Transcription
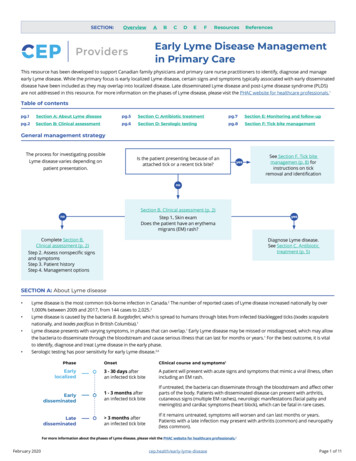
Restorative DentistryTooth wear: Attrition, erosion, and abrasionLuis A, Litonjua, DMDVSebastiano Andreana, DDS, MS /Peter J. Bush, BS /Robert E, Cohen, DDS, PhD"Attrition, erosion, and abrasion rGsult in alterations to the tooth and manifest as tooth wear. Each ciassitication acts through a distinct process that is associated with unique clinical characteristics. Accurateprevalence data for each classification are not auaiiabie since indices do not necessarily measure onespecific etiology, or the study populations may be too diverse in age and characteristics. The treatment ofteeth in each classification will depend on identifying the factors associated with each etioiogy. Somecases may require specific restorative procedures, while others wili not require treatment. A review of theliterature points to fhe interaction of the three entities in the initiation and progression of lesions that mayact synchronously or sequentiaiiy, synergisficaliy or additiveiy, or in conjunction with other entities to maskthe true nature of tootti wear, which appears to be mulfifacfcriai. (Quintessence int 2003:34:435 46)Key words: abrasion, attrition, cervicai abrasion, dentifrice, erosion, toothbrush abrasion, tooth surfaceloss, tooth weaross of tooth structure may occur through noncarious processes. Regressive alterations may vary inetiology, extent, and clinical presentation among individuals and may be associated with physiologic orpathologic processes. Traditionally, those entities havebeen classified as attrition, erosion, and abrasion (Figs1 to 3), Attrition is defined as the physiologic loss oftooth structure as a result of the masticatory processes; erosion is the chemical dissolution of structurethat does not involve the carious process; and abrasion is the mechanical wearing away of structure,Eccles' suggested that the term tooth surface iossbe used to encompass all those descriptions hecause asingle etiologic factor is usually difficult to identify.Later, Smith and Knight- proposed the term toothL'Periodontics Resident, Department ol Penodontics and Endodontics,Stale University of New York at Butlalo, Buffalo. New York. Clinicai Assistant Professor, Department of Periodontics and Endodortcs,State University of New York at Buffaio, Buffalo, New York, Director, South Campus Instrumentation Center, State University of NewYork at Buffaio. Buffalo. New York."Professor, Department of Peiiodontics and Endodontics, State Universityof New York at Buffaio, Buffalo, New York.Reprint requesls; Dr Luis A, Litonjua, Department of Periodontics andEndodontios, State University of New York a( Buffaio. 250 Squire Hail, 3435fularn Street, Buffaio, NY 14214-3008. E-maii: laldmd yahoo comQuintessence internationalwear to embrace all those conditions and their combinations whether or not the etiology is known. Theycontended that the term tooth surface loss did not adequately reflect the severity of the condition and advocated the use of the term tooth wear.-'ATTRITIONThe term attrition is derived from the Latin verb attritum which describes the action of rubbing againstsomething, Dental attrition is defined as the physiologic wearing of teeth resulting from tooth to toothcontact as in mastication, '' This is an age-relatedprocess that can occur at the incisai or occlusal surfaces and sometimes on the proximal surfaces.Clinically, the first manifestation is the appearance ofa small polished facet on a cusp tip or ridge or an incisal edge. Severe attrition may lead to dentinal exposure, which may increase the rate of wear,''' -"Tooth wear occurs at an ultrastructural level andcan be caused by direct contact between surfaces orthe action of an intervening slurry.' Attrition may behastened by a coarse diet and abrasive dust. ' " " Dahlet al'' found high levels of inorganic compounds andsalts in snuff while Bowles et al** found silica particlesto be abrasive in tobacco chewing. However, some audisagree with this classification of attrition435
Litonjua et aiFig 1 Severe attrition on mandibular incisors and oanines as aresult of bruxism.Fig 3 Abrasion aL buccal surfaoes of premola.'s. Patient reporteda history of incorrect and excessive toothbrushing.where an intervening bolus of food is invoived.Instead, they use the tenn demastication to describethe wearing away of tooth substance during mastication of food influenced by the ahrasiveness of the individual food particles.Some paraftinctionai habits (bruxism and clenching) may also contribute to attrition.*"' While theprevalence of bruxism is unclear, studies report between 5% to 96% of the population may be affected.*In contrast, Seligman et al'* reported that the prevalence of dental attrition was not associated with thepresence or absence of temporomandibular jointsyrnptomatology. While a certain amount of attrition isphysiologic, excessive destruction of tooth structure isnot physiologic.RusselF distinguished physiologic and normal frompathologic and abnormal attrition. He contended thatocclusal wear that renders itself vulnerable even tonormai functional loading cannot be regarded as normal. In addition, if occlusal wear occurs at a ratefaster than compensatory physiologic mechanisms.436Fig 2 Erosion at palatal and occlurai iurlacfcs a i a result olchronic vomiting.this is not physiologic. He also reported that labelingof tooth wear must be viewed in the context of thecultural environment under which it has occurred.Epidemiologie surveys on the prevalence of attrition have been reported as tooth wear or tooth surfaceloss. The exact prevalence of tooth wear or tooth surface loss is unclear, primarily due to different assessment criteria, but has been reported to range from13% to 98%.'""" One problem of tooth wear surveysis the definition of the condition and parameter ofmeasure. Thus, reports are confusing and incomparable because some researchers have reported erosionand attrition singly, or together as tooth wear. Furthermore, the use of different indices with differentcriteria adds to the confusion reported in the NorthAmerican and the European literature. NorthAmerican literature has concentrated more on attrition rather than on erosion, while European literaturehas reported that the most common and destructivecause of tooth wear is erosion. Tables 1 to 4 are examples of different criteria or indices.The studies of measurement of rate, pattern, anddegree of tooth wear are numerous, but it was Broca's1879 method that initially divided wear into degrees. Recent authors have patterned their subjective scoringmethod after Broca, and depend primarily on theamount of exposed dentin on the occlusal table to derive their methodology. Subsequent methods have utilized photographic and planimetric methods to address quantitative criteria. A more recent method byMayhall and Kageyama * combined three-dimensionaland digital imagery for describing molar wear.The value of tooth wear surveys comes into question when one wants to know the progress of attrition,since the data is a cumulative record. It is here wherelongitudinal studies play a vital role in describing thedisease process. Unfortunately, these studies are rarelargely because wear occurs slowly.' ' ' Vertical loss ofVoiume 34, Number 6, 2003
Litoniua et alTABLE 1An attrition index '0 No wear1 Minimal wear2 Noticeable flattening parallel to the occluding planes3 Flattening of cusps ot grooves4 Total loss of contour and/or dentin exposure when identiliableTABLE 2Ciass 1Class IIClass IIIModiflea from Richaids and Biown. enamel rarely exceeds 50 pm/year'' with one report at68 pm/year.-* One should bear in mind that the occurrence and pattern of tooth wear is likely related to educational, cultural, dietary, occupational, and geographic factors in the population studied.* Otherimportant factors that should be added are age andthe function of occlusion.Dental attrition has been used in archeology and theforensic sciences to estimate human age. While thereare some measurement methods (see example on Table5) that have been suggested by authors, estimationshould be based upon several teeth or the entire dentition.'" Seligman and Pullinger' concluded that attritionhas a multifaetorial etiology with age and canine guidance having signlGcant influence (in addition to parafunction, including crowding, occlusal slides, crossbites,chewing habits, and diet). Controlled in vitro experiments show that enamel wear is affected by cbanges inlubricating conditiotis, acidity, and loads. ' In addition,enamel wear differs from dentin wear and progressiveincrease of dentin wear is associated witb increasingload." Finally, it should be noted that attrition is a continuing process. Newman," in his review, concludedthat teeth continue to erupt in adulthood even in the absence of masticatory function and concomitant attrition.Normal attrition requires no treatment since formation of secondary dentin and the eruption processkeep tbe wear process in balance. Where there is lossof posterior support, malocclusion, and bruxism. occlusal adjustment and splint therapy may be indicatedfor the remaining dentition."' The treatment of severeattrition where teeth are worn to the gingival marginmay require restoration of the vertical dimension toimprove function and esthetics. Treatment options include extraction of affected teeth and replacementwith conventional dentures, overdentures, overlayprosthesis, amalgam or composite buildups, and fixedor removable prostheses.' EROSIONThe term erosion is derived from the Latin verb erosum(to corrode) which describes the process of gradualQuintessence InternationalClassification of dental erosion 'Superficial lesions involving enamel only.oca 1 i zed lesions involving dentin for less than onethird ol ttie surfaceGeneralized lesions involving dentin for more than onethird ot the surfaces Facial surfaces Lingual and palatal surfaces Incisai and occlusal surtaces Severe multisurtace involvementTABLE 3Tooth wear in general with erosion as oneRatingOperational explanationSatisfactoryR (Romeo)S (Sierra)No visible wear or change in anatomic form.Limited (normal) wear. Limited change inanatomic to'mConsiderable wea; with obvicus change otanatomic form, but does not require treatmentM (Mike)Not acceptableT (Tango)Considerable wear with marked change manatomic torm. Further damage to the toothand/or its surrounding tissues is likely to occur.Excessive wear. Extreme change of anatomicV (Victor)form, esttiefics, and function. Pain on chewing.Damage to the tooth and/or its surrounding tissues occurs.Based or Ryge and Snydsr'' syslenTABLE 4Tooth Wear Index /0ICNo loss ot enamel surface characteristicsNo change of contourLoss of enamel surface characteristicsMinimal loss of contourLoss ot enamel exposing dentin tor less than onethird ot the surfaceLoss ot enamel ust exposing dentinDetect less than 1 mm deepLoss of enamel exposing denlin greater than onethird ot the surfaceLoss of enamel and substantial loss of dentin, butnot exposing pulp or secondary dentinDelect 1 to 2 mm deepComplete loss of enamel, or pulp exposure, or exposure ot secondary dentinPulp e5(posure or exposure ol secondary dentinDelect greater than 2 mm deep, or pulp exposure, orexposure of secondary dentinB bjccal or labial; L lingual or palatal, O occlusal; I incisai; C cer-437
Lilonjua et aiTABLE 5 Classification of point values of comparison to age changes inattrition, secondary dentin, periodontosis, cementum, and root résorption,according to degree of development An no attritionA, attrition withinenamelS„ no secondaryS - seoondarydentindentin has tiegunto form in upperpart ot puip cavityP(, no periodontcsis P, periodontosisjust beginningCQ normai iayerC, - apposition aof oementum iaidlittle greater thandownnormalR.j No tootRi Root resorptiorésorption visibleonly on smaflisoiated spotsdestruction of a surface, usually by a chemical or electrolytic process, Dental erosion is defined as the loss oftooth structure hy a nonhacterial chemical process, 'The soluhility of enamel is pH dependent, and the rateat which apatite precipitates depends on certain factors, such as calcium binding in saliva. Saliva containscalcium and phosphate ions and exists in a supersaturated state at neutral pH with respect to enamel hydroxi'apatite. As the pH of saliva decreases, it crossesthe saturation line at a point known as the critical pH.Since the critical pH of enamel is approximately 5.5,any solution with a lower pH may cause erosion, particularly if the attack is lengthy and intermittent overtime. Tbe inorganic dental matrix is demincralizcd byacid, which may originate from a diet including tbingssuch as fruit juices, from gastric acid in individuals experiencing bulimia, or from industrial acids in the workClinically, dental erosion is primarily a surface phenomenon, wbile earies originates as a suhsurfacedemineralization of enamel structure." Erosion generally presents as concave and rounded defects withoutthe roughness normally associated with caries. In earlystages, erosion affects enamel resulting in smooth,glazed surfaces lacking in developmental ridges andstain lines. The involved dentin may also show a polished surface while some teeth may have a dull mattedappearance.**" In advanced cases, restorations mayprojeet above occlusal surfaces and cusps of posteriorteeth {and incisai edges of anterior teeth) exhihitingconcavities known as cupping. Erosion associatedwith gastrointestinal reflux are evident as concave depressions on the palatal and oeclusal surfaces of maxillary teeth, as well as huccal and oeclusal surfaces ofmandibular posterior teeth, and have been termed perimolysis or perimylolysis ' Erosion associated withdiet may be evident on labial surfaces of maxillary anterior teeth and present as scooped-out depressions. "438Aj attrition reachingdentinSj - pulp cavity ishaiftiliedwith secondary dentinAj attrition reachingpuipS3 pulp cavity isnearly or wholiy fiiledwith secondary dentinPj periodontosis aiong P, periodontosis hastirst one third ot rootpassed two thirds of rootCj - Heavy layer ofCj great layer ofcementumcetnentumRj Greater iossofsubstanceRj Great areas ofboth oementum anddentin affeotedMannerberg ' described two types of erosive lesionsusing the scanning electron microscope (SEM). Theactive lesion shows distinctly etched enamel prisms resembling a honeycomb, while latent or inactive erosions are faint with unrecognizable characteristics.Further ultrastruetural studies have demonstrated irregular patterns of enamel dissolution. As the lesionprogresses to dentin, the first area to be affected isperituhular dentin. Dentinal tubules tben become enlarged, affecting intertubular areas as well. Rapidprocesses may lead to sensitive teeth, while slowerprogression may be asymptomatic."In 1995, a European workshop on dental erosionswas undertaken specifically to discuss current knowledge on etiology, mechanisms, and implications of thisproblem.'*' Among topics discussed was the etiologicclassification of erosion, which is one of four bases fornomenclature and classification of erosion (the otherthree are clinical severity, progression, and localization). Thus, etiologic classification of tooth erosionmay fall under extrinsic (exogenous), intrinsic (endogenous), or idiopathic (unknown). Extrinsic etiology of dental erosion can'further be subdivided intoenvironmental, diet, medication, and lifestyle,' thecharacteristics of which are summarized in Table 6.Environmental erosion occurs when individuals areexposed to acids in their work place or during leisureactivities, although bealth and safety laws have mostlikely reduced this risk.'" The process predominantlyaffects the labial surfaces of maxillary or mandibularincisors.' Surveys in industrial environments havedemonstrated that workers exposed to acid fumes andaerosols experience more dental erosion compared toacid-free department employees. Among groups studied were battery factory workers exposed to sulfuricacid, galvanizing factory workers exposed to hydrochloric acid, and workers in etching and cleaningprocesses involving those acids. Other occupationsVoiume 34, Number 6, 2003
Litonjua et aithat may increase the risk of dental erosion includemunitions manufacturing, commereial printing, andlaboratory workers. Some case reports have showncompetitive swimmers at gas-chlorinated pools suffering from dental erosion.' * One study« reported thatprofessional wine tasters had an associated increasedrisk of tooth erosion due to the frequent exposure towines with erosive potential (pH range of 3.0 to 3.6).Although the latter is an occupation, il is also relatedto diet-a factor that has received the most attention.The extrinsic etiology of diet has been extensively investigated, but the actual evidence linking a particularaeidie food or beverage as the primary agent is limited,Coliectively, however, the evidence strongly supportsthe role of acidic foods and beverages as a contributingfactor in dentai erosion,'* The erosive potential offoods and beverages are significantly associated withtheir acidity, pH, phosphate and fluoride contents, aswell as the baseline surface microhardness and iodidepermeability values of the exposed enamel, ' Amongthe foods and beverages implicated are citric acid,acidic and citrus fruits and their juices, carbonated softdrinks and diet drinks, sports drinks, and vinegar conserves,5«-"-'s Acidic foods and beverages have been implicated based on eiinical studies, animal studies, andin vitro investigations. Epidemiologic studies and clinical trials have provided the strongest evidence for therole of acidic foods and beverages. However, animalstudies are vulnerable to differences in physiologicmechanisms and properties between speeies. In vitro investigations may not address the differences in hard tissues, the role of saliva, and the roleof soft tissue and physiologic soft tissue movements,'* ' " ' !n vitro and in situ experiments havedemonstrated the protective role of saliva against mineral loss by erosion for enamel and dentin. This maybe attributed to the chemical composition of saliva,the quantity of saliva protecting the specimens, thepresence of organic layers covering the specimens,and the potential effect of fluoride in situ.'*'There also have been some reports associating medications and over-the-counter dental products withdental erosion. Those products have a low pH and,upon frequent and/or sustained contact with the dentition, will have a marked effect on dentai erosion.Among medications implicated are aspirin, vitamin C,and oral hygiene products with calcium cheiators.' Although acidic foods and beverages have thestrongest association with dental erosion, the quantityand frequency of how these arc ingested is modifiedby lifestyle and behavior factors,'' Dieting and the obsession for a healthier lifestyle may lead one to ingestmore fruits and diet drinks. The quest for beauty maylead to more frequent product use. Toothbrushing immediately after an acid attack has been shown to acQuintessence InternationaiTABLE 6 Nomenclature and classification ofe ros I on ä' 'EtiologyExtrinsic nLifestyleIntrinsic (endogenous)Idiopathic (unknown)Clinieal severity on tooth surfaceSuperficiaiLocalized lesionGeneraiized lesionPattiogenic activity ot progressionManitest or aetiwLatent or inactiveLoealization of erosion (perimolysis/perimylolysis)Paiatal and occlusai surface ot maxiilary teethBuccal ana oeelusal surface ot mandibular teethTABLE 7 Intrinsic factors associated with chronicvomiting or persistent gastroesophageal refiux 't. Alimentary tract disorders (peptic uleer, ehronic gastiitis, intestinal obstruction)2. Central nervous system disorders (encephalitis, neoplasms)3. Neuroiogic disorders (migraine, diabetic poly neu ropa thia)4. Metabolic and endoerme disorders (adrenal insufficiency, hyperthyroid crisis)5. Drug side-eftects (central emetic ettects, gastnc irntation)6. Psychosomatie disorders (stress-induced vomiting, eatingdisorders)celerate loss of tooth substance, and bleaching agentsmay increase susceptibility to acid erosion. ' In addition, two case reports cite the use of intraora! cocainein inducing dental erosion, "Dental erosion from intrinsic factors is causedmainly by gastric acid reaching the dentition and oralcavity frequently and consistently. This may be a resultof chronic vomiting, persistent gastroesophageal reflux,régurgitation, or rumination." Long-term, regular vomiting results in dental erosion and is caused by disordersof the alimentary tract, metabolic and endocrine disorders, as well as indirect drug side effects including theuse of alcohol,' "' However, in most cases the underlying cause of dental erosion and vomiting is due to a bulimic eating disorder. This affects mostly young womenwhere the prevalence of dental erosion is high,5i Othercommon disorders related to dental erosion are gastroesophageal reflux and régurgitation. Those arecaused by the incompetence of the gastroesophagealsphincter due to disease, drugs, increased intra-abdominal pressure, and intragastric volume '''-" (Table 7),439
Prevalence surveys are few in number, while case reports or small case series occupy most of the epidemiologic literature on dental erosion. It is also difficult tocompare prevalence studies because of different indicesand different sampled teeth. * There are many indicesfor the grading of erosion that have been formulatedand appiied in animal and human studies. Some ofthese describe very fine morphologic changes, whichare not ideal for epidemiologic data. ' Azzopardi et a Freviewed techniques to measure tooth wear and erosion. They concluded that in vitro tediniques may havelittle direct clinical relevance, but they may lead tonovel and accurate methods. Moreover, in vivo studiesmay have problems with reference points and accuratevalidation of the techniques.Another source of variation is the way in whichdamage to the teeth has been recorded, estimated, andreported. Some give general guidelines on case historyand clinical examination, whereas others define severity categories and classifications of erosion," In addition, the indices appear to measure only enamel lossand not the specific action of erosion or cause of theerosion. Identification of the prevalence per se is difficult because of the multifactorial etiology', which maycomplicate the situation in the population, " Nevertheless, depcndahie methods exist for the assessment oferosive potential of dental erosion, but the prospectiveuser would need to study the method and learn thespecialized techniques required.-- Azzopardi et aF concluded that there is need for a simple and reliabletechnique to quantify tooth wear due to erosion. Supporting this is a case-control study that reported prevalence of erosion at 5"* of a Finnish population. * 'Conversely, a review of epidemiologic studies of erosion reported that prevalence in children varied widelybetween 2 /o to 57%, probably due to a small number ofsubjects and different criteria for diagnosis, In contrast, a recent International Dental Federation (FDI) commission report' reviewed and analyzed the past data. It concluded that tooth enamelerosion is rare, easily misdiagnosed, and occurs onlyin susceptible individuals regardless of food and beverage consumption patterns. Therefore, consumption ofacidic food or beverage alone is highly unlikely tocause erosion. Moreover, susceptibility is highly variable from one individual to another, and erosion ismultifactorial in nature.The prevention of erosion can be attempted in twoways, specifically by weakening the erosive potentialof acid challenge and by increasing resistance of thedentition, ' Reducing the frequency of contact withacidic foods and beverages is the most effective advice.* ' * Referral to {and comanagement with) the patient's physician should be considered if erosion bygastric acid is suspected, -* Dietary advice and oral440therapy may be performed to increase the protectiveproperties of saliva and alter consumption of potentially harmful foods. These include the consumption ofacidic drinks quickly or through a straw, rather thansipped slowly; and the consumption of products withhigh content of calcium, phosphate, and buffering substances, such as milk and cheese. ' "* Additionally,other recommendations are prescription of buffercontaining chewing gum, oral health instructions toprevent further erosion, and fluoride therapy, '' Modification of food and beverage for content andacidity is theoretically possible but not feasible because of food regulatory constraints and consumer acceptance such as altered taste, ' It also has beenshown that calcium and phosphate salts added tofoods and beverages cause less enamel and dentindemineralization.sis« Aside from calcium and phosphate supplementation, other studies on food and beverage modification have explored other salts that varycalcium and phosphate levels; reduction of acidity levels and addition of calcium citrate malate to softdrinks; and the applications of fluoride, bicarbonates,and certain milk constituents.*''Restorative therapy includes glass ionomers, resincomposites, composite or porcelain veneers, andplacement of crowns and bridges. Sensitive teeth maybe treated with desensitizing agents and dentifrices.Unless the etiology of erosive lesions is eliminated,restorations that are abrasive to the antagonistic teeth,such as porcelain, should not be used. - ' ABRASIONAbrasion is derived from the Latin verb abrasum (toscrape off), which describes the wearing away of asubstance or structure through mechanical process, Dental abrasion is the pathologic wearing of teeth asa result of abnormal processes, hahit, or abrasivesubstance, "Forms of dental abrasion may be related to habit oroccupation, ''-" Notching of incisai edges may becaused by pipe smoking, nut and seed cracking, nailbiting, and hairpin biting. Carpenters, tailors, and musicians may exhibit similar notched teeth due to nails,tacks, and instrument mouthpieces, respectively. Thelocation and pattern of abrasion may be dependentupon the cause. " Proximal root abrasion may be dueto improper flossing and toothpicks. However, themost common cause of dental abrasion found at thecervical areas is toothbrushing, which may be related totechnique, zealous and vigorous methods, time and frequency, bristle design, and abrasive dentifrices, *''"'''This is termed toothbrush abrasion and has merited themost attention.Voiume 34, Number 6, 2003
Litonjua ei alBptdemiologic studies have dealt mainly with toothbrush abrasions, or cervical abrasions attributed totoothbrushing and interrelated factors. Unlike attritionand erosion, these are easier seen, classified, and identified. Historically, these lesions have been clinicallydescribed as wedge-shaped, dish-shaped, flattened irregular, and concave, and can be further characterizedaccording to depth and size." An SEM study by Bradyand Woody'- delineated morphology into two groups:angular and deep versus rounded and shallow.Bevenius et al" used microendoscopy and SEM to define two distinct forms {saucer and wedge-shaped) ofcervical lesions.The prevalence of toothbrush abrasions varies anywhere from 5% to 85%, depending on the populationstudied. Remarkably, there are reported conflicts onthe role of contributing factors, liitchin' divided 200individuals aged 20 to 59 into four age classes andfound 42% of tbe 20-to-29-year age group with abrasions, while the 40-to-49-ycar age group exhibited76 0 with abrasions. Deep lesions were found in theolder groups, and good oral hygiene was associatedwith frequency of abrasion, Radentz et al" found halfof the subjects aged 17 to 45 with cervical abrasionsrelated to dentifrice use. However, they found no relationship of the lesions to toothbrush technique andfrequency. Sangnes and Gjermo'* found 32% of theiryoungest age group and 50% of subjects over 30 yearswith at least one toolh with wedge-shaped defects.The higher prevalence of lesions was associated withhigher frequency of toothbrushing. Tbe tendency of lesions to appear on the left side of the mouth was attributed to having more right-handed people. Thesmaller number of left-handed subjects likewise presented with more lesions on the right side of themouth. Brady and Woody" found 5% of 900 dentistsshowing cervical lesions, with premolars exhibitingthe most frequency. Bergström and Lavstedt" found30% of 81S people with cervical abrasions (with 12%of those also demonstrating wedge-shaped and deepdepressions). Moreover, they concluded that horizontal brushing technique versus vertical roll and frequency (more than twice per day) had a strong correlation to abrasion, while brush stiffness and dentifriceabrasivity were weak. Hand et aP found 56% of an elderly population exbibited cervical abrasions, 30% ofwhich was described as greater than 1 mm deep.Premolars were more frequently affected, and dataanalysis implicated vigorous toothbrushing as themajor etiologic factor. Bergström and Eliasson' founda high occurrence rate of 85% in subjects aged 21 to60 years old. No significant differences were foundwith regard to tootbbrush technique, nor dentifriceswith different abrasivily. Furthermore, there was nosignificant difference between subjects using soft.Quintessence Internalionaimedium, or hard bristies to the presence of cervicalabrasions (Table 8).Altbough studies show a strong association of cervical abrasions to toothbrushing, some authors contend that dental erosion plays a role in this toothwear.-'-'." In experiments where teeth were subjectedto acid attacks and toothbrush abrasion, it was foundthat rate of abrasion resistance of eroded enamel continued with remineralization time. In addition,
ATTRITION The term attrition is derived from the Latin verb attri-tum which describes the action of rubbing against something, Dental attrition is defined as the physio-logic wearing of teeth resulting from tooth to tooth contact as in mastication, '' This is an age-related process that can occur at the incisai or occlusal sur-