Transcription
HHC ACO INC.ANNUAL SOLE MEMBER MEETINGDecember 16, 2021At 1:00 p.m.Held via teleconference/videoconferenceNew York CityAGENDACALL TO ORDEROLD BUSINESS1. Approve and adopt minutes of the HHC ACO Inc. (“ACO”) Membership meeting heldon January 28, 2021 (Exhibit A)NEW BUSINESS2. RESOLUTION Authorizing that each of the following persons be elected, effectiveimmediately, to serve as a Director of HHC ACO Inc. (“ACO”) Board of Directorsin accordance with the laws of the State of New York, until such person’ssuccessor is duly elected and qualified, subject to such person’s earlier death,resignation, removal, or termination of his or her employment with any entity thathas executed an ACO Participation Agreement or ACO Agreement3. REPORT by ACO Chief Executive Officer Matthew Siegler on the ACO’s PY 2020Performance Results and PY 2021 Expenditure Projection4. REPORT by ACO Chief Medical Officer David Stevens, M.D. on the ACO's ClinicalActivitiesADJOURNMENT
EXHIBIT A
NEW YORK CITY HEALTH AND HOSPITALS CORPORATION ACCOUNTABLE CAREORGANIZATION SOLE MEMBER ANNUAL MEETINGA meeting of HHC ACO, Inc. Sole Member Annual Meeting of New YorkCity Health and Hospitals Corporation was held viateleconference/videoconference on the 28th day of January, 2021, pursuantto a notice which was sent to all of the Directors of New York CityHealth and Hospitals Corporation and which was provided to the public bythe Secretary. The following Directors participated r.Ms.Ms.Mr.Ms.Ms.Mr.Ms.José PagánMitchell KatzVincent CalamiaDave ChokshiPhillip WadleScott French – left at 4:11Helen Arteaga Landaverde – joined at 4:16Barbara LoweRobert NolanSally Hernandez-PiñeroFreda WangFeniosky Peña-MoraAnita Kawatra – joined at 2:13Mr. Pagán, Chair of New York City Health Hospitals Board,called the meeting to order at 4:04 p.m. Mr. Pagán chaired themeeting and Ms. Colicia Hercules, Corporate Secretary, kept theminutes thereof.Mr. Pagán notified the Board and the public that Scott Frenchwould be representing Steven Banks and Phillip Wadle would berepresenting Deputy Mayor Melanie Hartzog for this portion of themeeting, both in a voting capacity.ADOPTION OF MINUTESThe minutes of the meeting of the HHC ACO Sole Member meetingheld on December 19, 2019, were presented to the Board. On motionmade and duly seconded, the Board unanimously adopted the minutesRESOLVED, that the minutes of the meeting of the HHC ACO SoleMember meeting held on December 19, 2019, copies of which havebeen presented to the Board, be and hereby are adopted.
Mr. Pagán then turned the meeting over to Matthew Siegler, ChiefExecutive Officer of HHC ACO, Inc. to present the next items on theagenda.Mr. Siegler read the resolution into the record:Authorizing that each of the following persons be elected,effective immediately, to serve as a Director of HHC ACO Inc.(the “ACO”) Board of Directors in accordance with the laws of theState of New York:Name:Mitchell Katz, M.D.Matthew Siegler, Esq.John Ulberg, Jr. M.P.H.Andrea Cohen, Esq.Gary Kalkut, M.D.Nicole Jordan-Martin, M.P.A.Jasmin Moshirpur, M.D.Luis Marcos, M.D.Warren Seigler, M.D.Lori Donnell, M.B.A.Hyacinth PeartGroup Represented:NYC Health HospitalsNYC Health HospitalsNYC Health HospitalsNYC Health HospitalsNYC Health Hospitals, NYUPhysicians representative atBellevue, Cumberland andWoodhullNYC Health HospitalsMt. Sinai Elmhurst FacultyPracticePhysician Affiliate Group of NewYork, P.C.Coney Island Medical PracticePlan, P.C., Harlem MedicalAssociated, P.C. andMetropolitan Medical PracticePlan, P.C.Non-Affiliated Participants(Community Healthcare Networkand University Physicians ofBrooklyn)Medicare BeneficiaryUpon motion made and duly seconded, the Board unanimouslyapproved the resolution.Mr. Siegler provided an update of the ACO activities during thepast year. He advised that Dr. David Stevens is now the new ChiefMedical Officer for the ACO. He highlighted the performance paymentsfor 2019, the MSSP contract renewal, quality performance metrics, anexpenditure comparison of the ACO to regional and national benchmarks,the ACO’s evolving role with partnerships and engagements, and theACO’s clinical model for high-risk patients.
OLD BUSINESS/NEW BUSINESS - ADJOURNMENTAfter discussion - hearing of no old business or new business ton; nua;eti n g, the meetingt-I c. SoleA :7 : d : d3:: nColicia Hercules NYC Health Hospitals Corporate Secretary
RESOLUTION
RESOLUTION OF NEW YORK CITYHEALTH AND HOSPITALS CORPORATION (the “CORPORATION”)Authorizing that each of the following persons be elected, effective immediately, to serveas a Director of HHC ACO Inc. (the “ACO”) Board of Directors in accordance with the lawsof the State of New York, until such person’s successor is duly elected and qualified, subjectto such person’s earlier death, resignation, removal, or termination of his or her employmentwith any entity that has executed an ACO Participation Agreement or ACO Agreement:Mitchell Katz, M.D.;Matthew Siegler, Esq.;John Ulberg, Jr., M.P.H.;Andrea Cohen, Esq.;Nicole Jordan-Martin, M.P.A.;Hyacinth Peart, a Medicare beneficiary Director;A Director who shall be the Chief Executive Officer of Physician Affiliate Group ofNew York, P.C. (“PAGNY”);A Director to be named by NYC Health Hospitals to represent physicians employedby New York University School of Medicine and providing services in NYC Health Hospitals facilities, as specified in a writing by NYC Health Hospitals that isdelivered to the Chairman of the ACO;A Director to be named by the Icahn School of Medicine at Mount Sinai, doingbusiness as Mt Sinai Elmhurst Faculty Practice (the “Elmhurst FPP”), as specified ina writing by the Elmhurst FPP that is delivered to the Chairman of the ACO;A Director to be named pursuant to a designation by a majority in number of thePresidents of Coney Island Medical Practice Plan, P.C., Downtown Bronx MedicalAssociates, P.C., Harlem Medical Associates, P.C., and Metropolitan MedicalPractice Plan, P.C. (the “PAGNY FPPs”), as specified in a writing by such majoritythat is delivered to the Chairman of the ACO; andA Director to be named pursuant to a joint designation by Community HealthcareNetwork, Inc., and University Physicians of Brooklyn, Inc., (the “Non-AffiliateParticipants”) as specified in a writing by such Non-Affiliate Participants that isdelivered to the Chairman of the ACO.
WHEREAS, the ACO was established as a subsidiary to NYC Health Hospitals, and theACO’s By-Laws designate NYC Health Hospitals as the Sole Member of the ACO; andWHEREAS, the ACO’s By-Laws state that Directors of the ACO shall be elected annuallyby the Member.NOW, THEREFORE, BE ITRESOLVED, that the Member hereby authorizes that each of the following persons beelected, effective immediately except as noted below, to serve as a Director of the ACO Board ofDirectors in accordance with the laws of the State of New York, until such person’s successor isduly elected and qualified, subject to such person’s earlier death, resignation, removal, ortermination of his or her employment with any entity that has executed an ACO ParticipationAgreement or ACO Agreement:Mitchell Katz, M.D.;Matthew Siegler, Esq.;John Ulberg, Jr., M.P.H.;Andrea Cohen, Esq.;Nicole Jordan-Martin, M.P.A.;Hyacinth Peart, a Medicare beneficiary Director;A Director who shall be the Chief Executive Officer of Physician Affiliate Group of NewYork, P.C. (“PAGNY”);A Director to be named by NYC Health Hospitals to represent physicians employed byNew York University School of Medicine and providing services in NYC Health Hospitals facilities, as specified in a writing by NYC Health Hospitals that is deliveredto the Chairman of the ACO;A Director to be named by the Icahn School of Medicine at Mount Sinai, doing businessas Mt Sinai Elmhurst Faculty Practice (the “Elmhurst FPP”), as specified in a writing bythe Elmhurst FPP that is delivered to the Chairman of the ACO;A Director to be named pursuant to a designation by a majority in number of the Presidentsof Coney Island Medical Practice Plan, P.C., Downtown Bronx Medical Associates, P.C.,Harlem Medical Associates, P.C., and Metropolitan Medical Practice Plan, P.C. (the“PAGNY FPPs”), as specified in a writing by such majority that is delivered to theChairman of the ACO; and
A Director to be named pursuant to a joint designation by Community Healthcare Network,Inc., and University Physicians of Brooklyn, Inc., (the “Non-Affiliate Participants”) asspecified in a writing by such Non-Affiliate Participants that is delivered to the Chairmanof the ACO.
NYC Health HospitalsAccountable Care OrganizationAnnual Sole Member MeetingDecember 16, 2021Matthew Siegler.CEO of HHC ACO Inc.David Stevens, MDCMO of HHC ACO Inc.
Agenda Approve and Adopt Meeting Minutes HHC ACO Inc. Board of Directors Resolution PY 2020 Performance Results PY 2021 Expenditure Projection Benchmark Calculation and Risk Score Clinical Activities ACO High-Utilizer Pathway Annual Wellness Visit Plan for 20222
HHC ACO Inc. Board of DirectorsResolutionAuthorizing that each of the following persons be elected, effectiveimmediately, to serve as a Director of HHC ACO Inc. (the “ACO”) Board ofDirectors in accordance with the laws of the State of New York.NAMEGROUP REPRESENTEDMitchell Katz, M.D.NYC Health HospitalsMatthew Siegler, Esq.NYC Health HospitalsJohn Ulberg, Jr., M.P.H.NYC Health HospitalsAndrea Cohen, Esq.NYC Health HospitalsGary Kalkut, M.D.NYC Health Hospitals, recommended by NYU to represent their employedphysicians at Bellevue, Cumberland, and WoodhullNicole Jordan-Martin, M.P.A.NYC Health HospitalsJasmin Moshirpur, M.D.Mt. Sinai Elmhurst Faculty PracticeRichard Becker, M.D.Physician Affiliate Group of New York, P.C.Warren Seigel, M.D.Coney Island Medical Practice Plan, P.C., Downtown Bronx Medical AssociatesP.C., Harlem Medical Associates, P.C., and Metropolitan Medical Practice Plan, P.C.Daniel Napolitano, M.D.Non-Affiliated Participants (Community Healthcare Network and UniversityPhysicians of Brooklyn)Hyacinth PeartMedicare Beneficiary
PY 2020 Performance Results- 8 Consecutive Years of Success Performance Results for the Current Contract:PY 2019Savings to Medicare ( )Quality Score (%)Earned Performance Payment ( )PY nce from past contracts available in the AppendixCOVID Utilization and Related Policy Changes had Major Impact COVID expenditures excluded from shared savings calculation Initial Quality Scores were adjusted in accordance with a CMS policy PY 2019 Initial: 87%; PY 2020 Initial: 93%Total Savings and Earned Performance Payment (2013-2020): Total Savings to Medicare: 67,312,191 Total Earned Performance Payment: 35,109,866PY 2020 provider distributions will be largest in history of ACO ACO planning 2.7m deferred distribution fund for PY20214
PY 2020 Quality PerformanceDomain2019 Domain 2020 DomainScoreScore*Patient/Caregiver Experience*84.00%100.00%Care Coordination/Patient Safety*75.25%96.25%Preventive Health95.00%90.00%At-Risk Population92.50%87.50%Full set ofmetrics availablein the Appendix*CMS Extreme and Uncontrollable Circumstances Policy In effect for the entire PY 2020 CMS gave ACOs full credit for the following quality domain/metrics:o CAHPSo All Condition Readmissionso Admissions for Patients with Multiple Chronic Conditions5
PY 2021 Expenditure ProjectionsProjections based on CMS data from Jan-Sept 2021 indicate that theACO will not be able to earn shared savings but will not owe money to CMS Projected Savings/losses: - 82 per beneficiary Projected Threshold to earn Shared Savings: 411 per beneficiarySavings 0- 411Shared Losses Range(ACO pays CMS)PY 2021Projected 411Shared Savings Range(CMS pays ACO)Minimum Savings/Losses RangeNo Payment Made6
2021 Challenges Driven by PostCOVID Patient Acuity and ACOProgram Design Issues HHC ACO continues to spend less than regional and national averages,deliver high quality care with lower hospital admissions.Reducing expenditure per beneficiary and/or CMS relaxing the cap onrisk adjustment may be critical to earn future shared savings.Rate of ChangeCompared to 2018 (Baseline)Number of Hospital Admissions per 1,000Average Cost of Hospital AdmissionOverall Risk ScoreACO Expenditure per BeneficiaryRegional Expenditure per BeneficiaryNational Expenditure per BeneficiaryPer Patient Exp.(COVID Excluded)*Weighted average based on ourACO’s population proportion201920202021 Q3201920202021 %1.4%-24.7%44.2%TBD11.2%7.4%5.5%HHC ACO 12,127 10,714 13,164Regional* 17,193 16,350 17,885National* 16,142 15,670 15,7097
Drivers of ACO Shared SavingsKey ACO program design features present challenges to H H: ACO benchmark pre-dates H H EPIC conversion and revenue cycle improvements Risk adjustment capped at 3% per year These factors are not as relevant in our Managed Care Value Based Payment contracts40% Increase in CMI at H Hbetween 2018 and 2021Changes inCMS-HCCRisk ScoresAccounts for changes inseverity and case mix forthe attributed patientsbetween 2018 and 2021*Increase Capped at ditureBaseline expenditurecalculated using datafrom 2016 to 2018 (fixed)Medicare FFSGrowth RatesAccounts forchanges inMedicarereimbursementpolicies andrates between2018 and 20218
Concerns from ACOs: Risk Adjustmentand Benchmark CalculationCapping any increase in the risk adjustment at 3 percent does not account for risk score growth inthe ACO’s regional service area and is not well suited for systems with major IT and revenue cycleenhancements like H H Problematic for ACOs in regions with beneficiaries whose risk scores rise more than 3 percent May be penalizing ACOs with complex beneficiaries where the cap may be inadequate to accountfor changes in beneficiaries’ disease burden over timeCurrent risk adjustment methodology may not adequately adjust for changes in health statusamong continuously assigned beneficiaries between the benchmark and performance years;specifically it may not adequately account for issues facing HHC ACO patients such as: Socioeconomic factors Frailty and functional status Chronic conditions requiring ongoing careCMS recognizes that the current approach may be inadequate and may not account for theaforementioned factors; however CMS argues that: Having no cap or higher cap would provide insufficient protection against efforts to increasecoding intensity 3 percent cap represents a reasonable balance between recognizing potential differences inhealth status for ACO assigned beneficiaries between years while protecting the Medicare TrustFunds against excessive coding9
Clinical ActivitiesUpdates by David Stevens, MDACO Chief Medical Officer
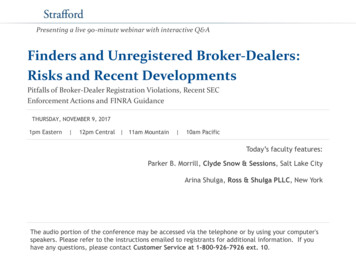
Highest Priority PatientsWhat we know:1. A very small number ofpatients account fordisproportionately high costTop 2%Per PatientProj. Costfor PY 2021 120,00098% 11,0002. ACO Patients who have been admitted twice in a year have aVERY high rate of additional admissions within the year Based on Past Data, Risk of 3rd Admission: 41.5% 2021: 200 patients with 2 or more admissions11
ACO High-Utilizer PathwayCare ModelPC TeamPCP-RN-CHWPatientClinicalPartnersUrgent Access:Virtual ExpressCareSocial Support: Home Care SW, NYLAG, etc.Home Nursing:H H Home CareTransportation:ACO PilotLonger-term Care Coordination:TBD12
ACO Highest-Utilizer PathwayHypothesis:Patients with 2 or more admissions in a given year are 50% likelyto have repeat admissions.Can we identify and address barriers to optimal care?CO ACOidentifieshighest-riskpatientsHome Care Skilled nursing care Social Work evaluation Address social supports Family/caregiver issues Rehab (PT/OT) at home Self management teaching Safety Evaluation Virtual ExpressCare infoOutreach andassessment forunmet c Health Corps (PHC) Assess address barriers to goals Social supports/SDOH Care Coordination Support with self-management Collaborate with PC Team 90 day enrollment13
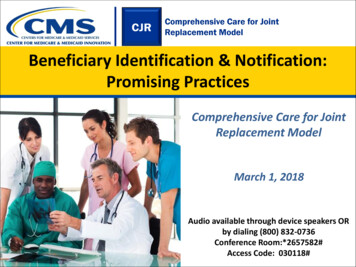
ACO High-Utilizer PathwayBarriers Breakdown107 PatientsFully ressUnaddressed12061 (47.8%)42 (37.2%)17 (15.0%)191715148445557422720ADLsMedication SelfManagementTransportation# of Barriers Unaddressed0Disconnected fromDifficultyWound Care NeedH H Outpatient Care Obtaining/AffordingMedications# of Barriers In-Progress# of Barriers Addressed14
ACO High-Utilizer Pathway24 Hour Contacts All H H ACO High-Utilizerpatients received this flyer H H Home Care nursesgive it to ACO patientsduring their home visits Public Health Corps CHWstrained to give thesephone numbers15
ACO High-Utilizer PathwayTransportation Needs PC Teams identified Transportation as a key barrier to care Plan: Provide free car service for high-priority ACO patientswith transportation challenges ACO-funded and coordinated Facility teams identify appropriate patients Established vendor (Sentry) used16
Annual Wellness VisitMedicare-defined benefit that reimbursesComprehensive Geriatric Risk managementReason for Action: Address health risks early (12 functional screens)Close quality gaps (falls screening, etc.)Support capturing CRG scores (‘Dependent for ADLs’, etc.)Engages non-provider staff to deliver more value efficientlyStatus: Implemented at 7 facility Geriatrics practicesPlan: Implement across adult primary care in 202217
Annual Wellness VisitEpic Express Lane – Screen and NotesIntakeScreeningsCompleted byRN PCAClick on any Risk thatscreened positive tobring up order set andadd diagnosesScreenings andPlanspulled into note18
Plan for 2022Annual Wellness Visit:a. Expand to Adult Primary Care H H wideHigh-Priority Patient Work: continue to:a. Support Facility ACO teams, CHW involvementb. Develop Clinical Partnerships ( VEC, HC, others)Innovations being explored:a. Model for extended social support/coordinationb. Start-up support for Home Based Primary Carec. Alternatives to Subacute Rehabd. Integrate with system-wide care transitions worke. Strengthening partnership with Behavioral Health19
Have a safe and wonderfulholiday season!20
Appendix21
PY 2020 Quality PerformanceDomainDomainDomainMeasure #Score 2019 Score 2020Patient/Caregiver84.00%Experience (CAHPS)Care Coordination/Patient SafetyPreventive Health95.00%96.25%90.00%ACO-3892.50%87.50%Risk Standardized, All Condition Readmissions *, †All-Cause Unplanned Admissions for Patients with MCCs *, †ACO-13Ambulatory Sensitive Condition Acute Composite †Falls Risk ScreenACO-14Influenza ImmunizationACO-17ACO-18Tobacco Screen f/uDepression Screen f/uACO-19Colorectal ScreenACO-20Breast CA ScreenStatin for CVDACO-43ACO-42At Risk PopulationH H ACO2020All 9972.87CMS waived the CAHPS requirement for PY 2020 andassigned automatic full credit for the entire domain100.00%ACO-875.25%Measure NameH H ACO2019ACO-27Diabetes: Hemoglobin A1c Poor Control ( 9%) †ACO-40Depression RemissionHTN controlACO-28*CMS assigned automatic full credit for measure due to PHE† Lower rate means better performance‡ Extreme and uncontrollable circumstances policy was in affect for entirePY 2020. Accordingly, CMS awarded SSP ACO's the higher of the meanquality score across all ACOs or the ACO's own quality score in PY 2020Significant ImprovementSignificant DeclineNo Significant ChangeFinalInitialACO Overall ACO OverallQuality Score Quality Score2019202092.17% ‡96.87% ‡86.69%93.44%22
Performance ResultsAll Contract YearsPY 2013Assigned BeneficiariesPY 201412,369PY 201513,294PY 2016PY 2017PY 201812,24110,04210,29310,5697,122,016 13,118,3023,592,1665,276,9737,262,050Total Savings ( )7,428,094Quality Score ,644,6056,052,3641,586,8592,182,3602,967,275Earned Performance Payment ( )PY 2019(Jan - Jun)Assigned BeneficiariesPY 2019(Jul-Dec)PY 202011,0269,0929,268Total Savings ( )3,343,8014,456,17115,712,618Quality Score 00Earned Performance Payment ( )Total(2013-2020)67,312,19135,109,8664,621,33723
has executed an ACO Participation Agreement or ACO Agreement 3. REPORT by ACO Chief Executive Officer Matthew Siegler on the ACO's PY 2020 Performance Results and PY 2021 Expenditure Projection 4. REPORT by ACO Chief Medical Officer David Stevens, M.D. on the ACO's Clinical Activities. ADJOURNMENT