Transcription
Systems Immunology in IO:A View from the Parker InstituteNikesh Kotecha, PhDVP, Informatics
Disclosures
OUR MISSIONTo accelerate the developmentof breakthrough immunetherapies to turn cancer into acurable disease.
A New Network7 ResearchInstitutions300 Nation’sTopResearchers60 Laboratories40 Industry& Non-profitPartnersPROJECT-BASEDCOLLABORATORSApril, 2016: Billionaire tech entrepreneur Sean Parkerannounced a 250 million donation to establish theParker Institute for Cancer Immunotherapy to speedresearch into innovative cancer treatments.Fortune Health
The Institute LeadershipInstitute LeadersANTONIRIBAS, MD, PhDUCLAJAMESALLISON, PhDMD AndersonCancer CenterCARLJUNE, MDThe University ofPennsylvaniaJEDDWOLCHOK, MD, PhDMemorial SloanKettering Cancer CenterJEFFREYBLUESTONE, PhDPresident CEOParker Institute forCancer ImmunotherapySEANPARKERFounder ChairmanParker Institute forCancer ImmunotherapySTEPHEN SHERWIN, MDUCSFJEFF HUBERGRAILNINA BHARDWAJ, MD, PhDMount SinaiELLIOTT SIGAL, MD, PhDNEATHOMAS DANIELArch Venture PartnersELIZABETH JAFFEE, MDJohns HopkinsLEWISLANIER, PhDUCSFLAURIEGLIMCHER, MDDana-FarberCancer InstituteProgrammaticCollaboratorsScientific Steering CommitteeDAN LITTMAN, MD, PhDNYUCRYSTALMACKALL, MDStanford MedicineLARRY TURKA, MDHarvard Medical SchoolNIR HACOHEN, PhDBroad InstituteNINABHARDWAJ,MD, PhDMount SinaiROBERTSCHREIBER, PhDWashington UniversitySTEPHENFORMAN, MDCity of HopePHILGREENBERG, MDFred HutchJIMHEATH, PhDInstitute for Systems Biology
Our Research AgendaLarge collaborative efforts focus on four areas withgreat potential.Best-in-class T-cellsAdvance the next generation of T-cell therapies to provide targeted, safe,long-lasting treatments to conquer cancer.Immune ResponseUncover why some patients respond to immunotherapy while others may notto overcome cancer drug resistance.Tumor Antigen DiscoveryPinpoint novel cancer cell markers that will become the foundation for newtherapies and personalized treatments.Tumor MicroenvironmentDiscover how tumors impair immune cells, which will jumpstart the creation oftherapies that can fight hard-to-treat solid tumors.
INFORMATICSInformatics is involved in all aspects of translational clinical research:I IDEATION Providing context through public data integration Evaluating new experimental technologies Supporting clinical trial designI EXECUTION Sample tracking and data collection Clinical data entry and management Correlative assays data managementI ANALYSIS Integrative data analysis Developing and scaling analytical methods Supporting computational efforts across theconsortium
Informatics supports PICI Clinical and Research studies withsystems, programming, and biostatso PICI Sponsored Clinical Studies Clinical Programming and Systems Setup forPICI trials (8 ) Clinical Report Generation & Biostats Global library project Towards a standardized set of CRFs/collectionparameters to use across PICI studieso PICI Sponsored Research Studies Programming and Systems Setup forResearch Studies Prospective collection underway for studyingimmune-related AEs after IO Novel deployment of REDCap environment We are running it on a GCE environment thathas others in the community excited. Configuration is available athttps://github.com/ParkerICI/redcap-k8stemplates MedidataVeevaEndpointOracle Argus SafetyKubernetes
Primary analysis pipelines in place for 15 assaysInput from our investigators informs how we prioritize further development of thesepipelinesAssays that can beautomatedPrototype stage:have run once or twice,Advanced prototype:have run a few times,Standard analysis:have run many times,Mature analysis, mostlyautomatedPrototype stage:have run once or twice,Advanced prototype:have run a few times,Standard analysis:have run many times,Mature analysis,as automated as ngscRNA-seqAssays that need ahuman in the loopVectraIMCMIBICODEXCytokines/LuminexFlowCyTOF
Systems and infrastructure to support PICI trials andtranslational analyses (latest iteration)Clinical & Research OpsTranslational
Informatics Progress across PICIo 30 projects across 7 sites, 15 data types, 10 publicationso PICI worked with MD Anderson to identify TCR features in tumorsassociated with response to neoadjuvant nivolumab in high-riskresectable metastatic melanoma patients.o Amaria et al. Nature Medicine 2018o PICI worked with UCLA to apply in-house CyTOF methodology,revealing differences in PD-1 expression patterns by anatomic site.o Davidson et al. Clinical Cancer Research 2018o and moreo Enabled novel work with PICI developed toolso https://github.com/parkericio “Deep” integrative analysis of multi-omic trials
Outline of talk/examples of progressing IO End-to-end clinical trial analyses Approaches to think about (PD1) Resistance and Toxicities Approaches to think about neoantigen prediction (TESLA) Bringing data together to answer key questions
Pancreatic Study Combining NivoCD40 and Chemo (PRINCE)
PRINCE OverviewExploring safety and efficacy of chemotherapy and immunotherapy combinationsfor metastatic pancreatic canceroChemotherapy CD40 Ab anti-PD-1: Standard of care chemotherapy Nab-paclitaxel Gemcitabine Immunotherapies CD40 Antibody APX005M (Apexigen) Nivolumab anti-PD-1 checkpoint inhibitor (Bristol-Myers Squibb)
PRINCE OverviewGemcitabine nab-Paclitaxel CD40 Ab APX005M /PD-1 Ab NivolumabCD40Antibody4(APX005M)Trafficking of T-cellsto tumors (CTLs)5Infiltration of T-cellsinto tumors(CTLs, endothelial cells)3Pancreatic cancerChemotherapyPriming andactivation(APCs ody(Nivolumab)2Cancer antigenpresentation(dendritic cells/APC)Tumor6Recognition ofcancer cellsby T-cells(CTLs, cancer cells)1Release ofcancer antigens(cancer cell death)CD40 antibody(APX005M)PD-1 antibody(Nivolumab)Chemotherapy7Killing ofcancer cells
Deep Immune ProfilingPatient SamplesBiomarkerSamplesGermline WESHLA Determination(MHC Class I and II)Tumor WESNeo-epitopePredictionRNAseq(tumor & blood)TumorTumor Genome/TMBTME GeneExpression SignatureMultiparameterImagingImmune ProfileCyTOF/FlowBloodClinicalMetadatactDNA: MutantKRASCytokine(serum)Harmonized methods of collection andprocessing at a central biorepositoryExtensiveComputationalAnalysis
PRINCE Phase 1b: Promising Efficacy SignalsCohort B1: Gem/NP/APX005M 0.1 mg/kgCohort B2: Gem/NP/APX005M 0.3 mg/kgCohort C1: Gem/NP/APX005M 0.1 mg/kg nivoCohort C2: Gem/NP/APX005M 0.3 mg/kg nivoOverall Response Rate (CR or PR) 46.7% (14/30)Historical ORR for Gem/NP: 23%Phase 2 ongoingClinical Snapshot date: 05MAR19Safety-evaluable Population
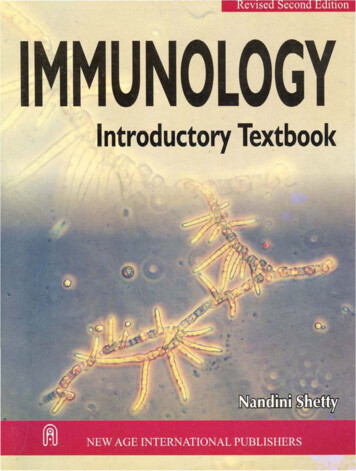
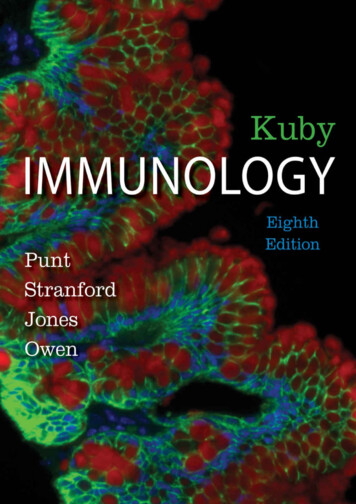
Tu m o r I m m u n e P r o f i l i n g w i t h H i g h - D i m e n s i o na l I m a g i n gVectra tumor imaging with 3 panelsreveals low overall immune infiltrate withhigher macrophages and low CD8 T CellsFraction of nucleated cellsCD68CD8Ki67PD-L1FoxP3panCK,DAPIImaging of baseline tumors with two technologies:Vectra and 30-marker OHSU mIHC
Circulating Tumor DNA: Mutant KRASEarly analysis suggests that KRAS fraction in cfDNA correlates with tumor diameterin patients who have measurable KRAS mutations at baseline (67% of patients)Cell-free DNA in blood Droplet digital PCR (ddPCR)assay to detect KRAS mutationsin cfDNA Measured the portion of cfDNAthat is confirmed to contain one ormore KRAS mutationsKRAS Variant Allelic FractionKRAS G12V, D, R mutationsSDPRPRPRSDPRPRTumor Sum Diameter (cm) Plasma cfDNA concentrationmeasured before mutationanalysisPRKRAS Allelic FractionTumor Sum DiameterTimepoint
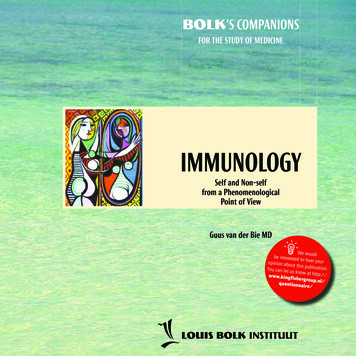
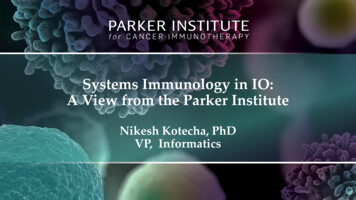
H i g h - d i m e n s i o n a l c yt o m e t r y f o r p r o f i l i n g o f i m m u n ed yn a m i c s i n b l o o dCD4 EMTregCyTOFImmune phenotyping(37 markers)FACS SymphonyT cell panel(28 markers)B2: Gem/NP APX005M 0.1mg/kgC2: Gem/NP APX005M 0.1mg/kg NivoMemory B cells(CD19 CD27 CD38-)Plasmablasts(CD19 CD27-)Treg-like CD38 (CD4 FoxP3 )CD4 CentralmemoryCD4 NaiveCD8 NaiveTEMRAEarly observations of immune changes with treatment:- Activation of B cells during the course of therapy- Activation of Tregs at the early timepointsCD8 EffectormemoryCD8 CentralmemoryCurrent work: Unbiased clustering analysisof cellular population dynamics
Outline of talk/examples of progressing IO End-to-end clinical trial analyses Approaches to think about (PD1) Resistance and Toxicities Approaches to think about neoantigen prediction (TESLA) Bringing data together to answer key questions
The problem of the majority2,250 active trials testing anti-PD1/PDL1 agents as of September 2018,PD-1totaling about 380,900 patient volunteersResponseResistancePD-1 “Responders” 35%PD-1 “Non-Responders” 65% 65% 247,585 patients will experience resistance inTotal 100trials alone (not accounting for SOC patients)Tang et. al. (2018) Nat Rev. Drug Discovery
Intrinsic & extrinsic factors: What’s knownHavel et. al. (2019) Nature Reviews
Important questions in breaking down & harmonizingbiomarker studies of PD-1At what clinical timepoint(s) was this measured?How was this measured?BiomarkerClinicalResponseto PD-1At what clinical timepoint was this measured?How was this measured?
PICI trials addressing the problem of PD -1resistancePICI trial nameMAHLERMelanoma Tx with Ipi/Nivo Enrolled atMultiple Centers MelanomaPRINCEChallenge addressed in design-Trial exclusively in patients who progressed on PD-1Prior PD-1 resistance type taken into account in analysisLongitudinal, multi-omic biomarker studies, standard processingWorking with partners to build out reference dataset (expandsample size)-Novel combinations in Pancreatic cancer, a novel tumor typeLongitudinal, multi-omic biomarker studies, standard processing-Novel biomarker (microbiome) as combination with PD-1Patients stratified by baseline microbiome (pro-resistance vs proresponse)Longitudinal biomarker studies, standard processingPancreatic Study Combining Nivo,CD-40 and ChemoMCGRAWMelanoma CP and Gut MicrobiomeAlteration With MicrobiomeIntervention-PORTER-Prostate Researching TranslationalEndpoints Correlated to Response toInform Use of Novel Combos-Novel combinations in castrate-resistance prostate cancer(CRPC), a novel tumor typePlatform trial designLongitudinal, multi-omic biomarker studies, standard processingSpencer, Wells & LaValle (2019) Trends in Cancer
We Ran A Workshop“Translational Approaches to PD-1 Resistance Workshop” Brought pharma non-profit science academia together todiscuss how PD1 resistance can be addressed throughtranslational science. Attendees from Merck, BMS, Genentech, Pfizer, Amgen,Regeneron; SITC, PICI, ISB; MDA/PICI, Yale, MSKCC/PICI Outcomes: core questions focus questions: How can data sharing be enabled between pharma? What should be the standard clinical definition of PD1resistance? What are the molecular phenotypes of cancer resistance toimmune killing?
What’s Coming – come join us! Molecular Phenotypes of Immune Resistance in Cancer Working group based out of, but not restricted to, the workshop Initial goals Draft white paper/review on mechanisms of immune resistance (non-clinical) Retrospective, integrative analysis of gene expression and WES datafrom published cohorts Lead by SITC/TimIOs & ISB/UNC & PICI A follow up to “The Immune Landscape of Cancer” Actively seeking collaborators with large molecular data sets from IO trials!
What about toxicities?
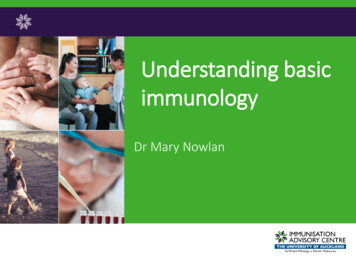
PICI Launches the Autoimmunityand Cancer Program in Partnershipwith JDRF and HelmsleyCONSORTIUM: PICI sites, academic labs, cancer centers, researchhospitals, foundations, pharma and governmentinstitutionsGOALS: Generate insight into the mechanisms behind irAEsfollowing immune checkpoint inhibitionPITUITARY HypophysitisLUNGS PneumonitisLIVER AutoimmuneHepatitis Understand irAE drug selectivity Determine target antigen specificityTHYROID Hypothyroid HyperthyroidHEART MyocarditisADRENAL Insuff iciencyPANCREAS T1DGASTRO INTESTINAL Colitis Determine overlap in mechanism with “classic”forms of autoimmune disease Identify at-risk patients early to reducethe incidence and/or severity of such eventsNERVOUS SYSTEM Guillaine–BarréSyndrome Myasthenia GravisEncephalitisRHEUMATOLOGIC Vasculitis ArthritisSKIN Vitiligo Psoriasis
Autoimmune Events Resulting frOm Systemic Modulationby ImmunoTherapy (AEROSMITH) Aim: To collect clinical data and blood samples on patients before, at the timeof, and after irAEs during checkpoint blockade therapy for cancer Goal: Enroll 1000 patients prospectively and follow-up for 1.5yrs Progress: 200 patients enrolled to date across 35 sites (April 2019)Distribution of Cancer Types collected so far: 50% melanoma lung 50% otherDistribution of AE Grades collected so far: 50% are Grade 1
Outline of talk/examples of progressing IO End-to-end clinical trial analyses Approaches to think about (PD1) Resistance and Toxicities Approaches to think about neoantigen prediction (TESLA) Bringing data together across PICI to answer key questions
Tu m o r - s p e c i f i c n e o e p i t o p e s a r e a t t r a c t i v e t a r g e t s f o rcancer therapeutics Truly tumor-specifico Novel peptideso No pre-existing toleranceo Immunogenic oSafer therapeutic profileMinimal risk of autoimmunityYarchoan, & al. , 2017 Possibility of targeting multi-neoantigens could be a response to tumor heterogeneity and evolutionHypothesis: if we can identify and target neoantigens with therapeutic agents, we can havepersonalized, safe, highly active therapies.
Neoantigens can be targeted by therapeutic vaccines
N e o a n t i g e n D i s c o v e r y Wo r k f l o wWES RNASequencingVariant IdentificationTumor cells NormaltissueMassSpec.Neoantigen identificationRanked neoepitopesDeep machinelearningAntigen processingmodelsMHC I BindingpredictionSNVMNVFSIndel
Neoantigen discovery pipelines are becoming morediverse and complexMedgenomeSpeedy and accurate identification ofneoantigen hasbeen identified as a criticalFrom Personalis Websitebottleneck for the delivery of neoantigenpromisesGenome Medicine20168:11
The need for benchmarking prediction algorithms isbecoming more pressingBenchmarking p r e d i c t i o n a l g o r i t h m s i s a p r e s s i n g n e e d
TESLA : a community -based effort to optimizingneoepitope discovery
T h e Tu m o r n e o E p i t o p e S e L e c t i o n A l l i a n c e ( T E S L A )Program GoalsoTESLA is a community-based initiative that aims to support the field’s efforts to developsafe and efficacious neoantigen-based therapeutics/vaccines for cancer by: Delineating the variation of neoepitope predictions in existing computational pipelines Generating high quality epitope validation sets that provide a basis to assess andimprove prediction pipelines Elucidating the key factors for accurate neo-epitope prediction
TESLA Participating Groups and Contributors 24 Academia/Non-Profits 22 Pharma/BiotechAdvaxis ImmunotherapiesAgenusAMGENBiontechBGI GenomicsBristol-Myers SquibbEpiVaxGenentechIlluminaISA PharmaceuticalsMSDMedImmuneMedgenomeNeon TherapeuticsOncolmmunityPersonalisSeven BridgesTEMPUSVaccibodyYu Bio
Schematic of TESLA
Va l i d a t i o n o f t h e p r e d i c t e d p e p t i d e s i s c e n t r a l t oalgorithm improvementoValidation aims at determining whether patient’s T cells are able to recognize the predictedneoepitope. Focus on peptides binding to Class I MHC (pMHC)oGoal: To validate predicted peptides in at least 2 assays guided by HLA restriction Availability of biological material
T E S L A F u n c t i o n a l Va l i d a t i o n M e t h o d s1. Peptide:MHC BindingA. Sette, LIAI2. ex vivo stimulationN. Bhardwaj, Mt Sinai
TESLA functional validation methods3. Tetramer detection (FACS)R. Schreiber, WUSTLP. Kvistborg, NKI4. NP-tetramer isolationJ. Heath, Caltech/ISB
There is no “consensus” neoantigen identificationpipeline.Conclusions Only few steps werecommonly used across allteams TESLA teams use a widevariety of approaches, tools,filters, etc. in their process. Most teams use 20-25features for predictionsManuscript in preparationConfidential – Do Not Post
Summary Overlap in ranked neoepitope are limited In the majority of the patients, reactive T cells could be detected againstsome of the predicted neoepitopes Substantial variability exists between teams for predicted and ranked theneoepitopeso There are a set of teams that can consistently identify and rank highly peptideMHC (pMHC) for which binding T-cells can be identifiedo Filtering seems to play in important role in the quality of the results Pipelines are complex and diverse across teams Overall 600 pMHC were tested for T-cell binding in a tetramer-basedassayso 37 of these pMHC were found to have binding T-cellso Majority of tested pMHC also have in-vitro MHC binding measurement in-depth analyses and elucidation of the key factors for accurate neoepitope prediction are underway
Outline of talk/examples of progressing IO End-to-end clinical trial analyses Approaches to think about (PD1) Resistance and Toxicities Approaches to think about neoantigen prediction (TESLA) Bringing data together across PICI to answer key questions
How we engage with sites and partners Ask broad questions of interest to PICI and the field Find stakeholders who are interested in asking the question with us and can bring dataand expertise to the table Align on a question of interest. Recent example:“What features of the immune repertoire are associated with particular somatictumor alterations, and how does this interaction shape the response tocheckpoint inhibitor therapy?”
Bring PICI together to answer the questionMSK Melanoma: Clinical (R/NR) WES/TCRTools from BroadInstitute: GATK, Mutect2,Polysolver,Oncotator,MSK NCLC: Clinical (R/NR) WES/TCRPICI Informatics Brings Together: 1000s of unique samplesData from 13 trials, 6 published papers300 WES samples1M TCR from 550 unique samplesBioinformatic methods for: Variant calling, HLA, HLA mutations. HLA copynumber, neoantigens, mutational signature ID,. TCR clustering Expertise in cancer immunotherapy: Renowned experts in cancer immunotherapy,immunology, immunogenomics, Tools fromStanfordImmunology:GLIPH(TCR Clustering)MDA Melanoma: Clinical (R/NR) WES/TCR/RNAIndustry Partners
Funneling DataSingularpatientsincompatiblewith remainingcohort300 IO patientsMissing clinicaldataObviouslyincorrectclinical dataLow TCRQualityLow WESQualityFinal unifiedcohort
TMB status is associated with TCR clonality inpretreatment.Wells, et. al. 2019. In Preparation.
Bringing it all together: how does TMB shapeTCR repertoire?Summary: TMB High is associated with a “short, flat” repertoiredistribution TMB Low is associated with a “long, skewed” repertoiredistributionWells, et. al. 2019. In Preparation.
Organize ourselves to answer broad questions working withPICI investigators industryoWhat are the genomic and immunologic features which predispose a patient to having animmune-related adverse event?oWhich features of the pre-infusion product are associated with durable clinical response to celltherapy?oWhat are the immune characteristics of the tumor microenvironment in castration-resistantprostate cancer, and how do they depend on previous treatmentoWhat are the molecular subtypes of cancer resistance to immune killing? How do these intersectwith aPD1 therapy?
Data organized to enable the PICI community toask further questions TCGA, published data, collaborator data, and PICI trial er TypesTechnologiesMeasurementsExample question,answered in seconds:“Which non-metastatichead and neck cancer sampleshaveCNVs in PD-L1 andCD8 percentage 15%?”
Thank you!nkotecha@parkerici.org
What about cell therapy?
Parker Institute: Next generation cell therapyCARL JUNE, MDThe University ofPennsylvaniaNovel CARs and vectors for clinical trialsNK cell evaluation and engineeringCASSIAN YEE, MDMD AndersonEndogenous T cell priming and therapeuticsCAR-T persistence and pediatric clinical trialsHIDEHO OKADA, MD, PhDUCSFCRYSTALL MACKALL, MDStanford MedicineT cell trafficking and glioma targetingNon-viral methods for T cell engineeringSTEPHEN FORMAN, MDCity of HopeLEWIS LANIER, PhDUCSFALEXANDER MARSON, MD, PhDUCSFNovel cell therapy programs in GBM56
Efforts at PICI informatics are focused in 4 areasMolecular DataClinical DataCTMSREPORTSEMRNOTESSAMPLES/LISLABSDICOMGENOMIC TESTSFLOWSEQUENCINGFISHMICROBIOMEIMAGINGTechnology Evaluation & Standardization”Deep” Immune ProfilingGENETIC/EPIGENETICSGENEEXPRESSIONWESNano StringTCRRNA nthusiastsMICROBIOMERNA SeqHD ImagingHD FLowFrom TumorFrom BloodscRNA-seqFrom bothIncorporate Prior Knowledge Public DataPubMedExternal databasesSkepticsIHC (Vectra)Nano StringPRIOR tsVisionariesPROTEINPast Sites’ Trials
You can’t afford to ignore the outside world
Each sample is annotatedwith multiple molecular measurements (features)Gene expression(RNAseq)Categorical Cell populations(CyTOF)Continuous endpointProgression-free survival
Pre-treatmentNumber of patientswith all features: 8Post-treatment.All subjects : 60 totalNo matter what, real -world data is incompleteFeatures from all assays : 30,000 total
The Core Questions How frequently do different mechanisms ofimmune evasion/suppression occur (in differentcancers)? How do different mechanisms of immune evasionor suppression correlate (in different cancers)? How does aPD-(L)1 alter the tumor resistancelandscape? What are the subtypes of resistance to aPD-(L)1therapy?
Vectra and 30-marker OHSU mIHC Vectra tumor imaging with 3 panels . Gem/NP APX005M .1mg/kg Nivo High-dimensional cytometry for profiling of immune dynamics in blood Treg CD4 Central memory CD4 Naive . and Cancer Program in Partnership with JDRF and Helmsley