Transcription
Montreal Children’s Hospital – McGill University Health CenterEmergency Department Fracture GuidelineDisclaimersThis document is designed to assist physicians working in our emergency department in caring for children (under 18 years ofage) with traumatic injuries. The recommendations contained within this guideline do not preclude the need for a completeand thorough patient assessment, or indicate an exclusive course of action. Variations taking individual patient circumstancesinto account may be appropriate. All open fracture or those with neurovascular impairment require urgent management inconsultation with the appropriate surgical specialty. This guideline pertains to closed fractures only.Who to call for clinical adviceFor Health Care Professionals requiring additional assistance or advice, please call the on-call orthopaedic or plastics servicefor immediate advice at 514-412-4400 ext 53333; they are available 24/7/365.For doctors outside of the MCH who have diagnosed a fracture, refer patients:DIRECTLY to the OUT-PATIENT Orthopedic or Plastic Surgery Clinic- NON-DISPLACED AND IMMOBILIZED INJURIES (ex. temporary slab, wrist guard)- Referral can be submitted (directly by patient) via the website: https://www.thechildren.com/request-appointmentTo the EMERGENCY ROOM- DISPLACED FRACTURES AND / OR UNABLE TO TEMPORARILY IMMOBILIZE- Send patient with a consult (legible name and license) and any imaging already done*** Please note we do not have a cast technician at night between 11pm-8am ***Specifications on organizing follow-up- If there is (potential) significant swelling, a 3-way slab should be utilized for immobilization- For orthopaedic and plastics follow-up, please enter the following on the consult form:Age, Sex, Side, Bone, Location, Fracture Type, Cast-Type (ex. 8-year-old girl, Right distal radius fracture, below elbow molded cast)- If closed reduction done, please indicate (ex. Left D5 Boxer’s Fracture, post-reduction, Ulnar gutter cast)- If PRN f/u indicated, please indicate in chart and provide patient/family phone number to clinic (514-412-4040)- FYI: Ortho has physiotherapist in their clinic, Plastics has access to occupational therapy during clinicImmobilization ConsiderationIf immobilized with follow-up within 1 week, this guideline suggests SLABS over definitive immobilizationMaterials*** NEW Standard of Care Child proof casts : 3M sleeve, Wet/Dry soft roll, and Fiberglass cast ****** Water proof casts : may be offered to patients whose follow up is at 3 weeks and is most appropriate for below large jointcasts (examples: below elbow cast fingers in safe).Molded cast- When molding is required, the ideal material is plaster of Paris.Hand injuries- SAFE position is defined as wrist extension at 20 degrees, metacarpophalangeal (MCP) joint at 70 degreesflexion and the inter-phalangeal (IP) joints in full extension.- If follow-up within 1 week, then use gutter or slab. Otherwise use full cast to immobilize in safe position.- Injuries requiring single digits to be immobilized may be done so with aluminium splints or “buddy taping”.Any questionsPlease direct comments or suggestions to Dr Sasha Dubrovsky at sasha.dubrovsky@mcgill.caAcknowledgement and ApprovalsDubrovsky, Bretholz, Benaroch, Saran, Cugno, Friedman, Kudirka, Frechette, and Eliane Cote (family partner)Special acknowledgements: Drs. Brody and Diksic for their contributions to previous edition, Dr. Diksic for editorial assistance on this version, and to all members ofthe ED’s CASTED (casts and splints in the emergency department) LEAN QI project team.Approved by MCH Divisions of Emergency, Orthopedic, Plastic Surgery, and Trauma, July 1, 2018.
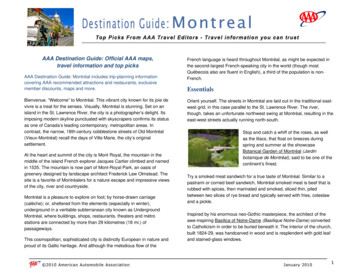
ED Fracture Guideline 2018UPPER EXTREMITYConsult ORTHOPAEDICS for follow-upAbbreviations:Above elbow A/EWrist Guard W/GDistal third of bone DISTALAge definitions:YOUNG 10 or 12FractureRadius&/orUlnaDetailsIndication toreduceBuckle, SH-1 undisplacedBelow elbow B/ESalter-Harris Classification SHOLDER 10 or 12ImmobilizationtypeW/GFollow upguidelinesNo sports 4-6 weeksIf YOUNG, PRN f/u if anyconcerns 6 weeksIf OLDER, 4 weeksYOUNG, W/G 4 weeksOLDER, B/E 1 weekSH-2 undisplacedB/E MoldedSH-1,2 displacedSH- 3,4,5Reduce in EDCALL ORTHOPEDICSDISTAL undisplacedor DISTAL “minimally” displaced(greenstick or transverse)- “minimally” defined as:YOUNG 10 degreesOLDER 5 degreesDISTAL displaced(greenstick or transverse)NB: if more than “minimally” displaced & not needingreduction, ensure well molded cast with plaster of ParisReduce in ED if:Age 6 20 degreesYOUNG 15 degreesOLDER 5 degreesPlastic deformity (clinically visible)Reduce in EDHead displacedB/E Molded1 weekA/E1 weekA/E1 week1 weekYOUNG, A/EOLDER, SlingHead undisplacedA/ECALL ORTHOPEDICS1 week(consider A/Emolded 5yrs)CALL ORTHOPEDICSRadial neck buckle1 week1 weekW/G(if concern, treat asDISTAL displaced)Shaft(s) undisplacedShaft(s) displaced(consider A/Emolded 5yrs) 3 weeks 1 week3 weeks1 week2
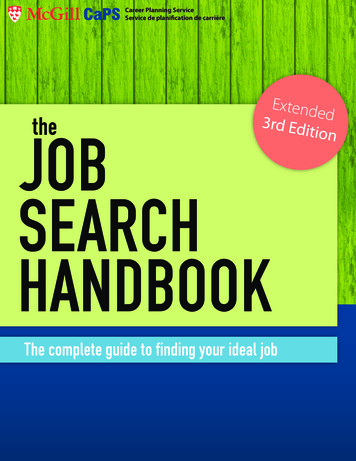
ED Fracture Guideline 2018UPPER EXTREMITYConsult ORTHOPAEDICS for follow-upAbbreviations:Above elbow A/EWrist Guard W/GDistal third of bone DISTALAge definitions:YOUNG 10 or 12FractureElbowDetailsDislocationOLDER 10 or 12Indication toreduceImmobilizationtypeReduce in ED and note“stability” post-reductionon referralA/E Slab1 weekA/E Slab1 weekOlecranon undisplacedHumerusBelow elbow B/ESalter-Harris Classification SHFollow up guidelinesOlecranon displacedCALL ORTHOPEDICSOperativeLateral condyleCALL ORTHOPEDICSUsually operativeMedial epicondyle displacedCALL ORTHOPEDICS1 weekMedial epicondyleundisplacedCALL ORTHOPEDICSA/E3 weeksEffusion (fat pad sign)YOUNG, A/EOLDER, Sling 3 weeks 1 weekSupracondylar Type IA/E3 weeksSupracondylar Type II or III(displaced)CALL ORTHOPEDICSOperativeYOUNG, f/u PRN 6 weeks-Stevenson x 4 weeks-No sports for 8 weeksNeck undisplacedNeck displacedCALL ORTHOPEDICS(ONLY IF “OLDER”)ShaftShoulderDislocationReduce in EDStevensonOLDER, 4 weeksStevensonYOUNG, 4 weeksOLDER, 1 weekStevensonYOUNG, 4 weeksOLDER, 1 weekStevenson2 weeks3
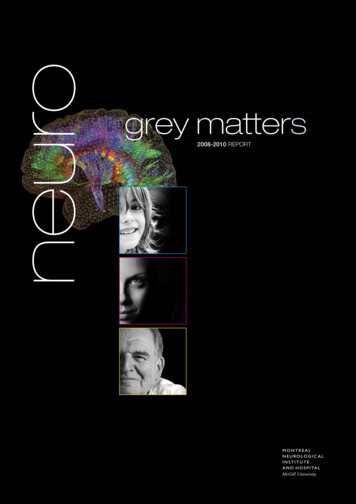
ED Fracture Guideline 2018UPPER EXTREMITYConsult ORTHOPAEDICS for follow-upAbbreviations:Above elbow A/EWrist Guard W/GDistal third of bone DISTALAge definitions:YOUNG 10 or 12Below elbow B/ESalter-Harris Classification SHOLDER 10 or 12Undisplaced: ALL agesClavicleDisplaced:Girls 12 and Boys 14Displaced, comminuted, ortenting:Girls 12 and Boys 14Sling PRN 1st weekNo contact sports x 3 monthsPRN f/u if still in pain 2 monthIF interested in operativeoption, f/u 1 weekStevensonIF not interested in operation,f/u 4 weeks4
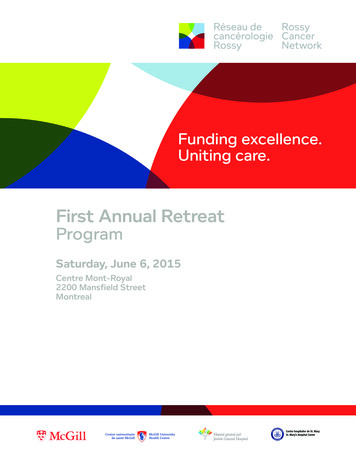
ED Fracture Guideline 2018LOWER EXTREMITYConsult ORTHOPAEDICS for follow-upAbbreviations:Above knee A/KNon-walking cast NWDistal third of bone DISTALFracturePelvisDetailsHip Dislocation / FracturesIndication toreduceBelow kneeWalking castProximal third B/K WC PROXIMALImmobilizationtypeFollow up guidelinesCALL ORTHOPEDICSIschial tuberosity 5 mm 1 weekAvulsion fracturesCrutchesFemurAll types of fracturesCALL ORTHOPEDICSKneePatellar dislocationReduce in EDPatellar fracture/dislocationwith osteochondral fragmentZimmerAce bandage2-3 weeksPhysio PRNPRN f/u if pain 2 weeksTibial tuberosity avulsion withloss of active extensionCALL ORTHOPEDICSOperativeTibial spineCALL ORTHOPEDICS1 weekProximal BuckleShaft undisplacedShaft displacedSuspected toddler’s fracture4 weeksA/K NW(in PLASTER)1 week1 weekB/K WC(A/K if PROXIMAL)Option 1: Watchful waitingOption 2: B/K WC if significant painCrutches SlabPRNShaft (displaced or undisplaced)MaisonneuveAK NWCALL ORTHOPEDICSToddler’s fracture(i.e. no cortical disruption)Fibula(Proximalor Shaft)Often operativeCALL ORTHOPEDICSEffusion without fractureTibia(Proximalor Shaft)All others (displaced or not) 4 weeks4 weeks PRN f/u 6 weeks 4 weeks1 weekCALL ORTHOPEDICS5
ED Fracture Guideline 2018LOWER EXTREMITYConsult ORTHOPAEDICS for follow-upAbbreviations:Above kneeNon-walking castDigit NumberFractureAnkleDetails A/K NW D#Indication toreduceOption 1: ankle sprainOption 2: B/K WC if significant painDISTAL tibia undisplaced(Buckle, SH-1,2, avulsion)MetatarsalB/K SlabFollow up guidelines“Ankle sprain kit” No sports x 4 weeks 4 weeks1 weekCALL ORTHOPEDICS1 weekDisplaced/Unstable Tib-FibCALL ORTHOPEDICS1 weekTillaux or Triplane fractureCALL ORTHOPEDICS1 weekSpiral fibula (Weber a,b,c)CALL ORTHOPEDICS1 weekHard shoeD1 or D2-5 UndisplacedIntra-articular or displacedConsider B/K WCCALL ORTHOPEDICSNo f/u4 weeks (if casted)1 weekStress fracture 5th metatarsal“dancer’s fracture”B/K NW4 weeksJones fracture(5th metatarsal)B/K NW6 weeksHard shoe4 weeks4 weeksBase 5th AvulsionPhalynges B/K WCDISTAL tibia or fibuladisplaced SH-1,2, andany SH-3,4,5Multiple fracturesStressJonesAvulsionImmobilizationtypeAce bandageSprainDISTAL fibula undisplaced(Buckle, SH-1,2, avulsion)Below kneeWalking castD1 (proximal phalynx)Reduce if clinicaldeformityB/K WCD1 (distal phalynx, any)D2-5 (any)Reduce if clinicaldeformityHard shoe buddy tapeMultiple fracturesHard shoeConsider B/K WCNo f/u4 weeks (if casted)6
ED Fracture Guideline 2018HAND & WRISTConsult PLASTICS for follow-upAbbreviations:DigitDistal inter-phalyngealProximal inter-phalyngealPreformed splint3-way slabBelow elbowFractureDetailsFingerDislocationD2-5Distal Phalynx D DIP PIP Splint Slab B/EIndication toreduceReduce in EDTuft aloneTuft with nailbed injuryRepair as indicatedMalletD2-5Middle nge of motionFollow-upSafe positionImmobilizationtype1 weekBuddy tape PRNNo f/uSplint DIP1 week24/7 splint inhyperextension1 week1 weekCALL PLASTICS(r/o Seymour fracture)24/7 splint inhyperextensionShaft (unstable)Reduce in EDangulated or scissoringSplint DIPBuckle, SH-1,2Reduce in EDangulated or scissoringVolar Plate(sprain or fracture)Follow up guidelinesSafe SlabMallet with nailbed injury MC MCP ROM f/u safeIf reduced, 1 weekAll others, 3 weeksIf reduced, Slab insafe 1 weekAll others, buddytape PRN 3 weeksBuddy tapeNext clinic ( 72 hours)Condylar fracture (unstable)Consider reduction inED (unstable)Slab in safeNext clinic ( 72 hours)Shaft (unstable)Reduce in ED ifangulated or scissoringSlab in safe1 week7
ED Fracture Guideline 2018HAND & WRISTConsult PLASTICS for follow-upAbbreviations:DigitDistal inter-phalyngealProximal inter-phalyngealPreformed splint3-way slabBelow elbowFractureD2-5MetacarpalDetailsIndication to reduceNeck (minimal or noangulation)D2-3 20 degreesD4-5 40 degreesNeck (angulated)D2-3 20 degreesD4-5 40 degreesor ScissoringD1 “thumb” D DIP PIP Splint Slab B/EReduce in EDImmobilizationtype MC MCP ROM f/u safeFollow up guidelinesB/E in safe3 weeksSlab in safe1 weekShaft or BaseReduce in ED if angulatedor scissoringIf reduced, slab insafe 1 weekAll others, B/E insafe 3 weeksPhalynx(Distal or Proximal)Reduce in ED if angulatedor scissoringIf reduced, slab 1 weekAll others, thumbspica 3 weeksIf UCL instability,slab Next clinicAll others, thumbspica 3 weekUlnar Collateral Ligament(UCL; sprain or fracture)MetacarpalReduce in ED if angulatedor scissoringRolando or e of motionFollow-upSafe positionFracture seen on X-raySuspectedCALL PLASTICS(consider CT)If reduced, slab 1 weekAll others, thumbspica 3 weeksSlabNext clinic ( 72 hours)Slab 1 weekSlab2 weeks8
- Approved by MCH Divisions of Emergency, Orthopedic, Plastic Surgery, and Trauma, July 1, 2018. Montreal Children's Hospital - McGill University Health Center Emergency Department Fracture Guideline Disclaimers This document is designed to assist physicians working in our emergency department in caring for children (under 18 years of