsMust maintain an identifiablegoverning body with the authority toexecute the functions of the ACOHas the following responsibilities:Provide oversight & direction 1 old ACO management accountable andDefines processes for evidence-basedmedicine, quality & cost reporting, andcoordinating care.Governing bodies governing processmust be transparentMust have a conflict of interests policy11
EligibilityLeadershipLeadership & management structureGoverningBodyOrganizational chartsCommittee lists with names of committeemembersJob descriptionsExecutiveLeadDocuments effectuating formationCharters, urance &Improvement?Articles of incorporationPartnership, joint venture, management, orasset purchase agreementsParticipants’ and ACO providers /suppliers’ rights and obligationsParticipation agreementsEmployment contracts?Operating policies12
EligibilityPromotion Of Evidence-Based MedicineMust describe how it will establish andmaintain ongoing quality assurance &improvement effortsMust provide documentationdescribing its plans to:Promote evidence-based medicinePromote beneficiary engagementReport on quality and costs andCoordinate careMust document its plans to:Ensure provider / supplier complianceRemediate non-compliant partiesAssess and continuously improve cost &quality performance13
Options14
OptionsStart DatesThree options for participation:1.April 1, 2012Term of Agreement is 3 years and 9 monthsFirst period 21 months2.July 1, 2012Term of agreement is 3 years and 6 monthsFirst period 18 months3.January 1, 2013 and beyondTerm of agreement is 3 yearsFirst period is 12 months15
OptionsTracksTrack 1(One-Sided Model)Shared savings only (no risk)Maximum of 50% share or 10% ofbenchmark performanceMinimum savings rate based on asliding scale determined by thenumber of beneficiariesNo shared lossesFirst dollar savings if minimumthresholds are metTrack 2(Two-Sided Model)Shared savings & losses (risk)Maximum of 60% share or 15% ofbenchmark performanceMinimum savings rate set at a flat2%Shared loss potential set at 1 minusthe calculated shared savings rateMinimum loss rate set at a flat 2%Loss sharing limit increases overthe 3 year term (5%, 7.5%, 10%)First dollar savings and losses ifminimum thresholds are met16
Operations17
OperationsBeneficiary AssignmentBeneficiaries enrolled under Medicare fee-forservice parts A & BPreliminary attributionRetrospective assignmentStepwise process1.2.3.Plurality of primary care services from ACO affiliatedPCPPrimary care services provided by other ACOaffiliated professionals (specialists, NPs, Pas, etc.)Retrospective assignmentPrimary care services defined byHCPCP codesFQHC & RHC revenue center codes18
OperationsExpense BenchmarksBased on Medicare Part A & BexpendituresCalculation based on 3-month run-outof claims with a completion factorBenchmark years weights:BY3: 60%BY2: 30%BY1: 10%Adjustments made for:Newly assigned beneficiariesChanges in health status (CMSHCC risk score)19
OperationsQuality & Reporting Standards33 measures in four domainsPatient / caregiver experience2. Care coordination / patient safety3. Preventative health4. At-risk population1.Pay-for-performanceyears 2 & 3phasedinoverMultiple reporting methodologies5 step process to calculate score1.2.3.4.5.Determine points earned for each measureSum the total points for all measures ineach domainDivide the total points earned in eachdomain by the total available points in eachdomainMultiply each domain by the 25% weightSum all weighted domain scores20
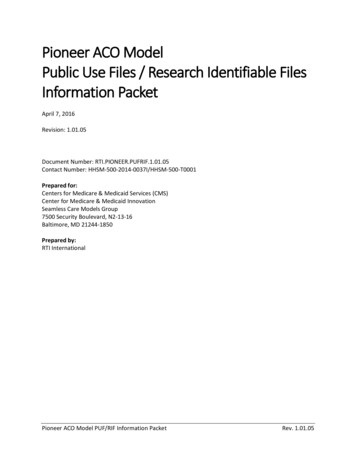
OperationsShared Savings CalculationEstimated savingsX50% – 60% share(max 10% - 15% forecast expenditures)XOrganizational quality score Annual shared savings distribution to ACO21
OperationsMarketing & NotificationMarketingmaterialsdefinedasmaterials, “used to educate, solicit,notify, or contact Medicare beneficiariesor providers and suppliers regarding theShared Savings programMay use marketing materials 5 daysafter filing them with the CMS andcertifying that they comply with allrequirementsMust notify beneficiaries of participationat point-of-careMust post signs at their facilitiesMust make standardized written noticesavailable22
Coordination With Other AgenciesFederal Trade Commission & The US Departmentof JusticeGuidance applies to all ACOsNo mandatory anti-trust reviewVoluntary expedited review (90 days)CMS to share application & dataSafe harbor for ACOs with less than 30% market sharein their PSA or under the rural exception“Will vigilantly monitor complaints about ACO formationor conduct and take whatever enforcement action maybe appropriate.”Internal Revenue Service (for comment)ACOs engaged exclusively in the MSSP would stillqualify for tax exempt status under 501(3)(c)Participation in the MSSP through an ACO will furtherthe charitable purposes of the tax exempt organizationThe tax exempt organization does not have to havecontrol over the ACOOffice of the Inspector General (for comment)Do not want to unduly limit impede development ofbeneficial ACOsApplies to Physician Self-Referral Law, Federal AntiKickback Statute, and the Civil Monetary Penalties LawFive proposed waivers1.ACO Pre-Participation Waiver2.ACO Participation Waiver3.Shared Savings Distribution Waiver4.Compliance with Physician Self-Referral Law5.Patient Incentive WaiverCenter for Medicare & Medicaid InnovationAdvanced Payment ACO ModelStart up capital for physician-only ACOs and rural ACOsUp to 50 ACOs ( 170 M in funding)Must indicate interest in CMS filingRecipients selected based on formulaIn general, will not consider participation inurement orimpermissible private benefit23
Anticipated Impact24
ACO’s Estimated ImpactCenter for Medicare & Medicaid ServicesParticipants50 to 270 ACOsFederal Savings 470MBonus Payments 1.31BStart Up Costs 29M to 157MOperating Costs 63M to 342M25
ACO’s Estimated ImpactCongressional Budget OfficeReviews the outcomes of 10 majordemonstrationsIn nearly every care coordinationprogramspendingwaseitherunchanged or increasedFor value-based payments only,bundled payments showed significantsavingsKey Takeaways1.The ACO model remains unproven2.Physician & patients must be engagedin care management efforts3.Incentive payment design matters26*Lessons Learned from Medicare’s Demonstration Projects on Disease Management, Care Coordination, and Value-Based Payment. January, 2012.
ACO Activity27
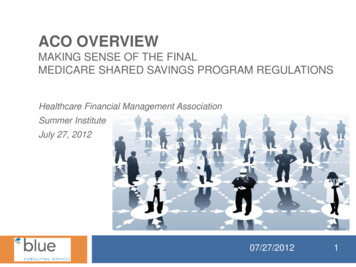
Types Of ACOsGovernmentalPioneer ACOsMedicareShared SavingsProgramCommercialProviderSponsored ACOsPayer SponsoredACOsProvider-PayerSponsored ACOs28
Pioneer ACOsJanuary 1, 2012 Organizations with experience offering coordinated, patient-centered care, and operating in ACO-likearrangements First two performance years, shared savings and shared losses payment arrangement with higher levels ofreward and risk than in the Shared Savings Program Third performance year, those Pioneer ACOs that have shown savings over the first two years will beeligible to move to a population-based payment model (per-beneficiary per month payment amount)intended to replace some or all of the fee-for-service (FFS) payments with a prospective monthly payment1.Allina Health11.Genesys Alliance22.Partners Healthcare2.Atrius Hospitals12.Healthcare Partners Medical Group23.Physician Health Partners3.Banner Health Network13.Healthcare Partners of Nevada24.Plus!4.Beacon, LLC14.Heritage California ACO25.Presbyterian Healthcare Services5.Bellin Thedacare HealthcarePartners15.JSA Medical Group26.Primecare Medical Network16.Michigan Pioneer ACO27.Renaissance Health Network17.Monarch Healthcare28.Seton Health Alliance18.Montefiore ACO29.Sharp Healthcare System19.Mount Auburn CambridgeIndependent Practice Association30.Steward Healthcare System31.Trinity Pioneer ACO, LC20.OSF Healthcare System32.University of Michigan21.Park Nicollet Health Services6.Beth Israel Deaconess PhysicianOrganization7.Brown & Toland Physicians8.Dartmouth-Hitchcock ACO9.Fairview Health System10.Franciscan Alliance29
Medicare Shared Savings Program ACOsApril 1, 20121.Accountable Care Coalition of Caldwell County,LLC13.Chinese Community Accountable CareOrganization2.Accountable Care Coalition of Coastal Georgia,LLC14.Catholic Medical Partners15.Costal Carolina Quality Care, Inc.16.Crystal Run Healthcare ACO, LLC17.Florida Physicians Trust, LLC18.Hackensack Physician-Hospital Alliance ACO, LLC3.Accountable Care Coalition of Eastern NorthCarolina, LLC4.Accountable Care Coalition of Greater AthensGeorgia, LLC5.Accountable Care Coalition of Mount Kisco, LLC19.Jackson Purchase Medical Associates, PSC6.Accountable Care Coalition of SoutheastWisconsin, LLC20.Jordon Community ACO21.North Country ACO22.Optimus Healthcare Partners, LLC23.Physicians of Cape Cod ACO, Inc.24.Premier ACO Physician Network25.Primary Partners, LLC7.Accountable Care Coalition of Texas, Inc.8.Accountable Care Coalition of the Mississippi GulfCoast, LLC9.Accountable Care Coalition of the North Country,LLC10.AHS ACO, LLC26.RVG ACO Health Providers, LLC11.AppleCare Medical ACO, LLC27.West Florida ACO, LLC12.Arizona Connected Care, LLC30
Medicare Shared Savings Program ACOsJuly1, 20121.Arizona Health Advantage, Inc.23.Advocate Health Partners2.John C Lincoln Accountable Care Organization, LLC24.Chicago Health System ACO, LLC3.Fort Smith Physicians Alliance ACO, LLC25.Deaconess Care Integration, LLC4.ApolloMed Accountable Care Organization Inc.26.Franciscan AHN ACO, LLC5.Golden Life Healthcare LLC27.Indiana University Health ACO, Inc.6.John Muir Physicians Network28.Genesis Accountable Care Organization, LLC7.Meridian Holdings, Inc.29.Iowa Health Accountable Care, L.C.8.North Coast Medical ACO, Inc.30.One Care LLC9.Torrance Memorial Integrated Physicians, LLC31.University of Iowa Affiliated Health Providers, LC10.MPS ACO Physicians, LLC32.Owensboro ACO11.PriMed, LLC33.Quality Independent Physicians12.Accountable Care Coalition of Northwest Florida, LLC34.Southern Kentucky Health Care Alliance13.Accountable Care Partners, LLC35.TP-ACO LLC14.Allcare Options, LLC36.Central Maine ACO15.Florida Medical Clinic ACO, LLC37.Maine Community Accountable Care Organization, LLC16.FPG Healthcare, LLC38.MaineHealth Accountable Care Organization17.HealthNet, LLC39.Accountable Care Organization of Maryland, LLC18.Integrated Care Alliance, LLC40.Greater Baltimore Health Alliance Physicians, LLC19.Medical Practitioners for Affordable Care, LLC41.Maryland Accountable Care Organization of Eastern Shore LLC20.Palm Beach Accountable Care Organization, LLC42.Maryland Accountable Care Organization of Western MD LLC21.Reliance Healthcare Management Solutions, LLC43.Circle health Alliance, LLC22.Wellstar Health Network, LLC44.Harbor Medical Associates, PC31
Medicare Shared Savings Program ACOsJuly1, 2012 Continued 45.Accountable Healthcare Alliance, PC68.Summa Accountable Care Organization46.Oakwood Accountable Care Organization, LLC69.University Hospitals Coordinated Care47.Southern Michigan Accountable Care, Inc.70.North Bend Medical Center, Inc.48.Essential Health71.Coastal Medical, Inc.49.Medical Mall Services of Mississippi72.Accountable Care Coalition of The Tri-Counties, LLC50.BJH Healthcare ACO, LLC73.AnewCare LLC51.Heartland Regional Medical Center74.Cumberland Center for Healthcare Innovation, LLC52.Nevada Primary Care Network ACO, LLC75.MissionPoint Health Partners53.Concord Elliot ACO LLC76.St. Thomas Medical Group, PLLC54.Barnabas Health ACO-North, LLC77.Summit Health Solutions55.Accountable Care Coalition of Syracuse, LLC78.BHS Accountable Care, LLC56.Asian American Accountable Care Organization79.Memorial Hermann Accountable Care Organization57.Balance Accountable Care Network80.Methodist Patient Centered ACO58.Beacon Health Partners, LLP81.Essential Care Partners, LLC59.Chautauqua Region Associated Medical Partners, LLC82.Physicians ACO, LLC60.Healthcare Provider ACO, Inc.83.Texoma ACO LLC61.Mount Sinai Care, LLC84.Central Utah Clinic, P.C.62.ProHEALTH Accountable Care Medical Group, PLLC85.Accountable Care Coalition of Green Mountains, LLC63.WESTMED Medical Group, PC86.Polyclinic Management Services Company64.Cornerstone Health Care, PA87.Aurora Accountable Care Organization, LLC65.Triad Healthcare Network, LLC88.66.Mercy Health Select, LLCDean Clinic and St. Mary’s Hospital Accountable CareOrganization89.ProHealth Solutions, LLC67.ProMedica Physician Group, Inc.32
ACO Development TrendsFive Trends InACO Development1.The number & types ofACOs are expanding2.Growth is centered inlarger populationcenters3.Hospitals continue to nethe largest backers ofACOs, but physiciangroups are playing aincreasingly larger role4.Non-Medicare ACOsare experimenting withmore diverse modelsthat Medicare backedACOs5.The success of anyparticular ACO model isstill undetermined*David Muhlenstein et al., Growth and Dispersion of Accountable Care Organizations June 2012 Update, White Paper, (Leavitt Partners, June 2011).33
ACO Insights34
Likely Characteristics Of Successful ACOs3 Most Essential Elementsof a Successful ACO*3 Other Essential Elementsof a Successful ACOA deep understanding& vigilant managementof costsRobust care / diseasemanagementSophisticated clinicalanalyticsPractice-orientedoperational redesignAn elegantmethodology forsharing savingsCulture of continuouslearning*Bob Spoerl., “3 Most Essential Elements of a Successful ACO”, Becker’s Hospital Review, June 13, 2012.35
Likely ACO EvolutionShort-TermMid-TermLong-Term(1st Contractual Period)(2nd Contractual Period)( 3rd Contractual Period)Waste Reduction & InpatientOperational ExcellenceAppropriateness-Of-Care &Physician Practice RedesignDisease Management &Population HealthLength of dable admissionsGaps-in-careReferral patternsSite-of-careTransitions in careDisease avoidanceDisease progressionDisease specific PMPM costsPatient engagement / complianceRisk stratified outcomes36
The ACO ModelViable For Some And Likely To Impact ManyThe CMS & HHS have made significant modifications to theirproposed regulations to increase the value proposition of theMSSP to hospitals and health systemsHospitals & health systems that dismissed the ACO model basedon the proposed regulations would be wise to reconsider theopportunity provided by the program under the final regulationsAlthough the MSSP will not be universally attractive, it is likely toimpact a number of local and regional healthcare marketsHospital leaders should evaluate and begin planning for thepotential impact of ACOs in their marketsWhether or not participation in the MSSP is right for yourorganization at this time, “business as usual” will not be asustainable long-term strategy37
Questions & Answers38
Trinity Pioneer ACO, LC 32. University of Michigan Organizations with experience offering coordinated, patient-centered care, and operating in ACO-like arrangements First two performance years, shared savings and shared losses payment arrangement with higher levels of reward and risk than in the Shared Savings Program