Transcription
2/27/2020Board of Pharmacy UpdateMARCIE BOUGH, PharmDEXECUTIVE OFFICERJOHN DOUGLAS, RPhBOARD INSPECTORCertification in Sterile Compounding for Inspectors (CISCI)March 1 , 2020Recent Drug Developments and Law Update 2020University of Montana Skaggs School of PharmacyDisclosureThe presenters declare no actual or potential conflictof interest in relation to this presentation.1
2/27/2020Objectives1. Understand laws and regulatory updates related to theBoard of Pharmacy.2. Discuss changes to USP 797 2019 compared to the2008 version.QuestionsWhat are the 2019 legislative topics related to the Montana Prescription DrugRegistry (MPDR)?A. FundingB. Integration into electronic workflow systems in medical and pharmacypracticesC. Mandatory registrationD. Mandatory use by prescribers of opioids or benzodiazepines effective July2021E. All of the aboveOne major change in the 2019 version of USP 797 relates to the requiredfrequency of viable surface sampling in the certified area. How often mustsurface sampling be done in each certified area?A.B.C.D.E.Every MonthQuarterlyEvery six monthsAnnuallyAt the time of PEC certification2
2/27/2020Board of Pharmacy MembersTony King, Pharmacist, PresidentStarla Blank, Pharmacist, Vice-PresidentMarian Jensen, Public Member, SecretaryCourtney Bahny, Certified Pharmacy TechnicianMike Bertagnolli, PharmacistPaul Brand, PharmacistCharmell Owens, Public MemberBoard of PharmacyContact Information and MeetingsMarcie Bough, PharmD, Executive Officer406-841-2371, mbough@mt.govGeneralEmail: dlibsdpha@mt.govWebsite: www.pharmacy.mt.govJohn Douglas, RPh, Board Inspector406-431-1952, jdouglas@mt.govPhone: 406-841-2300Mark Klawitter, RPh, Board Inspector406-459-8847, mark.klawitter@mt.gov2020 Board MeetingsCustomer Service: 406-444-6880March 13June 12[Vacant], Program ManagerMontana Prescription Drug Registry (MPDR)406-841-2240, dlibsdmpdr@mt.govSeptember 182020 Subcommittee MeetingsMarch 12, Automated DispensingSystemsApril 16, Technicians3
2/27/2020MontanaPrescription Drug Registry(MPDR)www.MPDR.mt.gov4
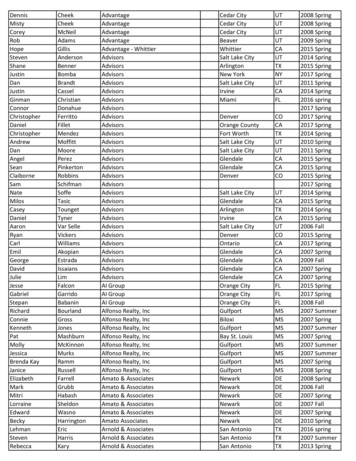
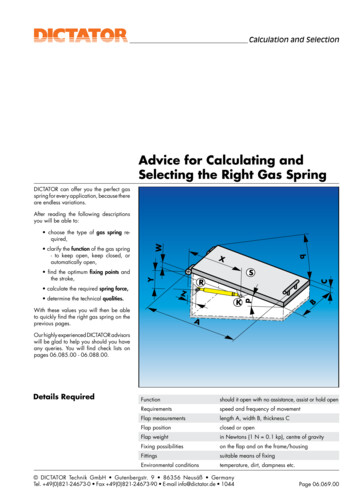
2/27/2020MPDR Interstate Data Sharing Map indicates statesconnected to NABP’shub (August 2019) MPDR is currentlysharing with 25other states:Alaska, Arizona,Arkansas, Colorado,Idaho, Illinois,Indiana, Iowa,Kansas, Louisiana,Michigan, Minnesota,Mississippi, Nevada,New Mexico, NorthCarolina, NorthDakota, Ohio,Oklahoma, SouthCarolina, SouthDakota, Texas,Virginia, Washington,and Wisconsin. Additional states willbe added in thefuture.MPDR Legislative AuditInformation Systems Audit, The Montana Prescription Drug Registry,18DP-01, Final Report June 2019 9 Recommendations–––– Department of Labor and Industry’s Response Included in Final Report–––– Contract management, governance and resources, securityFunctionality, delegate accessData destruction, data reporting and validation, data analysisUtilization of MPDR Advisory GroupOngoing improvements since launched in 2012Future migration to a new vendor platform to improve functionalityTools and efficiencies in more advanced systemsData integration, MPDR Advisory Group, staffing/resourcesLegislative Audit Committee Meeting June 25, 2019–Report: on/audit/201920/Meetings/June-2019/18DP-01.pdf5
2/27/2020MPDR Next Steps Hire new pharmacist position for MPDR Program Manager Issue Request for Proposal for a new MPDR system vendor and migrate to anew online platform–Improve functionality, provide integration and new clinical tools for frontline users,increase use, and improve administrative procedures Continue to collect MPDR fees from all Montana licensed prescribers andpharmacists during license renewal Collaborate with boards, state agencies, associations, and other stakeholderson outreach/education Continue to implement recommendations from Legislative Audit and engageMPDR Advisory Group Continue to collaborate on MPDR data research with Department of PublicHealth and Human Services and other stakeholders2019 Law UpdatesHouse Bill (HB)Senate Bill (SB)Senate Resolution (SR)Montana Code Annotated (MCA)Administrative Rules of Montana (ARM)6
2/27/2020Montana Legislature: https://leg.mt.govSB 61, Revise Prescription Drug RegistrySponsor: Sen. MacDonald (D-Billings)Requestor: Board of Pharmacy/Department of Labor & Industry MPDR Funding–––Permanent funding through fee collectionFee set in rule commensurate with costAll licensees authorized under Title 37, MCA, to prescribe or dispenseprescription drugs are required to pay the MPDR fee Mandatory MPDR Registration for Prescribers and Pharmacists MPDR Data Integration into Electronic Workflow Systems in Medical andPharmacy Practices–– Electronic health records, health information exchange networks, and pharmacydispensing systemsOnline service will continue to be availableEffective 10/1/2019–37-7-1503(1) and 1511(1), MCA, and ARM 24.174.17127
2/27/2020HB 86, Generally Revise Prescription Drug Laws(1 of 2)Sponsor: Rep. Ricci (R-Laurel)Requestor: Department of Justice/Attorney General Tim Fox Require Positive Identification of Recipient of Controlled SubstancePrescription––Statute: driver’s license, school district/postsecondary photo ID, tribal photo ID,by Board ruleRule: valid government-issued photo ID, including but not limited to passport,military, or state-issued ID– Requires positive identification of recipient of controlled substanceprescription, with exceptions, and documentation– Prescriber 7-day Supply Restrictions for Opioid-naïve Patient–––– 37-7-410, MCA; ARM 24.174.842 as identified in MAR Notice No. 24-174-73Opioid-naïve defined as no opioid in past 90-daysDoes not apply: professional judgement of prescriber for treatment of chronicpain, cancer pain, palliative care pain; treatment of opioid abuse/dependence37-2-108, MCA; terminates 2025Pharmacists responsible for DEA corresponding responsibility (21 CFR 1306.04)and practice of pharmacy requirements (37-7-101(38), MCA)Effective 10/1/2019HB 86, Generally Revise Prescription Drug Laws(2 of 2)Sponsor: Rep. Ricci (R-Laurel)Requestor: Department of Justice/Attorney General Tim Fox Mandatory MPDR Use for Prescribers of Opioids and Benzodiazepines––– Mandatory MPDR Registration for Prescribers and Pharmacist– Does not apply: hospice, 7-day supply or less/no refills, administration in healthcare facility, or emergenciesUse for chronic pain patient required every 3 months37-7-1515, MCA; effective 7/1/202137-7-1503(1) and 1511(1), MCA, and ARM 24.174.1712Effective 10/1/2019 - Except MPDR Mandatory Use 7/1/20218
2/27/2020Other New Laws of Interest (1 of 2) SB 274, Revise Drug Scheduling LawsSen. Olszewski (R-Kalispell)––Listing of controlled substances updated to match recent DEA activityCannabis-related FDA approved drugs will match DEA schedule Changed dronabinol (Marinol) to Schedule III Added cannabidiol (Epidiolex) to Schedule V– 50-32-221 through 232, MCA; effective 4/12/2019HB 231, Revising Pharmacy Laws Regarding VaccinesRep. Knudsen (R-Malta)–––––Amends 37-7-105, MCA, Administration of ImmunizationsAdds pertussis vaccine to list of immunizations pharmacists canprescribe/administer independentlyAllows for age 7 and older through collaborative practice agreement per Centers forDisease Control and Prevention (CDC) guidelinesAdds various documentation, communication, and notification requirements37-7-105, MCA; effective 7/1/2019Other New Laws of Interest (2 of 2) HB 105, Revise Process for Out-of-State Licensure for Professional Licensing BoardsRep. Sullivan (D-Missoula)–Effective 3/20/2019 HB 137, Create a Statewide Drug Takeback Day HB 555, Ensuring Transparency in Prior AuthorizationRep. Dudik (D-Missoula)–Rep. Lenz (R-Butte)– Effective 1/1/2020HB 654, Generally Revise Laws for Funding Treatment CourtsRep. Brown (D-Bozeman)––– Effective 10/1/2019Department of Revenue licensing of wholesale drug distributors selling opioids into Montanawho are licensed by Board of Pharmacy 500 annual license fee to help fund treatment courtsEffective 5/6/19; license required after 6/30/2019SR 31, Confirm Governor’s Appointees to Health & Human Services Related BoardsSen. Howard (R-Park City)–Adopted by Senate 3/12/19; filed with Secretary of State 3/18/20199
2/27/2020Information on PBM Legislation SB 83, Establishing Allowable and Prohibited Practices for Pharmacy Benefit ManagersSen. Fitzpatrick (R-Great Falls)–– SB 270, Revise Reimbursement Conditions for Certain Pharmacies, PharmacistsSen. McNally (D-Billings)– Effective 7/1/2019SB 71, Regulate Health Insurers’ Administration of Pharmacy Benefits for ConsumersSen. Olszewski (R-Kalispell)–– Montana Pharmacy Association effortEffective 1/1/2020Requestor: State Auditor Matt RosendaleVetoed by Governor 5/9/2019; veto override vote failedHB 344, Require Transparency Reporting of Pharmacy Benefits ManagersRep. Kelker (D-Billings)–Passed House, Failed Senate Floor voteNOTE: PBM bills/laws relate to drug price transparency, reimbursement, and other pharmacy businessissues that are not related to Board of Pharmacy activity or authority but are included as informational.Contact the Montana Pharmacy Association for details.Regulatory Updates10
2/27/2020Board Rulemaking MAR 71 (1 of 2)Final Rule Montana Administrative Register (MAR) Notice No. 24-174-71Effective 9/21/2019 Pharmacist to Technician/Intern Ratio–– Technician-in-Training (TTR) Licensing–––– Expanded pharmacist to technician ratio from 3:1 to 4:1 and interns removed from countingagainst the ratioARM 24.174.711Changed how TTR are licensed; issue as temporary certified pharmacy technician (PTE)license valid for 1 yearMust meet PTE requirements except for completion of certification examLogistics: license is still called TTRARM 24.174.701Internship and Preceptor Requirements–––––Removed requirements for interns to report hours to the BoardRedirects intern paperwork, forms, documentation, and reporting of hours to pharmacyschool(s)Removed intern limits for preceptorsRevised other related intern/preceptor requirementsARM 24.174.602, 604, 612Board Rulemaking MAR 71 (2 of 2)Final Rule MAR Notice No. 24-174-71Effective 9/21/2019 Collaborative Practice Agreements–– Prescription Transfers–– Aligns with Department standardsARM 24.174.2104Military Training and Experience for Licensure–– Revised to better reflect current practice, remove limitations, and align with existing DEArequirementsARM 24.174.835Continuing Education Requirements–– Removed requirement to submit copy to Board office; must be available upon inspectionARM 24.174.524Aligns with Department standardsARM 24.174.507Repeal unnecessary and duplicative rules to align with rule changes and theDepartment11
2/27/2020Board Rulemaking MAR 72Final Rule MAR Notice No. 24-174-72Effective December 7, 2019 Administration of Vaccines by Pharmacists––––– Aligns with legislative changes to 37-7-105, MCA, pursuant to HB 231Age 7 and older per CDC guidelines and collaborative practice agreementUpdated information about patient, product, pharmacist, and pharmacy to be maintained inpatient recordRemoved language duplicative to statuteARM 24.174.503MPDR Fee––––Aligns with legislative changes to 37-7-1511, MCA, pursuant to SB 61All licensees authorized under Title 37, MCA, to prescribe or dispense prescription drugs arerequired to pay the MPDR feeFee continues to be collected at time of license renewalARM 24.174.1712Board Rulemaking MAR 73New Rule MAR Notice No. 24-174-73Effective January 18, 2020 Positive Identification for Controlled Substance Prescriptions–Implements provisions of 37-7-410, MCA, pursuant to HB 86–Requires positive identification of recipient of controlled substance prescription,with exceptions, and documentation–Authorized identification in statute: Valid driver’s license; a school district/postsecondary photo ID; tribal photo ID–Authorized identification in rule: Valid government-issued photo ID, including but not limited to passport, military, orstate-issued ID–Current reference: ARM 24.174.842 as identified in MAR Notice No. 24-174-73 Effective but not yet updated in rules listed online12
2/27/2020Future TopicsNext Proposed Rule Continuing education programs: remove Board from pre-approval of non-ACPEprograms; revise requirements and audit information Prescription transfer: add reference to quantity remaining Device license type: new non-pharmacy license for device/DME/medical gas supplierto separate from other facilities; allow for person-in-charge Drug kits: combine contingency/emergency drug kits into one ruleFuture Rule Topics Wholesale drug distributors, third-party logistics providers, repackagers, andmanufacturers Facility general requirements Facility endorsements for compounding, outsourcing facility, and others Compounding information and references Collaborative practice, inspections, documentation/record keeping, limited servicepharmacy, and othersCurrent Subcommittee Rule Discussions Automated Dispensing Systems/Machines TechniciansQuestionWhat are the 2019 legislative topics related to the MontanaPrescription Drug Registry (MPDR)?A. FundingB. Integration into electronic workflow systems in medical andpharmacy practicesC. Mandatory registrationD. Mandatory use by prescribers of opioids or benzodiazepineseffective July 2021E. All of the above13
2/27/2020QuestionWhat are the 2019 legislative topics related to the MontanaPrescription Drug Registry (MPDR)?A. FundingB. Integration into electronic workflow systems in medical andpharmacy practicesC. Mandatory registrationD. Mandatory use by prescribers of opioids or benzodiazepineseffective July 2021E. All of the aboveTHANK YOU14
2/27/20202019 USP Sterile CompoundingChapter 797 OverviewJOHN DOUGLAS, RPhBOARD INSPECTORMONTANA BOARD OF PHARMACYCertification in Sterile Compounding for Inspectors (CISCI)March 1, 2020Recent Drug Developments and Law Update 2020University of Montana Skaggs School of PharmacyUnited StatesPharmacopeia(USP) General Chapter 795 Pharmaceutical Compounding—Nonsterile Preparations General Chapter 797 PharmaceuticalCompounding – Sterile Preparations General Chapter 800 HazardousDrugs—Handling in Healthcare Settings General Chapter 825 Radiopharmaceuticals— Preparation,Compounding, Dispensing, andRepackaging1
2/27/2020Reference: www.usp.org www.usp.org/compounding/general-chapter-797USP TimelineGeneralChapter 797 PharmaceuticalCompounding2019 Revisions Public comment period July 27, 2018through November 30, 2018 Open microphone session September 5,2018 Intended publication date June 1, 2019 Intended official date of December 1,20192
2/27/2020Important USP Updates: June 1, 2019 – Publication date of revised Chapter 797 (last revised 2008) September 23, 2019 – Revised Chapter 797 postponed until further noticePer USP: “The currently official version of General Chapter 797 (last revised2008) remains official until further hapter-7972019 USP 797 Overview:Sections1. Introduction and Scope2. Personnel Qualifications—Training,Evaluation, and Requalification3. Personal Hygiene and Garbing4. Facilities and Engineering Controls5. Microbiological Air and Surface Monitoring6. Cleaning and Disinfecting CompoundingAreas7. Equipment, Supplies, and Components8. Sterilization and Depyrogenation3
2/27/20209.2019 USP 797 Overview:Sections10.11.12.13.14.15.16.17.18.USP 797 Section 1.Introductionand ScopeSOPs and Master Formulation and CompoundingRecordsRelease TestingLabelingEstablishing Beyond-Use DatesUse of Conventionally Manufactured ProductsUse of CSPs As ComponentsQuality Assurance and Quality ControlCSP Storage, Handling, Packaging, Shipping, AndTransportDocumentationCompounding Allergenic ExtractsThis chapter describes the minimumstandards to be followed when preparingcompounded sterile human and animaldrugs based on current scientificinformation and best practices for sterilecompounding.4
2/27/2020Sterile Compounding is the process of combining,admixing, diluting, pooling, reconstituting,repackaging, or otherwise altering a drug or bulk drugsubstance to create a sterile medication.USP 797 Section 1.Introductionand ScopePreparing a conventionally manufactured sterileproduct in accordance with the directions containedin approved labeling provided by the product’smanufacturer is not compounding as long as theproduct is prepared for an individual patient andfollows the provisions for administration.Administration means the direct and immediateapplication of a conventionally manufactured productor CSP to a patient. It is out of the scope of this chapter Reconstitution: The process of adding a diluent to a solidconventionally manufactured product to prepare a sterilesolution or suspension.USP 797 Section 1.Introductionand Scope Repackaging: The act of removing a sterile product orpreparation from its original primary container and placing itinto another primary container, usually of smaller sizewithout further manipulation. Proprietary bag and vial systems (e.g., ADD-Vantage, MiniBag plus, addEASE):– Docking and activation in accordance with themanufacturer’s instructions for immediateadministration to an individual patient is notconsidered compounding.Docking for future activation and administration isconsidered compounding.5
2/27/2020Category is based on the conditions under which CSPs aremade, the probability for microbial growth, and the time periodwithin which they must be used.USP 797 Section 1.Introductionand ScopeCategory 1: All PECs may be placed in an unclassified segregatedcompounding area (SCA) Beyond use date (BUD):– Controlled room temperature: 12 hours– Refrigerated: 24 hoursCategory 2: PECs (LAFS and RABS) must be placed in an ISO 7 positivepressure buffer room with an ISO 8 positive pressure anteroom. BUD:– Controlled room temperature: 12 hours– Refrigerated 24 hoursPersonnel Qualifications:USP 797 Section 2.PersonnelQualificationsTraining,Evaluation, andRequalification Visual observation of hand hygiene and garbing: every 6months Gloved fingertip and thumb sampling: every 6 months,after media fill test Media fill testing: every 6 monthsCore Competencies 12 months (written and hands-onproficiency): Cleaning and disinfection Calculations, measuring, and mixing Aseptic technique Achieving and/or maintaining sterility and apyrogenicity Use of equipment Documentation of the compounding process (e.g.,master formulation and compounding records) Principles of HEPA-filtered unidirectional airflow withinthe ISO Class 5 area Proper use of PECs Principles of movement of materials and personnelwithin the compounding area6
2/27/2020Gloved fingertip and thumb sampling:USP 797 Section 2.PersonnelQualificationsTraining,Evaluation, andRequalificationDirect touch contamination is the most likely source ofmicroorganisms. Initial gloved fingertip and thumb sampling – before beingallowed to compound.– Evaluates a compounder’s competency in correctlyperforming hand hygiene and garbing.– No fewer than 3 separate times.– Must be performed on donned sterile gloves in the ISO 7buffer room or SCA.– Action level 1cfu (colony forming units) on both hands. Then every 6 months after completing the media-fill test.– Must be performed on donned sterile gloves inside of anISO 5 PEC.– Action level 3 cfu (colony forming units) on both hands.Before entering a compounding area, at aminimum, individuals must: Remove personal outer garments.USP 797 Section 3.PersonalHygiene andGarbing Remove all cosmetics. Remove all hand, wrist, and other exposedjewelry including piercings that could interferewith the effectiveness of garbing. Not wear ear buds or headphones. Not bring electronic devices that are notnecessary for compounding or other requiredtasks into the compounding area. Keep nails clean and neatly trimmed to minimizeparticle shedding and avoid glove punctures.Nail polish, artificial nails, and extenders mustnot be worn.7
2/27/2020Hand Hygiene:USP 797 Section 3.PersonalHygiene andGarbing Must be performed before entering acompounding area Alcohol hand sanitizers alone are notsufficient Brushes must not be used for hand hygiene(potential skin irritation) Hand driers must not be used (airturbulence and contamination) Perform after donning shoe covers, headand facial hair covers, and a face mask. The order of garbing must be determined bythe facility After hands are washed and dried, donremaining garb except sterile gloves, andthen perform hand antisepsis using analcohol-based hand rub with persistentantimicrobial activity immediately beforedonning sterile gloves.To enter a buffer room or SCA must be properlygarbed.USP 797 Section 3.PersonalHygiene andGarbingGarbing Requirements: Gown (non-cotton, low-lint, sleeves thatsnugly fit, enclosed at the neck) Disposable covers for shoes (low-lint) Disposable covers for head and facial hair(low-lint) Face mask Sterile gloves (powder free) If using RABS (CAI or CACI) disposablegloves (either nonsterile or sterile) inside ofgauntlet gloves, and sterile gloves overgauntlet gloves.8
2/27/2020Cleanroom Suite:USP 797 Section 4.Facilities andEngineeringControls All surfaces must be smooth, non-shedding,resistant to damage. HEPA filters must be located in the ceiling of thebuffer and ante-rooms. Returns must be low on the wall. Pressure –differential monitoring systems mustcontinuously monitor the pressure differentials. Aminimum differential positive pressure of 0.02-inchwater column is required between each ISOclassified area. Line of demarcation in the ante-room. No tacky surfaces. Access doors should be hands-free. Sink may be placed inside or outside of ante-room. Buffer room must not contain water sources. Microbiological incubator (if used) must be placedoutside of the classified areas. Temperature of 20 (68 F) or cooler and a relativehumidity below 60%.SCA:USP 797 Section 4.Facilities andEngineeringControls All surfaces must be smooth, non-shedding,resistant to damage. Must be located away from:– Unsealed windows, doors that connect tothe outdoors, and traffic flow.– Environmental control challenges(restrooms, warehouses, cafeterias, etc.) A visible perimeter must establish theboundaries. Sink at least 1 meter from the PEC, outside ofthe perimeter.9
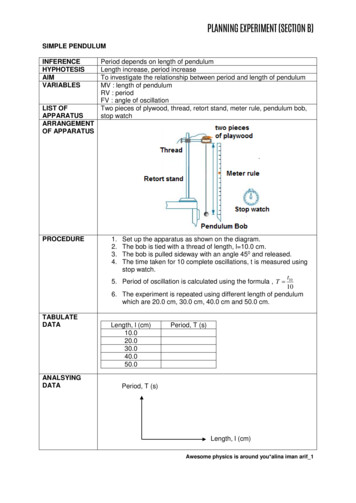
2/27/2020PECs:USP 797 Section 4.Facilities andEngineeringControls Placement must allow for cleaning around allPECs. Smoke pattern test (under dynamic operatingconditions) must be performed initially and every6 months. LAFS (Laminar Airflow Systems) -must be locatedout of traffic patters and away from room aircurrents that could disrupt airflow patter insidethe PEC. RABS (Restricted – Access Barrier System) (CAIand CACI) – the recovery time after opening toachieve ISO 5 air must be documented andfollowed.USP 797 Section 4.Facilities andEngineeringControlsAdded clarifications on Air Exchange RequirementsCompounding AreaUnclassified SCAISO Class 7 room(s)ISO Class 8 room(s)ACPH RequirementNo requirement 30 ACPH (at least 15 from HVAC) 20 ACPH10
2/27/2020Certification: During dynamic operating conditions Required every 6 monthsUSP 797 Section 4.Facilities andEngineeringControlsCertification needs to include: Airflow testing (air velocity/volume, ACPH (fromHVAC/PEC) HEPA filter integrity testing (PEC and SEC) Total particle count testing (all classified areas) Smoke visualization studiesRecertification: When changes to the area such as redesign,construction, or replacement or relocation of any PEC, oralteration in the configuration of the room that couldaffect airflow or air quality.Microbiological Air and Surface Monitoring:USP 797 Section 5.MicrobiologicalAir and SurfaceMonitoring Under dynamic operating conditions Viable air sampling (each classified area):– Initially and Every 6 months Surface sampling (each classified area):– Initially and MonthlyAnd when: New facility and equipment certification After any servicing of facilities or equipment Identified problems/trends11
2/27/2020https://www.usp.org/USP 797 Section 6.Cleaning andDisinfectingCompounding Areas Must be performed by trained andappropriately garbed personnel usingfacility-approved agents and procedures,which must be described in written SOPs. Minimum Contact Time -themanufacturer’s directions or publisheddata for the minimum contact time mustbe followed for the cleaning, disinfecting,and sporicidal agents used. 70 % IPA (Isopropyl Alcohol) must besterile.12
2/27/2020USP 797 Section 6.Cleaning andDisinfectingCompounding AreasUSP 797 Section 6.Cleaning andDisinfectingCompounding AreasTable 8 of the proposed revisedchapter provides the details theminimum frequency for cleaning anddisinfecting surfaces and applysporicidals in classified areas withinthe perimeter of the SCA.Cleaning Supplies(e.g., wipers, sponges, mop heads) Must be low-linting Should be disposable If reusable must be made ofcleanable material and cleanedbefore and after each use. Must be dedicated for use in theclassified areas or SCA, and mustnot be removed except for disposal.13
2/27/2020USP 797 Section 7.Equipment,Supplies, andComponentsUSP 797 Section 7.Equipment,Supplies, andComponentsRestricted-access barrier system (RABS): enclosurethat provides HEPA-filtered ISO Class 5 unidirectionalair that allows for the ingress and/or egress ofmaterials through defined openings that have beendesigned and validated to preclude the transfer ofcontamination, and that generally are not to be openedduring operations. Examples of RABS include CAIs andCACIs.Compounding aseptic containment isolator (CACI): Atype of RABS that uses HEPA filtration to provide anISO Class 5 unidirectional air environment designed forthe compounding of sterile HDs.Compounding aseptic isolator (CAI): A type of RABSthat uses HEPA filtration to provide an ISO Class 5unidirectional air environment designed forcompounding of sterile non-HDs.Components: Any ingredient used in the compounding ofa preparation, including any active ingredient, addedsubstance, and the container–closure system used topackage the preparation. Conventionally manufactured sterile products shouldbe used when available and appropriate for theintended CSP. Facility must establish the identity, strength, purity,and quality of the ingredients obtained. Each lot of commercially available sterile,depyrogenated containers and container–closuresystems must be accompanied by a COA . Any ingredient lacking an expiration date shall not toexceed 1 year after receipt by the compoundingfacility. Date of receipt must be clearly marked. Must be evaluated when received and before use.14
2/27/2020API (Active Pharmaceutical Ingredient):USP 797 Section 7.Equipment,Supplies, andComponents Must be obtained from an FDA-registeredfacility Must comply with USP-NF monograph if oneexists. Must be accompanied by a COA:– Includes the specifications and testresults and shows the API meets thespecifications of the USPNF monograph,if one exists.Sterilization MethodsAseptic Preparation USP 797 Section 8.Sterilization andDepyrogenation Compounding with only sterileingredientsSterilization by filtration (not for asuspension)Terminal Sterilization is preferred, unlessthe CSP or container cannot tolerate (canachieve Sterility Assurance Level of 10-6 ). Dry heat Steam autoclaving (not if moisture,pressure or temp would degrade CSP) Irradiation15
2/27/2020USP 797 Section 9.SOPs and MasterFormulation andCompoundingRecordsFacilities that prepare CSPs, mustdevelop SOPsUSP 797 Section 9.SOPs and MasterFormulation andCompoundingRecordsCompounding Record requiredfor all CSPs Must be reviewed every 12 months Any revisions must be communicated to allpersonnel Master Formulation Record; required if:– CSP prepared in a batch for 1patient– CSPs prepared from nonsterileingredient(s) May be in the form of prescriptionor medication order,compounding log, or label May be stored electronically(must be retrievable)16
2/27/2020Visual Inspection required at thecompletion of compounding andbefore releaseUSP 797 Section 10.Release Testing Check the physical appearance Check that the CSP, its label andthe prescription match Container closure integrity(leakage, cracks, etc.)Sterility Testing (CAT 2 as required)Bacterial Endotoxin TestingUSP 797 Section 10.Release TestingExcludes: Inhalations Topical ophthalmicsRequired for Category 2 CSPs: If made from one or more nonsterileingredient(s) or component(s) AND if assigned a BUD that requiressterility testing17
2/27/2020Label: A display of written, printed, or graphic matter on theimmediate container of any article.Labeling: All labels and other written, printed, or graphic matterthat are 1) on any article or any of its containers or wrappers, or2) accompanying such an article.USP 797 Section 11.LabelingThe label on the immediate container of the CSP must, at aminimum, display prominently and legibly the followinginformation: Assigned internal identification number (e.g., prescription,order, or lot number) Active ingredient(s) and their amounts, activities, orconcentrations Storage conditions if other than controlled room temperature Date prepared BUD Indication that the preparation is compoundedThe label on the immediate container of the CSP mustadditionally display prominently the followinginformation: Route of administration if it is not obvious from thecontainer, or when necessary for the safe use of the CSP.USP 797 Section 11.Labeling Total amount or volume if it is not obvious from thecontainer. If it is a multiple-dose container, a statement stating such. Contact information of the compounding facility if the CSPis to be sent outside of the facility in which it wascompounded. The labeling of the CSP must provide any applicablespecial handling instructions or warning statements.18
2/27/2020USP 797 Section 12.Establis
Board of Pharmacy Members Tony King, Pharmacist, President Starla Blank , Pharmacist, Vice-President Marian Jensen , Public Member, Secretary Courtney Bahny , Certified Pharmacy Technician Mike Bertagnolli , Pharmacist Paul Brand , Pharmacist Charmell Owens , Public Member General Email: dlibsdpha@mt.gov Website: www.pharmacy.mt.gov Phone: 406 .