Transcription
Presenting a live 90‐minute webinar with interactive Q&ANew Pioneer ACO Model Program:LLetteroff IIntent DDue JuneJ10Evaluating Whether to Participate in CMS' Alternative Shared Savings Program*** Letter of intent due by June 10, complete application by July 18 ***THURSDAY, JUNE 2, 20111pm Eastern 12pm Central 11am Mountain 10am PacificT d ’ facultyToday’sfl features:fDavid A. Manko, Partner, Rivkin Radler, Uniondale, N.Y.George Choriatis, Partner, Rivkin Radler, Uniondale, N.Y.The audio portion of the conference may be accessed via the telephone or by using your computer'sspeakers. Please refer to the instructions emailed to registrants for additional information. If youhave any questions, please contact Customer Service at 1-800-926-7926 ext. 10.
Conference MaterialsIf you have not printed the conference materials for this program, pleasecomplete the following steps: Click on the sign next to “Conference Materials” in the middle of the lefthand column on your screen.screen Click on the tab labeled “Handouts” that appears, and there you will see aPDF of the slides for today's program. Double click on the PDF and a separate page will open. Print the slides by clicking on the printer icon.
Continuing Education CreditsFOR LIVE EVENT ONLYFor CLE purposes, please let us know how many people are listening at yourlocation by completing each of the following steps: Close the notification box In the chat box, type (1) your company name and (2) the number ofattendees at your location Click the blue icon beside the box to send
Tips for Optimal QualitySSoundd QualityQ litIf you are listening via your computer speakers, please note that the quality ofyour sound will vary depending on the speed and quality of your internetconnection.If the sound quality is not satisfactory and you are listening via your computerspeakers, you may listen via the phone: dial 1-866-871-8924 and enter your PINwhen promptedprompted. OtherwiseOtherwise, please send us a chat or e-maile mailsound@straffordpub.com immediately so we can address the problem.If you dialed in and have any difficulties during the call, press *0 for assistance.Viewing QualityTo maximize your screen, press the F11 key on your keyboard. To exit full screen,press the F11 key again.again
New Pioneer ACO Model Program:gLetter of Intent due June 10George Choriatis, Esq.George.Choriatis@rivkin.comDavid A. Manko, Esq.David.Manko@rivkin.comJune 2, 20112011 RivkinRadler LLP. Privileged & Confidential 2011 Rivkin Radler LLP. Privileged& Confidential5
Agenda1Introduction to the Pioneer ACO Program/Placing it in context2In‐‐Depth Analysis of the Pioneer ACO programIn 2011 Rivkin Radler LLP. Privileged & Confidential6
The Pioneer ACO ProgramH CausedHasCdQQuitei a SStiri ini theh IndustryI d“The Pioneer Program is a faster pathfor mature ACOs,” CMSSSource: JJenny GGold,ld “Ad“Administrationi ii OffOffers NNew PPathh ffor ACOACOs,”” KKaiseri HHealthl hNNews,May 17, 2011 2011 Rivkin Radler LLP. Privileged & Confidential7
Dr. Berwick Succinctly ExpressesWh iit’sWhat’ All AbAbout “The [MSSP] proposed rule will bea core model. It will be whatanybody can play with. But we allknow there are places out therethat are ready to surge ahead to acompletely different level ofintegration. They’ve been therealready or are en route. Wouldn’tit be nice if we had made a spacepfor a vanguard, who can moveahead of the pack and teach us allthe way to go? Maybe theInnovation Center can be a homefor that kind of pioneeringelement on our behalf, oneveryone’s behalf. Not speciallyentitled pplayers,y , but our scouts.” 2011 Rivkin Radler LLP. Privileged & ConfidentialDr. Donald M. Berwick, Administratorof CMS, in a speech at the BrookingsInstitution on February 1, 2011,quoted in Douglas Hastings,Hastings “PioneerACOs: Surging to a New Level ofIntegration?” Health Affairs Blog, May25, 2011, http://healthaffairs.org/blog8
The Journey From the Affordable CareA to theActh ACO PioneerPiProgramPPatient Protection and AffordabilityyAct and Health Care and EducationReconciliation Act of 2010(“Affordable Care Act” or “PPACA”)enacted on March 23,23 2010 2011 Rivkin Radler LLP. Privileged & ConfidentialPPACA pput in placepnumerouspayment and delivery system reforms: Required CMS to establish theMedicare Shared Savings Program(MSSP) to support and promoteaccountable care organizations(ACOs) Required CMS to establish Centerfor Medicare and MedicaidInnovation ((“Innovation Center”)) Contained other complimentaryreforms, including medical homes,bundled payments, value‐basedpurchasing,h i etc.t9
Pioneer ACO Program is part of a broader set ofpaymentt andd deliveryd lisystemtreformsfoff PPACAPayment and delivery system reforms entails changingthe way providers are paid in order to incentivizethem to change the way they deliver care in a mannerth t improvesthatitheth valuel off suchh care, i.e.,i ththeeffectiveness and efficiency of such care.Reform ofPaymentMethodologies(Replace Today’sFee for Servicewith Outcomes‐based Payments)causes 2011 Rivkin Radler LLP. Privileged & ConfidentialRestructuring ofDelivery System(From Today’sFragmented CareSystems toCoordinated CareSystems, i.e. ACOs)yieldsImprovement inValue of HealthServices(Better healthoutcomes per dollarspent; Reduction ingrowth rate ofhealth spending)10
The MSSP: Medicare’sCCoreIInitiativei i i forf AdAdvancingi ACOACOs MSSP is not a pilot program, but it is part of Medicare Under MSSP, eligible providers who join together asan ACO to coordinate care and assume accountabilityfor a defined population of Medicare patients willshare in the savings the ACO achieves for Medicarewith respect to the total (Part A and Part B)expenditures of its defined patient population.population On March 31, 2011, CMS issued a proposed rule (the“MSSP Proposed Rule”) for implementing the MSSP Final rule is to be issued later this year Under PPACA, CMS must have the MSSP up andrunning not later than January 1, 2012 2011 Rivkin Radler LLP. Privileged & Confidential11
The Innovation Center as Testing Groundf MforMore EffEffectivei AlAlternativesito MSSP Innovation Center was established by CMS inNovember, 2010 Purpose is to develop and test innovative paymentand delivery system models designed to encouragecoordinated care in Medicare, Medicaid, and CHIP Expected to developdevelop, among other thingsthings, a series ofACO pilot projects to test alternatives to the MSSP Has authority to expand successful models, includingby implementing them on a nationwide basis 10 billion appropriated for 2011‐2019 2011 Rivkin Radler LLP. Privileged & Confidential12
What is thePiPioneerACO Program?P? The Pioneer ACO program is the first ACO pilot programdeveloped by the Innovation Center It is intended to support “vanguard” organizations in thetransformationa so a o oof theire busbusinessess modelode too thee ACOO modelode byentering into ACO arrangements with Medicare and otherpurchasers (including Medicaid and commercial payors) so as toderive the majority of their revenues from ACO arrangements One purpose of the Pioneer ACO program is to inform potentialfuture changes to the MSSP Upp to 30 organizationsgwill be selected to participateppin thePioneer Program. ACOs may participate in either the MSSP or the Pioneerprogram,pg, but not both concurrently.y 2011 Rivkin Radler LLP. Privileged & Confidential13
Why Consider Pioneer Model? Certain entities ineligible to form their own ACO under MSSPmay do so under the Pioneer program (i.e. FQHCs) Pioneer program differs in many respects from MSSP, includingon patientopa e assignmentass g e anda d paymentpay e arrangements,a a ge e s, whichc mayaybe more advantageous to certain ACOs CMS will provide to Pioneer ACOs various forms of technicalassistance,, including:g– assistance in developing ACO arrangements with stateMedicaid agencies– Provision of monthly,monthly quarterly,quarterly and annual patient datareports on assigned patient population Engagement of Pioneer ACOs in shared learning activities 2011 Rivkin Radler LLP. Privileged & Confidential14
Upcoming Dates and DeadlinesJune 7,, 2011CMS will host a specialpopenp door forumon the Pioneer programJune 10,, 2011Letters of Intent (LOI) due Not binding on ACO (used by CMS forplanning purposes only) In order to be considered, an applicantmust submit to CMS an LOI by its duedate Templates for LOI are available at theInnovation Center websiteJuly 18, 2011Full application is due Applications available on InnovationCenter website 2011 Rivkin Radler LLP. Privileged & Confidential15
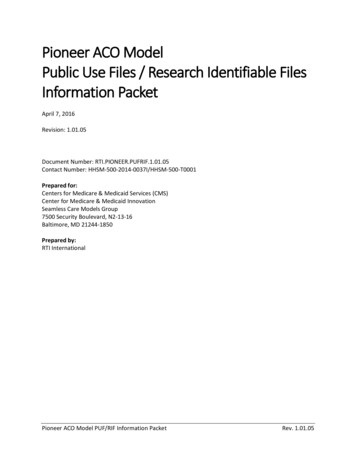
Pioneer ACO TimelineMarch2010March 23,2010PPACAenacted Nov2010 Jan2011CMSestablishedInnovationCenterApril2011May uly2011June10,,2011LetterofIntentDueOct2011July 18,2011FullApplicationDue Jan2012Start Date forPioneer ACO(sometime inthe 3rd or 4thquarter)PioneerMSSPMarch 31- CMSissues proposedregulations forMSSP 2011 Rivkin Radler LLP. Privileged & ConfidentialCMS to issue finalregulations forMSSP (sometimein 3rd or 4thquarter)StartDate forMSSP16
Relation between Pioneer Program andtheh MSSP PProposeddRRule/l / FiFinall RuleR l The MSSP regulationsgare onlyy proposedp prules,, and are subjectjto change when the final rule is issued later this year– MSSP will be governed by the final rule in all respects The Pioneer program incorporates many elements of the MSSPregulations– Elements incorporated from MSSP relating to eligibility willbe those set forth in the MSSP proposed rule, regardless ofchanges in the MSSP final rule– Other elements incorporated from MSSP will be those setforth in the final rule After acceptance into the Pioneer program,program a Pioneer ACO maywithdraw, if it finds unacceptable any conditions in the MSSPfinal rule– Withdrawal deadline is Januaryy 1,, 2012 2011 Rivkin Radler LLP. Privileged & Confidential17
Agenda1Introduction to the Pioneer ACO Program/Placing it in context2In‐‐Depth Analysis of the Pioneer ACO programIn 2011 Rivkin Radler LLP. Privileged & Confidential18
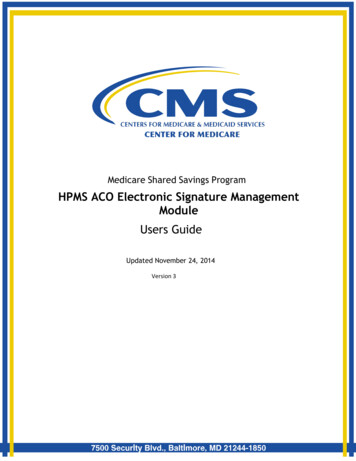
The Three Basic Elements of an ACO willSServeas OOur RRoadmapd Let s cover the Pioneer ACO program in a stepwise fashion, byLet’sfocusing on each of the three basic elements of the ACOconcept, in turn. An ACO is:1. A ggroupoup cocomprisedp sed oof providersp o de s fromo differentd e e institutionals u o asettings and specialties across the continuum of care, which2. Serves a defined patient population; and3 Assumes accountability for the quality and total costs of care of3.the defined patient population across the entire continuum ofcare:– By contracting for outcomeoutcome‐basedbased payments that reward/penalize its participating providers based on successes inimproving health outcomes per dollar spent for the definedpopulation.pp 2011 Rivkin Radler LLP. Privileged & Confidential19
Diagram of an ACOandd its ThreehBasic ElementslAccountableCareOrganizationPrimary ts forOutcome‐Basedd PaymentsHealthPlanAncillaryHealth CareProvidersProvide Coordinated CareDefinedPatient Population 2011 Rivkin Radler LLP. Privileged & Confidential20
Focusing First OnOrganizationall MattersAccountableCareOrganizationPrimary ts forOutcome‐Basedd PaymentsHealthPlanAncillaryHealth CareProvidersProvide Coordinated CareDefinedPatient Population 2011 Rivkin Radler LLP. Privileged & Confidential21
Which Entities are Eligible to be an ACO?(Ph i i G(PhysicianGroup PPracticesiNNetworks)k) In both the Pioneer program and the MSSPMSSP, thefollowing are eligible to serve as ACO:– ACO professionals in group practice arrangements– Networks of individual practices of ACOprofessionals In both programs,programs “ACO Professional” meansphysician, physician assistant, nurse practitioner, andclinical nurse specialist 2011 Rivkin Radler LLP. Privileged & Confidential22
Which Entities are Eligible to be an ACO?(E i i IInvolving(Entitiesl i HHospitals)i l)MSSPEligible EntitiesPioneer ProgramEligible EntitiesKey Differences inDefinition of HospitalMSSPPartnerships or joint Same as SSP, exceptventures betweenthat definition ofhospitals and ACO“hospital” is broaderprofessionalsp“Hospital” definedto mean an acutecare hospital subjectto inpatientpprospectiveHospitals employing Same as SSP, except payment systemACO professionalsthat definition of(IPPS) (consistent“hospital” is broader with PPACArequirements) 2011 Rivkin Radler LLP. Privileged & ConfidentialPioneer Program“Hospital” definedto include not onlyacute care hospitalssubjectj to IPPS butalso certain non‐IPPS hospitals,including cancerhospitals,p, children’shospitals, and CAHs23
Which Entities are Eligible to be an ACO?(C i i l A(CriticalAccess HHospitalsi l (CAHs))(CAH )) Medicare provides two payment methods for outpatient CAHs:– Standard Method (Soc. Sec. Act 1834(g)(1)): CAH bills afacility fee and claims for professional services areseparatelysepaa e y billedb ed by anda d paidpa d too thee renderinge de g physicianp ys c a– Method II (Soc. Sec. Act 1834(g)(2)): CAH bills for both thefacility fee and the professional services fee CAHCAH’ss that bill under the Standard Method are ineligible toparticipate in the MSSP because CMS concluded that they lackthe requisite data elements necessary for patient assignment CAHCAH’ss that bill under Method II are eligible to participate in theMSSP (and form their own ACO) because CMS concluded thatthey have the requisite data elements necessary for patientassignmentg 2011 Rivkin Radler LLP. Privileged & Confidential24
Which Entities are Eligible to be an ACO?(FQHC and(FQHCsd RHCs)RHC ) In MSSP pproposedprule,, CMS asserts that Federallyy QualifiedHealth Center (FQHC) and Rural Health Center (RHC) claims andpayment systems lack requisite data elements necessary forpatient assignment, so their patient population cannot beassigned to the ACO:– Patient population is assigned based on utilization of primarycare services furnished by a physician– Requisite data elements for assignment are (i) specificservice rendered (i.e. primary care HCPCS codes), (ii) type ofpractitioner (i.e. physician as opposed to PA or NP), and (iii)specialty of practitioner (i.e. primary care)– FQHC/ RHC claims systems distinguish general classes ofservices by revenue code, but do not have HCPCS codes thatidentify the specific service rendered and contain onlylimited information on the practitioner rendering the service 2011 Rivkin Radler LLP. Privileged & Confidential25
Eligibility of FQHCs/ RHCsto ParticipateP i iiin MSSP In MSSP,, FQHCs// RHCs cannot form their own,, independentpACO– Since CMS is unable to assign the FQHC/RHC patientpopulation to the ACO, an ACO formed by an FQHC/ RHCwould have no patient population assigned to it In MSSP, FQHCs/ RHCs may join an ACO formed by eligibleproviders– But even in this case, the FQHC/ RHC patient population willnot be assigned to the ACO– Nonetheless, the ACO has certain financial incentives toinclude FQHCs/ RHCs (to be discussed later on) In MSSP proposed rulerule, CMS indicated that it will seek to testways for collecting requisite data from FQHCs/ RHCs and atsome future date may allow FHQCs/ RHCs to fully participate inthe MSSP 2011 Rivkin Radler LLP. Privileged & Confidential26
Eligibility of FQHCsto ParticipateP i iiin PiPioneer ProgramP In Pioneer program,program CMS would negotiate with theFHQC methods for patient assignment, expenditurebaseline, and expenditure benchmark calculations In Pioneer program, FQHCs may form own ACOs orjoin ACO formed by others 2011 Rivkin Radler LLP. Privileged & Confidential27
Which Entities are Eligible to be an ACO?(O h providers(Otherid andd suppliers)li ) Other Medicare providers and supplies (includingambulatory surgery centers, skilled nursing facilities,long term care hospitals, etc.) are not eligible to forman ACO on their own Nonetheless, these other providers/ suppliers mayjoin an ACO formed by eligible providers and serve asan “ACOACO ParticipantParticipant” in such ACO– Their patients will not be assigned to the ACObased on their claims data– But they may be otherwise equivalent to otherACO participants, including with respect togovernance, distribution of shared savings, etc. 2011 Rivkin Radler LLP. Privileged & Confidential28
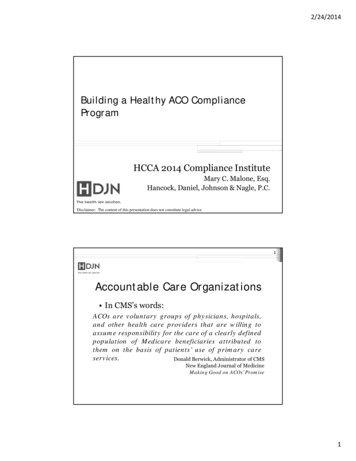
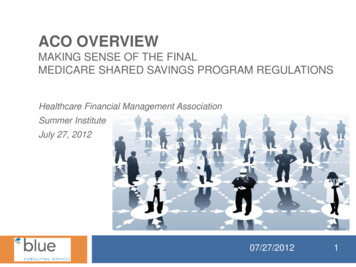
Pioneer ACO Selection Criteria Pioneer ACO applicationto be reviewed by a panelof experts fromDepartment of Healthand Human Services andother organizations Reviewed applicationswill be scored, based oncriteria set forth in thePioneer Program Requestf ApplicationforVulnerablepPopulations(5 points)Potential forproducing three‐part aim(20 points)Leadership andManagement Capabilities(20 points)Performance Capabilities/HIT infrastructure(20 points)PatientCenterednessCapabilities(10 points)Experience with Financial Risk‐Sharing(25 points)Summary of Selection Criteria and Scoring 2011 Rivkin Radler LLP. Privileged & Confidential29
Must Providers be Exclusive to an ACO?In both the MSSP and the Pioneer Program: An ACO Participant upon which patient assignment is dependentmust be exclusive to the ACO– Primary care physicians must be exclusives since,since asdiscussed later, assignment is dependent upon them– Primary care physician means Internal medicine General practice Family practice Geriatric medicine An ACO Participant upon which patient assignment is notdependent need not be exclusive to the ACO 2011 Rivkin Radler LLP. Privileged & Confidential30
Legal Structure Requirements In both the Pioneer Program and the MSSP: ACO must be a legal entity with its own taxidentification number (TIN) ACO may be structured as any type of entitypermitted under state law (i.e. corporation, limitedliability companycompany, partnership,partnership etc.)etc ) A pre‐existing legal entity need not form a new entityif it otherwise meets all ACO eligibility requirements ACO need not be Medicare‐enrolled (although eachACO participant must be Medicare‐enrolled) 2011 Rivkin Radler LLP. Privileged & Confidential31
Governance Requirements – ACO MustHHaveMMechanismh i ffor ShShareddGGovernanceMSSP Governance RequirementsPioneer Governance RequirementsGOVERNING BOARD(i.e. Board of Directors) 75% controlled by ACO participantsEach ACO participant Eachto have proportionate control Must include a patient representative CMS stated that PioneerACO governancerequirements are “similar”to those under MSSP,although it did not set forthspecific requirements Exception:– Governing Board mustalso include a consumeradvocate (in addition tothe patientrepresentative)QUALITY ASSURANCE/PROCESS IMPROVE‐MENT IVEDIRECTOROFFICER(B d C tifi earrangements may be vkinRadlerLLP.PrivilegedConfidentialacceptable, provided they have requisite capabilities32
Additional Requirements Internal Processes Requirements – Use and promotion of evidence‐basedmedicine– Patient engagement– Reportingpg on qualityqy and costmeasures– Promoting coordination of carePatient‐Centeredness Requirements– Patient experience of care surveyprocess– Patient involvement in governance– Process for evaluation of populationhealth needs and consideration ofdiversity– Process and systems for identificationof high risk individuals, individualizedcare plans for target populations, andintegration of community resources 2011 Rivkin Radler LLP. Privileged & ConfidentialPatient Centeredness (Cont.)– Processes for coordinationof care, including healthinformation exchange– Processes forcommunicating clinicalknowledge/ evidence‐based medicine withpatients– WrittenW itt standardst d d forfpatient access andcommunication, includingaccess to patient records– Processes for measuringclinical performance andusing the results to improvecare and service over time33
EHR Meaningful Use Requirements In both MSSP and Pioneer Program: As a condition to continued participation in theprogram, at least 50% of ACO’s primary carephysicians must be meaningful EHR users (as definedin the HITECH Act) by start of second year, in MSSP,and byy end of 2012,, in the Pioneer pprogramg In addition, the percentage of primary care physicianswho are meaningful EHR users will be reflected in theACO’ qualityACO’sli score (to( bbe didiscussedd laterlon)) 2011 Rivkin Radler LLP. Privileged & Confidential34
Focusing OnTheh Patient PopulationlAccountableCareOrganizationPrimary ts forOutcome‐Basedd PaymentsHealthPlanAncillaryHealth CareProvidersProvide Coordinated CareDefinedPatient Population 2011 Rivkin Radler LLP. Privileged & Confidential35
Patients’ Freedom of Choice of Provideri RisRetainedi d iin BBothhPPrograms An ACO is “assigned”assigned a patient population “Assignment” refers only to an operational processundertaken by CMS to attribute patients to an ACO;patient does not enroll in an ACO There are no restrictions on a patient’s freedom tochoose providers outside of ACO With respect to the above items, there are nodifferences between the Shared Savings and thePioneer programs 2011 Rivkin Radler LLP. Privileged & Confidential36
Composition and Numberoff AAssignedid PatientP iPPopulationl iMSSPPioneer ProgramType of PatientMedicare FFS beneficiariesMinimum Numberof PatientsAt least 5,000 Medicare FFSAt least 15,000 Medicare FFSbeneficiaries must be assigned beneficiaries must be assignedto the ACOto the ACOException: For rural ACO(whose majority of cliniciansare locatedl t d iin rurall areas),) ththeminimum is 5,000Consequences ofassigned patientpopulation fallingbelow the minimumnumber during theparticipation term(i) ACO given a warning andSameplaced on a correction plan; (ii)If the number of assignedpatients does not return to theminimum floor, thenparticipation will beterminated 2011 Rivkin Radler LLP. Privileged & ConfidentialSame37
Patient Assignment:Th BTheBasici CConcepts Under both programs,programs patient population is assignedon annual basis for each performance year – i.e.assigned patient population is redefined annually andmay differdiff fromfyear tto year. Under both programs, patients are to be assigned toan ACO based on their utilization of pprimaryy careservices provided by the ACO, although the specificmethodology differs 2011 Rivkin Radler LLP. Privileged & Confidential38
Patient Assignment:Th BTheBasici CConcepts Timing of the assignment:– Prospective assignment: Patients assigned at the beginningof each performance period, based on utilization datademonstratingdeo s a gpprovisiono so oof primaryp a y careca e servicesse ces too patientspa e sprior to the performance period– Retrospective assignment: Patients assigned at the end ofeach pperformance pperiod,, based on utilization datademonstrating provision of primary care services to patientsduring the performance period There are differences amongg the programsp gwith respectp totiming of assignment 2011 Rivkin Radler LLP. Privileged & Confidential39
Patient AssignmentU d theUnderh MSSP At the end of each performanceyear, the ACO is assigned on aretrospective basis those MedicareFFS beneficiaries who received– the plurality of their primarycare services (as determined bythe charges for the services,not their frequency or otherfactor)– from primary care physicianswho are ACO Participants ofthat ACO– during that performance year 2011 Rivkin Radler LLP. Privileged & Confidential Primary care PhysiciansInternal medicineGeneral practiceFamily practiceGeriatric medicinePrimary care Services(Identified by HCPC Code)99201 to 9921599304 to 9934099341 to 99350G0402 (Welcome toMedicare visits)G0438, G0439 (annualwellness visits)40
The “Expected” Assigned PopulationU d theUnderh MSSP At the beginning of each performance year andcontinuing periodically thereafter, CMS will provide tothe ACO certain data on the “expected” assignedpopulationl ti off theth ACO “Expected” assigned population is intended as a proxyfor that which could ppotentiallyy be assignedgto theACO at the end of the performance period Expected assigned population is comprised ofhihistoricallyi ll assignedi dbbeneficiariesfi i i andd may differdiff ffromthe patient population that is actually assigned at theend of the performance period 2011 Rivkin Radler LLP. Privileged & Confidential41
Patient AssignmentU d theUnderh PiPioneer ProgramP Pioneer ACO may elect either– Retrospective assignment (which would be nearlyidentical to the MSSP assignment process); or– Prospective assignment Patient assignment for FQHCs/ RHCs 2011 Rivkin Radler LLP. Privileged & Confidential42
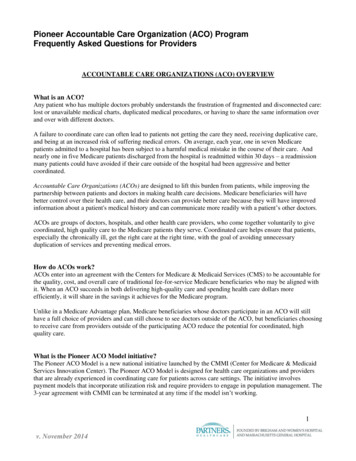
Prospective AssignmentU d theUnderh PiPioneer ProgramPPioneer ACO Start %weighting CMS will analyze claims data of ACO participants for the threeprior years (with the most recent year weighted most (as shownabove) to identify patients who received the plurality of theirprimary care services (as determined by the charges) during thatthree year period (as weighted) from providers who are ACOParticipants of that ACO CMS will engage in a two‐step process, as discussed in thefollowing slide 2011 Rivkin Radler LLP. Privileged & Confidential43
The Two‐Step Process for ProspectiveA iAssignmentUnderU d theh PioneerPiProgramP Step 1: CMS will first identifythose patients who received theplurality of their primary careservices from primary careproviders who are ACOparticipants of that ACO Step 2: For patients who had10% or less of their evaluationand management allowedcharges billed by PCPs, CMS willidentifyf the group off eligiblespecialist physicians who billedthe plurality of E&M allowedcharges for that patient.patient 2011 Rivkin Radler LLP. Privileged & ConfidentialUnder Step 1, “Primary CareProvider” has same meaning as“primary care physician” in MSSP,except that it includes nursepractitioners and physician assistants)Under Step 2, “eligible specialists” are: Nephrology Neurology Oncology Pulmonology Rheumatologygy Cardiologygy Endocrinology44
Assignment by Certification Available forPiPioneerACOACOs withi hPProspectivei AssignmentA i Pioneer ACOs who have selected prospective assignment mayhave patients assigned to it by certification (i.e. an affirmativeattestation by the patient rather than claims‐based algorithms)– Intente iss too allowa o patientspa e s anda d providersp o de s too aligna g based onomutually acknowledged care relationships Patients who newly enroll in Medicare or disenroll from aMedicare Advantageg pplan,, althoughg these will not be included inthe financial calculations of the ACO until after having accrued12 months of FFS experience Patients who alreadyy have 12 months of FFS experiencepmayyattest at anytime, but will not be included in the ACO’s financialcalculations until the subsequent performance period 2011 Rivkin Radler LLP. Privileged & Confidential45
End‐of‐Period Modifications to thePProspectivelyi l AAssignedidPPopulationl i Pioneer ACOs that select prospective assignment will beaccountable for all their prospectively assigned patients at theend of the performance year, with certain exceptions: Exceptions:cep o s– Patients who have any months of Medicare Advantageenrollment or enrollment in only Part A or only Part B at anypoint duringg the ppperformance yyear– Patients who transfer their Medicare address to a CoreBased Statistical Area or rural county that is not adjacent tothat the of ACO’s location– Patients who receive more than 50% of their evaluation andmanagement allowed charges in non‐adjacent CBSAs or ruralcounties duringg the performanceppperiod 2011 Rivkin Radler LLP. Privileged & Confidential46
Focusing In On AccountabilityAccountableCareOrganizationPrimary ts forOutcome‐Basedd PaymentsHealthPlanAncillaryHealth CareProvidersProvide Coordinated CareDefinedPatient Population 2011 Rivkin Radler LLP. Privileged & Confidential47
Participation Agreementandd itsi TermTMSSPPiPioneerPProgramAgreement ACO must enter into a participation SameRequirement agreement with CMSCommence‐Cment ofTermJJanuary 1 followingf ll i approvall offapplication, with first start date tobe January 1, 2012 (possibly asecond start date of July 1, 2012)3 d off 4th3rd4 h quarter off 2011Length ofTerm 3 years ACO performance periods areannual, for a total of 3 annualperformance periods in the term Minimum of 3 performance periods(slightly longer than 3 years due toearly start date), with two one‐yearoptional extensions (for a total ofapproximately five years) 2011 Rivkin Radler LLP. Privileged & Confidential48
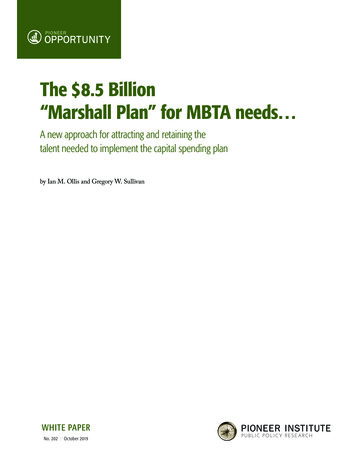
How Are an ACO and its ParticipantsPaid?id? Theh ThreehBasici Modelsd lVolume-Based/Less RiskOne‐Sided Shared Savings ACO participantscontinue to receivepayments under theMedicare FFS programunder Part A and PartB in the same manneras otherwise be made In addition, ACO isentitled to a portion ofsavingsiachievedhi d ifspending is less thanbudget targets,provided certainquality standards aremet 2011 Rivkin Radler LLP. Privileged & ConfidentialOutcome-Based/More RiskTwo‐Sided Shared Savings Same as oneone‐sidedsidedshared savings model,except that:i.ACO also is accountablefor losses to the extentactual spendingexceeds budget targetsii.Percentage of sharedsavings payable to theACO is greater thanunder the one‐sidedmodel Partial CapitationACO participantscontinue to receive FFS,but at lower ratesACO also receives aprospective, capitatedpayment equal to theremainder of the ACO’sFFS projected revenue.Some models alsocontain bonuses/penalties based onachievement of budgettargets and qualitymeasuresmeasures.49
The Full Continuum ofOOutcome‐BasedB d PaymentsPVol
the pioneer aco program is the first aco pilot program developed by the innovation center it is intended to support "vanguard" organizations in the traaso aonsformation of their busbus essiness model to the aco model by entering into aco arrangements with medicare and other purchasers (including medicaid and commercial payors) so as to