Transcription
This chapter is part of a record of the history of the Department of Anatomy and Cell Biology at McGill Universitywritten by Emeritus Professor, Dr. Gary Bennett, and completed in 2016. The entire history can be accessed istory.History 5 - Fire in the Medical Buildings to SelyeFire in the Medical Buildings (1907)At the beginning of the 20th century, the infrastructure of McGill University become veryimpressive. Thanks to generous benefactors such as MacDonald, Molson and Lord Strathcona(now the University Chancellor), several new buildings had been constructed. In addition to theArts Building and Dawson Hall, at the top of University Drive, there was the magnificentRedpath Museum to the west, and beyond this the new Redpath Library. To the east were thenew Engineering, Chemistry and Physics Buildings. North of these was the new, greatlyexpanded, Medical Building, and finally, up the hill was the glorious new Royal Victoria HospitalFrost 2:4.In 1907, however, disaster struck! A fire of unknown origin destroyed much of the preciousnew Medical Building Hanaway 2: 64-66. The central portion was completely gutted and its roof andcupolas collapsed. The original lower portion was also damaged beyond repair. Only thenorthern-most Molson Extension survived to be reutilized. The Anatomy museum wascompletely destroyed, along with all the specimens that Shepherd had collected over 30 years!The pathology museum also suffered major losses, but most of the Osler Collection, includingthe wonderful Holmes heart, was saved by the heroic efforts of Maude Abbott and the medicalstudents. The latter sifted through the rubble containing broken museum jars, and, withbleeding hands, saved what they could. Lectures were temporarily held in the Arts, Physics andChemistry buildings for the remainder of the year.1
The Strathcona Medical Building (1911 – Present)Clearly a new building was urgently needed. The insurance of the old structure was insufficient.Many McGill alumnae and other citizens contributed money, but this was not enough to build anew facility. Then Lord Strathcona came once more to the rescue and provided all thenecessary funds for another new medical building. This would be called the Strathcona MedicalBuilding, and was to be located on the southwest corner of Pine Avenue and University Street,south of the Royal Victoria hospital Frost 2:83. Since this land was not part of the original McGillcampus, Lord Strathcona also supplied more than 500,000 for its purchase and forconstruction costs. Plans for the new building were commissioned from Percy Nobbs, McGill’sprofessor of architecture.The east wing of the Strathcona Medical Building was opened in 1909, and the remainder of thebuilding was completed by 1911 Hanaway 2:67. On June 5, 1911, the building was formally openedby the Governor-General Lord Grey in his capacity as the Official Visitor to McGill University.The University Convocation ceremony was held on the same day, and the occasion was used towelcome back 600 graduates who had come for their first McGill Reunion.2
As described by a 1911 article in the British Medical Journal, “The building is of the highestmodern steel construction, and is thoroughly fireproof. The exterior of the whole building isconstructed of finely-cut Montreal limestone, and the roof is covered with green slate andcopper flashings. All the windows are fitted with steel frames and sashes. The corridors havemosaic floors, with marble borders, and all other floors are of hard wood; the finish throughoutis of white quartered oak. The entrances from the Campus and from University Street are bybroad flights of granite steps, through vestibules finished with gray sandstone, with vaultedterra-cotta ceilings. Two separate staircases, finished with ornamental balustrades of wroughtiron, with marble steps of ample width, lead to the upper floors. (It may be noted that, onehundred years later, the upper surfaces of the marble steps of the main staircases exhibit largeconcave depressions after use by countless thousands of students and staff!) The walls of thestaircase halls, as well as the corridors, are lined with low glazed terra-cotta to a height of 8 ft.”This sumptuous Strathcona Medical building was described in the local press as “unsurpassedfor efficiency” and much praised for its architecture and fitting Frost 2:83.The building consisted of a southern main portion and three wings (east, central and west)extending northward. The three floors were named according to the European system, with astreet-level ground (main) floor and, above this, first and second floors. The main entrance tothe building was at the eastern end of the front of the building facing the campus. At thisimpressive entrance were posted one or two doormen who acted as porters.3
4
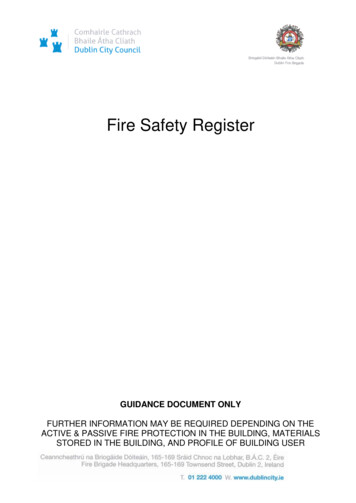
The main (southern) part of the building housed the 60,000 volume medical library. Its elegantreading room and journal room spanned most of the top (2nd) floor. This elegant room had abeautiful skylight ceiling and the large stained-glass southern windows contained images ofhistorical medical personages. On the walls and surrounding bookshelves were portraits andmarble busts. Below the reading room, there were glass-floored library stacks on the 1st floor,and cataloging rooms on the ground floor. Small circular stair cases connected these floors.When McGill University received the Osler Library from Oxford some years later, Percy Nobbsdesigned elegant rooms on the second floor of the central portion opposite the medical library.The chair of the Anatomy Department, S.E. Whitnall was in charge of the arrangements for thetransfer, and the official opening of the library took place in 1929 Hanaway 2: 132. In the floor of thehallway leading to the Osler Museum is a stone slab which exhibits a pattern resembling a crosssection of the spinal cord. This has remained in our building after the transfer of the OslerLibrary to the McIntyre building in 1966.5
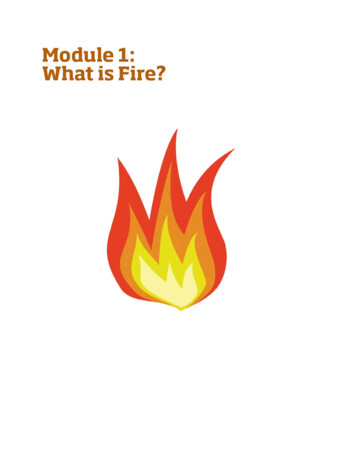
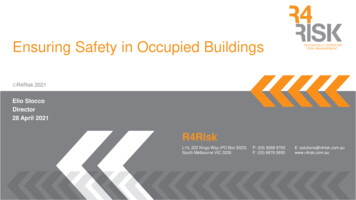
Lecture theatres were found on the ground and 1st floors. On the second floor was an anatomytheatre with an epidiascope. This theatre, with its long curved benches (see floor plan)resembled the one in McGill’s original medical building. It was renovated in the 1960’s tobecome a more functional but much less remarkable lecture theatre!The center wing containing the octagon contained the McGill Medical Museum which isdescribed in detail in a following section of this work. The west wing contained an AssemblyHall seating up to 400 persons on the ground floor, along with the Departments of Hygene,Pharmacology and Experimental Medicine on the upper floors.The east wing housed the Faculty of Dentistry and the Anatomy Department. The AnatomyDepartment was described in detail fifteen years later in a 1926 paper written by its chairEarnest Whitnall. In the basement was the mortuary which housed eighty cadavers in airtightspirit-vapor chambers. Adjoining was the preparation room. Also on this floor was a large lockerroom with 400 steel student lockers, the students’ lavatory (male only) and the students’reading and smoking room. The latter was provided with newspapers and magazines under thecontrol of the students themselves. The ground floor was reserved for the Faculty of Dentistry.The first floor contained the Anatomy Department’s large Histology laboratory in addition to6
the professor’s office, as well as a number of research laboratories and offices for the staff andother workers.Laboratories throughout the building had natural gas outlets at every bench for the use ofBunsen burners (some of which were used to brew coffee)! The water taps in the laboratorieshad a side portal which, when the water was running, served as a suction device. As a result,dangerous chemicals could be sucked into the water supply. This necessitated that all city watercoming into the laboratories had to be stored in a large cistern in the basement. This water wasconsidered unsafe to drink, and drinking water was provided by water fountains in thehallways.In the days before each laboratory had its own freezer and refrigerator, there was a commonrefrigerated room, the “cold room” in which many chemicals and samples were kept. In lateryears, when the when the use of radioactive isotopes became a hallmark of our Department, allexperiments using these isotopes were carried out in a special “hot lab” in the east wing.Isotopes whose radiation travelled a significant distance (e.g. iodine) had to be kept in thickwalled lead containers. In later years, the most common isotope used was 3H-tritium.Molecules labeled with this isotope (amino acids, sugars or nucleotides) were purchased fromsupply companies in aqueous solution. The volume of solution often had to first be reduced byevaporation under a stream of nitrogen, followed by intravenous injection into animals. Inorder to save on the cost of isotopes, small animals such as mice or baby rats were used. Eventhen, the cost could be huge in any one injection, i.e. several hundred dollars in the 1960’s(several thousand dollars today). The isotope solution had to be successfully injected7
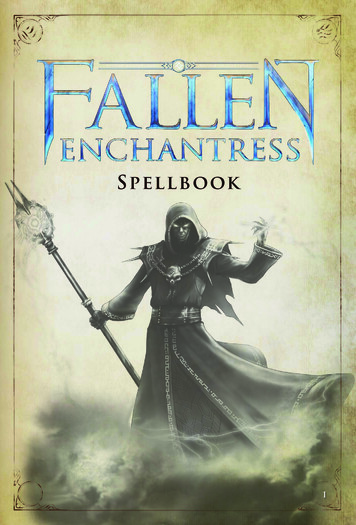
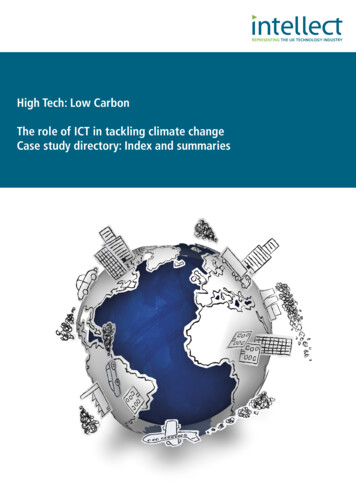
intravenously into the animal, using surgery to reveal the internal jugular vein. The biggestchallenge came at the time of sacrifice of the animal, since, to achieve quality fixation of tissuesnecessary for EM examination, it was essential to successfully perfuse the animal withglutaraldehyde fixative. This was done by surgically opening the thorax and injecting the fixativedirectly into the left ventricle of the heart via a perfusion system. If a successful perfusion wasobtained, the whole body soon stiffened. If not, the experiment was recognized as being afailure in terms of obtaining quality results. Many tense moments were experienced by theteam of young investigators on these occasions. The animals were anesthetized using ether,which was often liberally used to ensure that the animals remained unconscious. As the roomfilled with ether fumes, little attention tended to be was paid to the well-being of the humaninvestigators, or to the fact that an explosion could have blown up the whole hot lab!A mezzanine floor located between the first and second floors of the east wing had rooms forthe Professor of Surgery and offices for the Canadian Medical Association. The second floorcontained the large Gross Anatomy dissecting room which was 90 feet long and lighted onthree sides with large windows and a large skylight extending the whole length of the room.The walls consisted of white enameled brick, and the floor was of vitrified tile. Large framedanatomical illustrations graced the walls. There were 40-50 wooden dissecting tablesaccompanied by numerous metal stools. The tables were later replaced by ones of stainlesssteel. In addition to the main lab, there were small rooms for demonstrators and assistants, alarge general research laboratory and a (male) students’ washroom.8
9
The whole building was electrified, and the east wing even boasted an electric passengerelevator Frost 2:83 with a steel cage. An additional elevator was used to bring cadavers from thebasement up to the dissecting room on the top floor. The main elevator was operated by a fulltime staff member.10
For many years, our Department had its own animal room, located in the attic floor above thegross anatomy facility, and run by one or two technicians. The facility housed mainly rats andmice, which were the chief experimental models of research investigations of this era.Fortunately, in recent times, these laboratory rats were the only ones found in our building, asopposed to the wild rats which occupied the walls in former eras. During the early years,however, our animal facility was home to a huge colony of cockroaches which would dispersenoisily at the sound of footsteps on the stairs leading up to the attic room.In 1978, our Departmental animal facility closed, and the animals were transferred to a centralanimal facility. With time, much research emphasis has switched to the use of cell lines or totransgenic mice. A colony of frogs is still maintained in our attic by Craig Mandato.Curricular Changes: The five-, six-, and proposed seven-year courses (1910 - Present)In the early days, most students entered medicine directly from high school, and had had nouniversity level science training. Thus basic courses such as Chemistry, Physics and Biologyneeded to be taken in the first year of the curriculum. The major medical courses, e.g.Anatomy, Physiology, Biochemistry, and Pharmacology and Therapeutics were taken over aperiod of two years Hanaway 2: 67. Minor courses, such as Histology, were taken for one year oreven one semester. Clinical subjects like Medicine, Surgery, Obstetrics, Diseases of Infants, andGynecology were taken in the senior two years. A new course in Clinical Microscopy wasintroduced, and students had the use of microscopes in the hospitals for doing simplelaboratory tests such as blood smears and urinalysis. Failure in one or two subjects required asupplementary examination. Failure in more than two subjects or in Anatomy or Physiologymeant repeating the year. Hanaway 2:67.In 1910 a fifth year was added to the medical curriculum in order to allow graduating studentsto gain more practical medical and surgical experience in the hospital wards. Hanaway 2: 67. Then in1919, for similar reasons, the medical curriculum was still further extended to become a sixyear course Hanaway 2: 68.In the years that followed, discussions continued as to which curriculum formula, in terms oflength and content, would best achieve the desired learning goals. Certain faculty members,particularly Earnest Whitnall in Anatomy, and J. Tait in Physiology, with their Britishbackground, wanted to lengthen the curriculum to 7 years as was often done in that countryHanaway 2: 121. Instead, it was decided to shorten the curriculum by instituting two fundamentalchanges:11
Firstly, by 1923, it was realized that many first year medical students had already taken part orall of an undergraduate B.A or B.Sc. degree at McGill or other universities. In 1902, a “DoubleCourse” had also been introduced at McGill in which outstanding students could enroll in aBachelor of Arts or Applied Science for two years, and then enter the four year Medicalprogram. After two years in Medicine they would receive credit for basic science courses in themedical curriculum and would automatically be awarded a Bachelor’s degree Hanaway 2:9. Thispractice continued until the 1960’s.Since many students had completed first year basic science courses (Chemistry, Physics andBiology) during their undergraduate studies, McGill now decided that the minimal entrancerequirement for the medical school would be three years of a B.A. or B.Sc. degree with theinclusion of the above courses. By this means, the medical course was shortened from six tofive years Hanaway 2:121.Secondly, by 1934, it was felt that the responsibility for the extended clinical training in the finalyears of the curriculum should be transferred from the medical school to the hospitalsthemselves. This was because the university did not have jurisdiction and control over theclinical training of students in the hospitals. By this change (and slightly lengthening theacademic year), the medical curriculum was shortened from five years to four years Han 2: 122. Afundamental consequence of this shift, however, was that students did not become qualified topractice medicine after graduation from the university, but instead were required to completea hospital internship before receiving a license to practice.After Quebec’s quiet revolution in the 1970’s, the Parent Commission introduced the CEGEPsystem, whereby the French classical colleges were discontinued, and upon finishing highschool, all students interested in proceeding to university education were required to firstenroll in a two year CEGEP diploma program Frost 2: 407. Following this, students would attenduniversity for three years to obtain a Bachelor’s degree.For entry into medical school, by this time, most North American universities required aBachelor’s degree. The Quebec Government, on the other hand, proposed that students shouldbe accepted in the medical school directly from CEGEP. McGill objected to this and was allowedto require that students complete one university pre-professional year before being acceptedinto medicine Frost 2: 407. This arrangement remains in place until the present day. About half ofour current students are accepted into medicine after completing a Bachelor’s degree or evenmore advanced graduate training. The other half enter medicine after a “Med-P” year at McGillin which they are registered in a Bachelor’s program. Acceptance into this Med-P program fromCEGEP is highly competitive. During this pre-professional year they are required to pass coursesin certain prerequisite subjects (such as Cell Biology and Physiology) and to maintain a12
minimum grade average. In the other francophone Quebec medical schools, students areaccepted from CEGEP directly into the medical school.The New Biology Building (1922)After completion of the Strathcona Medical Building, it was decided that, of the basic sciencesof the medical curriculum, Anatomy, Histology, Embryology, Physiology Pathology, andBiochemistry would be taught in the Strathcona Medical Building (SMB), while OrganicChemistry and Biology would be taught in that portion of the Old Medical building (i.e. theMolson Extension) which had survived the fire of 1907. In 1922, a new Biology building waserected on the site of the original portion of the Old Medical Building. This now housed theDepartments of Botany and Zoology (in the Faculty of Arts), along with the Departments ofBiochemistry, Physiology, Pharmacology, and Experimental Medicine (in the Faculty ofMedicine) Frost 2:122, 165. The Molson Extension of the original medical building complex, remainedattached to the back of this new building, and continued to be used for some years Hanaway 2: 69.13
In 1924, the Departments of Pathology and Bacteriology were transferred to the newly-builtPathological Institute Hanaway 2:69, Frost 2:122, 165.In 1965, the new circular McIntyre Medical Building was erected, named for the McIntyrefamily which donated the land for all the north-western campus buildings Frost 2: 433. The Facultyof Medicine Departments of Biochemistry, Physiology, and Pharmacology, as well as theMedical Library were transferred to this new building. The Osler Library was completelydismantled and its rooms were reconstructed at this new site.At the same time as the opening of the McIntyre Building, the Departments of Botany andZoology were transferred from the Biology Building to the new Stewart Biology Building. Theold Biology building was then completely gutted and renovated, and became the new CyrilJames Administration Building. The building was given an additional floor during this extensiverenovation, but it still reveals its biological past by retaining the statue of the frog crouchedover its doorway Frost 2: 433.This left the Strathcona Building in the hands of the Anatomy Department and the Faculty ofDentistry. The upper floors of the east wing continued to house the Polypeptide Laboratory ofthe Department of Experimental Medicine. The main medical library reading room on thesecond floor became the Anatomy Department Reading Room as well as the office andlaboratory of Dr. Osmond.Maude Abbott (McGill: 1898-1936) and Women in the Medical CommunityThe story of women’s admission to McGill University is a long and fascinating one! Whenwomen such as Maude Abbot aspired to obtain higher education in the late nineteenth century,huge odds confronted them. In the McGill academic community, there were two broad campsof opinion regarding the status of women. One camp was represented by Principal WilliamDawson. He agreed that women should be educated, but he felt that a woman should beforemost a “lady, wife, mother and homemaker”. He felt that women were emotionally andspiritually refined, possessing a precious quality which must not be coarsened by too muchcontact with male society Frost1:253. He therefore believed that her education should be largelycultural and certainly given separately from men Gilette: 2, Frost 1:252.This chivalrous view was perhaps charming, but was in fact strongly discriminatory. Under thelaw, women were classified with children, criminals and idiots. After her wedding, a womanunderwent civil death: in marriage, a man and woman became one, and he was “the one” –with all the legal rights Gilette: 2. There was a strong feeling that women could not stand themental strain of higher education. It was also felt that such an education would contain many14
subjects that a woman should not even know about, including sex, violence, and money.Dawson believed that male and female intellectual capacities were different and divinelyassigned. In the great Nature versus Nurture controversy raging during this era, Dawson stoodfirmly on the side of Nature. Although he was a scientist, he rejected Darwin’s theory ofevolution and maintained a staunch belief in the Biblical explanation of the origin of life. Thisliteralist approach to Christianity had marked implications for his attitude towards theeducation of women Gillette: 28.The opposite camp of opinion was represented by Dawson’s colleague, J. Clark Murray. Astimulating lecturer in the humanities, and one of McGill’s most popular professors, Murrayregarded a woman as “a person, an independent being and potential worker”. He consideredthat women should have access to exactly the same education - including professionaleducation - as men, and in the natural company of men Gillette: 2; Frost 1: 255. In the above Natureversus Nurture controversy, Murray was strongly on the side of Nurture. He agreed with JohnStuart Mill that “what is called the nature of Woman is an eminently artificial thing, the result offorced suppression in some directions, and unnatural stimulation in others” Gillette: 1,2,3.In the United States, higher education for women was somewhat accepted by the mid 1800’s.Oberlin College admitted women in 1837, and Vassar College for women was founded in 1865Frost1: 252; Gillette: 9. The first Canadian college to admit women was Mount Allison in NewBrunswick in 1862, but it did not produce a female graduate until 1874. In the moreconservative province of Quebec, women were admitted to the Faculty of Arts at McGill only in1884. Laval did not admit women until 1910, and l’Université de Montreal until 1915 Frost1:252,Gillette: 11.At McGill, Principal Dawson had many supporters in his position that there should be no coeducational university courses for men and women, and in the end, his policy of separateeducation for women won the day. The resultant need to provide separate classes for women,however, posed a financial obstacle that delayed the admission of women to the university forsome time. The problem was finally solved via the generosity of Donald Smith (LordStrathcona), who shared Dawson’s views on women’s education. He provided a separateendowment for their education and built the very impressive Royal Victoria College for femalestudents Frost1:253; Frost 2: 8. Maude Abbott, and the other young women who were enrolled in thisBachelor of Arts program in 1880’s, were called “Donaldas” in recognition of their support fromDonald Smith Han2: 48. They turned out to be excellent students and graduated with brilliantperformances. Miss. Octavia Ritchie was voted valedictorian of her class and gave anoutstanding valedictorian address at graduation. Prejudices about the capacities of womenpersisted, however, and, after the ceremony, she was asked, in a caring fashion, “And are younot very tired my dear” Gillette:109 ?15
Having overcome the first obstacle of admission to Bachelor’s programs, some of these youngwomen aspired to enter the McGill Medical School. This was another huge hurdle, however,since resistance was especially strong in the “male” professions of Medicine, Dentistry, Law andEngineering. Why would a woman want to do what was considered to be a man’s work? Thefamous Oxford professor Charles Dodgson (alias Lewis Carroll – the author of “Alice inWonderland”) even considered such a woman to be a modern social monster, the “he-woman”Gilllett: 8. An article in the Cologne Gazette, in 1888, described such women as “having lost allwomanly emotions. Truly educated and cultured men would avoid them, uneducated oneswould flee them, and healthy natural women would shun their society” Gilllette: 14.Extreme views even came from the medical community when Edward Clarke, a physicianassociated with Harvard University, asserted in 1873 that “women were prone tooverexcitement and should not be placed in competition with men. Co-education would beextremely harmful and could induce neuralgia, uterine disease and hysteria, possibly to theextent that their children might be born deformed” Gillette: 16.This prejudiced attitude about women’s mental status had in fact existed throughout history. Inantiquity, Egyptian manuscripts dating back to 1900 B.C. ascribed women’s depressivesymptoms to spontaneous displacements of their uterus Tasca: 2. In 400 B.C., the Greekphilosopher Plato also propagated the myth of the wandering womb Knight: 141. He believed that,if unused for long periods, the uterus took to moving around in the body, disturbing the body’sspirits, blocking channels, and causing a form of mental illness. The term “hysteria” for thisexclusively women’s disease was coined by Hippocrates based on the idea that it was caused bya wandering of the uterus (Greek: hysteron) Tasca: 2 . This concept, persisted for over threethousand years along with mainstream thought that the woman is a physically and theologicallyinferior being (St. Thomas Aquinas asserted that “a woman is a failed man”) Tasca: 4. During theMiddle Ages and Renaissance, hysteria was considered indicative of witchcraft and thousandsof innocent women were executed until the practice finally ended in 1782 Tasca: 7.In the 1700-1800’s, the cause of hysteria slowly became associated with the brain rather thanthe uterus. As early as 1680, Thomas Sydenham had indicated that the primary cause ofhysteria was not the uterus Tasca: 2. However old concepts die hard. Even during the VictorianAge (1837-1091) most women carried a bottle of smelling salts. If they swooned when theiremotions were aroused, it was believed, as postulated by Hippocrates, that the pungent odorwould cause the uterus to return to its natural place, allowing them to recover theirconsciousness Tasca: 8.It should be noted that, in spite of their generally inferior status, individual women sometimesplayed important professional roles. During classical antiquity and during much of Europeanhistory, there had been many instances of women in medical practice and as faculty members16
in universities. An example is Trotula de Ruggiero, a faculty member of the University of Salernoin the 11th century who is considered the first female doctor in Christian Europe Tasca: 4.In the 1800’s however, especially in Victorian British and American societies, a trend of thoughtstarted to develop that considered femininity an essential nature and delegated women to aspecific social mission: to be mothers and guardians of virtue (see comments of PrincipalWilliam Dawson earlier) Tasca: 7. If women broke away from these normal natural functions theywould be subject to mental illnesses such as hysteria (see comments of Edward Clarke above).The standards of these societies regarding the role of women essentially prevented them fromentering higher education and professional practice. Occasional women went to great lengthsto overcome this barrier. Dr. James Miranda Stuart Barry, for example, disguised herself as aman in order to take a medical degree at Edinburgh University in 1812. She maintained thisdisguise for the rest of her entire medical career, and the discovery of this ruse after her deathcaused a great scandal in the medical establishment Gillett: 280.In North America, by the second half of the 19th century, some progress had been made inproviding medical education for women. At first there were separate medical schools such asthe New England Female Medical College in Boston in 1848 and the Philadelphia Women’sMedical College in 1850 Gillette: 280.In Canada, women were admitted into mixed medical classes at Queen’s University in Kingstonin 1880, but the women were subjected to such antagonism by both teachers and malestudents that they had to be given separate lectures. The outraged women finally transferredto the new Women’s Medical College in Kingston Gillette: 282.17
At McGill, Octavia Richie and Maude Abbott, both outstanding graduates from McGill’sBachelor of Arts program, applied to the Medical school in 1888 and 1889, but were instantlyrefused Gillette: 282; Hanaway 2: 48. This was at a time when admission standards for men were quitelow, requiring only a high school graduation with modest scores. Only a minority of the malecandidates had a college degree Hanaway 2:49. The obstacle encountered by Olivia Richie andMaude Abbott was a stone wall created by chauvinism, prudishness, stubbornness andtradition. “Women belonged in the home and were unsuited to a physician’s public life. Theirendurance was limited, their nerves were weak, and they were not mature enough or preparedfor the stress involved. They would become hardened and defeminized, especially by the studyof Anatomy with its dissection course Gillette: 287”!Even the male medical students were openly opposed to admitting women Hanaway 2:48. Whilesome professors were supportive, realizing the value of women doctors in such fields asobstetrics and gynecology or pediat
The insurance of the old structure was insufficient. Many McGill alumnae and other citizens contributed money, but this was not enoughto build a . The center wing containing the octagon contained the McGill Medical Museum which is described in detail in a following section of this work. The west wing contained anAssembly