Transcription
Evaluation of Pinnacle Auto-Planning forProstate VMATN. Simpson, G. Simpson, R. Laney, A. Thomson, D. Wheatley,R. Ellis, J. Mcgrane.Medical PhysicsRoyal Cornwall Hospital,Truro, CornwallUnited Kingdomnormasimpson@nhs.net
BackgroundPlymouth 95 miles.Exeter 120 miles.
Background VMAT 50% workload per month Regional service Catchment population is 450,000Variability in workload Interest in automation: Increase efficiencyStreamline standardized techniques More time for planning complex non-standardtechniques
BackgroundVMAT Planning RCHT 2015/2016
Background AutoPlanning is an integrated IMRT/VMAT module in the PhilipsPinnacleTM 9.10. UserAP Createdmimics the workflowexperiencedTechnique:skilled planner:Treatmentofan Beams Arrangement &Machine APuses Parametersclinical goals to formulateoptimisation objectives Clinical optimisationgoals for PTV coverage Multipleloops iterativelyand doseoptimisationlimits forreformulateand (OARs).adjust the optimisationorgans at risksobjectives to meet the criteria definedin the template. Global Settings prioritize sparing ofserial organsover Output:Clinicallydeliverable PlanKrayenbueh et al (2015) Evaluation of an automated knowledgetargets, dose fall-off,based treatment planning system for head and neck, Radiat Oncol.max doseKrayenbueh etal (2015)Evaluationof an automated knowledge based treatmentNov10;10:226)planning system for head and neck, Radiat Oncol. Nov 10;10:226)
MethodsPRESCRIPTION74Gy in 37# to PTV2(Prostate), with an SIB of66.6Gy in 37# to PTV1(Prostate SV)PTV1 (74Gy) Prostate 0.5cmmargin.PTV2 (66.6Gy) Prostate baseor full seminal vesicles plus 1.0cmmarginsSIB Rx 37 fractionsVMATSingle 6MV Arc (356 arcs (178 182 )3o SpacingDose resolution - 0.250cmIGRTCBCT fractions 1-4, then weeklyPLANNING TIMEVMAT PlanningExperiencePlanning Time(Mins)Experienced240Less Experienced360
ObjectivesTo evaluate the feasibility of automated single arcVMAT treatment planning for prostate cancer patientsusing a Pinnacle Auto-Planning ModuleTMTask Based Approach :1. Does AP produced plans meet the Institution Plan DVHProtocol?2.Are generated AP plans comparable to existing manuallyplanned VMAT protocol ?3.Clinicians Evaluation (a) Institutional Criteria (b) Preference4.Comparison of planning time differences.
Study DesignRetrospective Planning Study10 patientsAdenocarcinoma ProstateAge Range: 58-79Gleason Score: 7-9Routine(OAR overlaps withinprotocol)N 6Complex(OAR overlapsexceed protocol)N 4Apply AP Technique10 patientsComparisonD98, D2, CI, HI, OARBlinded Clinician StudyPlanning Time
MethodsInstitutional ProtocolPTV1PTV1 PTV2PTV2OARRectumD(Gy)VolMin DVH(%)63.398Max DVH(%)75.52Mean Dose66.6 - 71Max DVH(%)772Min DVH(%)70.398Mean DoseMax DVH(%)ProtocolCHHIPAP Technique73.3 - 74.7772D(Gy)max 5% AP Technique run on all plans.BladderCHHIP745%- One optimisation simultaneously.-BowelFemoral HeadPIVOTALCHHIP4578cc5017cc5514cc601cc*650cc5050% Time taken 40 minutes.
Results – Summary AP could produce a comparable clinicallydeliverable plan in all 10 cases. 6 routine plans met institution constraints 4 complex plans did not meet institution constraints due tooverlaps but were comparable to M-VMAT plans 2.4 x Planning Time Saving 240 mins to 100 mins /plan Clinician Blind Evaluation AP produced 100% clinically acceptable plans Difficult to distinguish between plan types Slight preference to M-VMAT plans on routine cases, AP forcomplex cases
ResultsPTV Coverage – No difference in PTV coveragebetween AP & M- VMAT plansInverse PlannedData-PointMeanS.DAuto PlannedMeanS.DSig.PTV1Min DVH(%)98.70.49498.60.6420.507Max DVH(%)0.0750.1920.0960.1000.784PTV1 PTV2Mean Dose68.690.32067.830.7610.507Max0000-PTV2Min DVH(%)99.950.05699.970.0420.277Mean Dose73.650.37273.840.1040.152Max DVH(%)0000-
ResultsPTV HI/CI – No difference in plan qualitybetween AP & M- VMAT plansInverse PlannedData-PointMeanS.DAuto V1CI1.3280.133PTV1 0400.0341.0680.0640.30
ResultsRectum Constraints – AP Met all constraints in a singlerun. Slightly higher V74Gy when compared within M-VMATD(Gy)Inverse PlannedData-PointMeanS.DMeanS.DSig.V30 80%47.899.61248.6513.070.236V40 70%35.648.09637.659.8220.501V50 60%27.336.75628.526.7120.475V60 50%19.475.31420.424.8290.282V65 30%14.634.45615.463.820.111V70 15%7.8712.8328.4352.4410.162V74 3%0.3630.5271.6340.8490.001**Auto PlannedStatistical significance achieved at the: 95% confidence interval (*)99% confidence interval (**)
ResultsBladder Constraints – AP Met all constraints in a single run.Slightly higher V74Gy when compared with M-VMATInverse PlannedAuto PlannedData-PointMeanS.DMeanS.DSig.V50 50%16.125.87815.645.9710.180V60 25%11.554.19511.304.2470.111V74 5%0.7350.8531.4200.6910.046*Statistical significance achieved at the: 95% confidence interval (*)99% confidence interval (**)
ResultsBowel Constraints – (Routine Cases N 6)AP Met all constraints in a single run. Slightly higher V74Gywhen compared with M-VMATInverse PlannedAuto PlannedData-PointMeanS.DMeanS.DSig.V45 78cc18.1111.9820.5113.550.95V50 17cc15.9811.2018.3512.540.76V55 14cc13.649.21115.9411.250.14V60 1cc11.407.9013.058.870.64V65 0cc7.045.749.706.710.23
ResultsBowel Constraints – (Complex Cases N 4)AP Met all constraints in a single run. Slightly higher V74Gywhen compared with M-VMATInverse PlannedAuto PlannedData-PointMeanS.DMeanS.DSig.V45 78cc18.1111.9720.513.550.095V50 17cc15.9811.2018.3512.540.076V55 14cc13.689.2115.9411.250.144V60 1cc11.407.9013.058.870.064V65 0cc7.045.749.716.710.023*Statistical significance achieved at the: 95% confidence interval (*)99% confidence interval (**)
Results Bowel overlap with PTV PTV preference over OAR sparing
Results Is there a way to improve the plans where thereis a large bowel overlap? Develop another Technique? Refine the current Technique? Interact with the plan at the optimiser level?
Results: Bowel OverlapAuto Planning Run AP Check overlaps, add DVH point at D60 &D65 points Re-Run the techniqueAuto Assisted Planning Run AP Modify PTV (minus OAR overlap) Constraint on OAR overlap in the Optimiser Warm Start Reduced PTVcoverage at D98and D95(shoulder) Reduced highdose tail andmaintainedcoverage at D98and D95 Increasedplanning time 40mins
Results: Bowel OverlapBowel Constraints - (Complex Cases N 4)No change to PTV D98/D95 but significant reduction in V65GyBowelInverse PlannedAuto PlannedData-PointMeanS.DMeanS.DSig.V45 78cc18.1111.9719.6812.490.106V50 17cc15.9811.2017.4611.600.051V55 14cc13.689.2114.569.740.09V60 1cc11.407.9011.948.620.24V65 0cc7.045.744.215.210.043*Statistical significance achieved at the: 95% confidence interval (*)99% confidence interval (**)
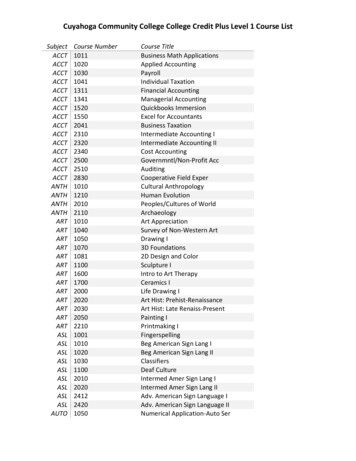
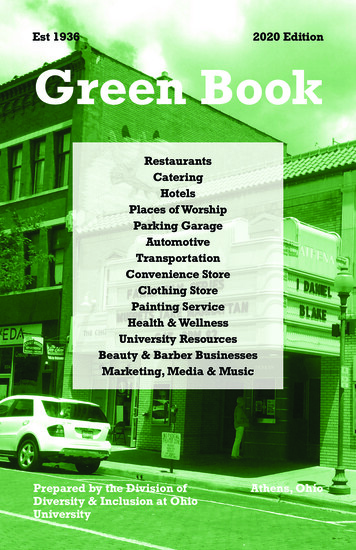
Results: Meet Institutional Protocol ? For all 10 plans clinicians scored AP as meeting InstitutionalProtocol in Blinded Study 100% would treat with AP Plans if not given a choiceConsultant Blind Evaluation12Case Number108DAW6RAEJMG4AHT20IPAPPlan Type
Results: Plan Preference AP. Vs. M-VMAT Plan Preference –Given a choice - preference towardsM-VMAT plans due to the slightly lower tail DVH for allOARsConsultant Blind Evaluation109Case Number876DAW5RAE4JMG3AHT210IPAPPlan Type
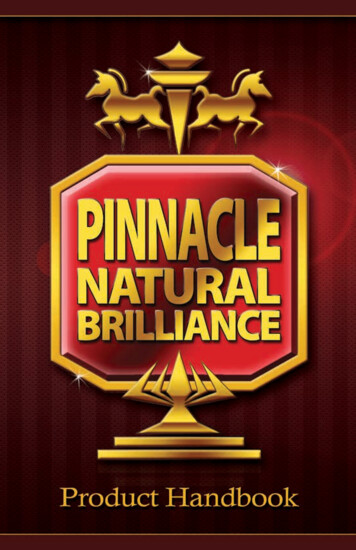
Results: Plan Preference AP. Vs. M-VMAT Plan Preference –Given a choice - preference towardsAP plans due to the slight lower tail DVH tail of Bowelin M-VMAT3.5Consultant Blind EvaluationBowel Overlap Cases3Number of Cases2.52DAW1.5RAEJMGAHT10.50IPAPPlan TypeEither
Results Planning time savings Experienced Planner 2.4 x time saving Less Experienced Planner 3.3 x time savingVMAT PlanningExperiencePlanning Time (Mins)(Manual VMAT)Planning Time (Mins)(Auto Planning)Planning Time(Mins)(Auto AssistedPlanning)Experienced24060100Less Experienced36070110
Conclusions AP produces highly consistent treatment plans with asingle treatment technique for both routine andcomplex prostate cases. Dose distributions of the target volumes were similarbetween the AP and M-VMAT OAR sparing was comparable using AP across theDVH curve but slightly increased on the tail.
Conclusions Planning time was substantially reduced with AP. Technique can be used by both experienced and lessexperienced planners. Clinicians would accept either plan but due to DVH tailon all OARs preferred Manually manipulated plans,whether this be the M-VMAT or the auto assisted.
Future Work Used Mean Doses for OAR Technique. Refine technique: Add DVH points to shape high dose tail How much further can be OARs be pushed? Assess Auto planning for other clinical sites
AcknowledgmentsCo-Authors:Mr G SimpsonMr R LaneyDr J McGraneDr D WheatleyDr R EllisDr A ThomsonWith thanks to:Philips: Greg Perkins and Nigel DeshpandeElaine BuckClaire CartledgeMarina Cousins
Evaluation of Pinnacle Auto-Planning for . Auto Assisted Planning Run AP Modify PTV (minus OAR overlap) Constraint on OAR overlap in the Optimiser Warm Start . Inverse Planned Auto Planned Data-Point Mean S.D Mean S.D Sig. V45 78cc 18.11 11.97 19.68 12.49 0.106