Transcription
Defective Sec61a1 underlies a novel cause ofautosomal dominant severe congenital neutropeniaErika Van Nieuwenhove, MD, PhD,a,b,c* John S. Barber, BA,a,b* Julika Neumann, MSc,a,b Elien Smeets, MSc,dMathijs Willemsen, MD,a,b Emanuela Pasciuto, PhD,a,b Teresa Prezzemolo, PhD,a,b Vasiliki Lagou, PhD,a,bLaura Seldeslachts, MSc,a Bert Malengier-Devlies, MSc,e Mieke Metzemaekers, MSc,f Sarah Haßdenteufel, PhD,gAxelle Kerstens, MSc,b,h Rob van der Kant, PhD,b,i Frederic Rousseau, PhD,b,i Joost Schymkowitz, PhD,b,iDaniele Di Marino, PhD,j Sven Lang, PhD,g Richard Zimmermann, PhD,g Susan Schlenner, PhD,a Sebastian Munck, PhD,b,hPaul Proost, PhD,f Patrick Matthys, PhD,e Christine Devalck, MD,k Nancy Boeckx, MD, PhD,l,m Frank Claessens, PhD,dCarine Wouters, MD, PhD,n,o,pà Stephanie Humblet-Baron, MD, PhD,a,bà Isabelle Meyts, MD, PhD,q,r,sà andAdrian Liston, PhDa,b,tàLeuven and Brussels, Belgium; Homburg, Germany; Ancona, Italy; and Cambridge, United KingdomGRAPHICAL ABSTRACTSEC61A1 mutations cause autosomal dominant severe congenital neutropenia(single patient from non-consanguineous Belgian parents)Ca2 leakageDefective protein translocationCa2 Ca2 CytosolCytosolER lumenER elocyte MetamyelocyteBandSegmentedSevere Congenital NeutropeniaER, endoplasmic reticulum; UPR, unfolded protein response,From athe Department of Microbiology and Immunology, Laboratory of Adaptive Immunity, dthe Department of Cellular and Molecular Medicine, Laboratory of MolecularEndocrinology, ethe Department of Microbiology and Immunology, Laboratory of Immunobiology, Rega Institute for Medical Research, fthe Department of Microbiologyand Immunology, Laboratory of Molecular Immunology, Rega Institute for MedicalResearch, hthe VIB Bio Imaging Core & Department for Neuroscience, ithe Department of Cellular and Molecular Medicine, Switch Laboratory, lthe Department ofOncology, nthe Department of Microbiology and Immunology, Immunobiology, andqthe Department of Microbiology, Immunology and Transplantation, Laboratory forInborn Errors of Immunity, KU Leuven; bthe VIB-KU Leuven Center for Brain andDisease Research; cthe Department of Pediatrics, mthe Department of LaboratoryMedicine, othe Department of Pediatrics, Division of Pediatric Rheumatology, andrthe Department of Pediatrics, Division of Primary Immunodeficiencies, UniversityHospitals Leuven; gthe Department of Medical Biochemistry and Molecular Biology,Saarland University, Homburg; jthe Department of Life and Environmental Sciences,New York-Marche Structural Biology Center, Polytechnic University of Marche, Ancona; kthe Department of Hemato-Oncology, H opital Universitaire Des Enfants ReineFabiola, Universit e Libre de Bruxelles, Brussels; pthe ERN-RITA Executive Board,Leuven; sthe ERN-RITA Core Center, Leuven; and tthe Laboratory of LymphocyteSignalling and Development, The Babraham Institute, Babraham Research Campus,Cambridge.*These authors contributed equally to this work.àThese authors contributed equally as co-last authors.This work was supported by the VIB Grand Challenges program, the Research Foundation Flanders (Fonds voor Wetenschappelijk Onderzoek [FWO]) (grants G0A3218Nand G080818N), the KU Leuven (C1 grant C16/17/010), the Biotechnology and Biological Sciences Research Council through Institute Strategic Program Grant fundingmissense mutationsBBS/E/B/000C0427 and BBS/E/B/000C0428, and the Biotechnology and BiologicalSciences Research Council Core Capability Grant to the Babraham Institute. This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 779295. The Nikon A1R Eclipse TiConfocal microscope was funded by a Hercules type 1 AKUL/09/037 grant. TheVIB Flow Core provided research support in this study. E.V.N. is funded by an SB grant(1S22716N). The following authors are funded by postdoctoral grants from the FWO:S.H.-B. (grant 1272517N), EP (grant 12S8918N), and VL (grant 12H3319N). I.M. isfunded by the Jeffrey Modell Foundation and by the CSL Chair in Primary Immunodeficiencies. C.W. and I.M. are members of the European Reference Network for RareImmunodeficiency, Autoinflammatory and Autoimmune Diseases (Project ID No.739543). S.L. and R.Z. were supported by the DFG via IRTG1830.Disclosure of potential conflict of interest: I. Meyts is funded by the CSL Chair in PrimaryImmunodeficiencies. The rest of the authors declare that they have no relevant conflictsof interest.Received for publication October 21, 2019; revised March 24, 2020; accepted for publication March 27, 2020.Corresponding author: Adrian Liston, PhD, The Babraham Institute, Babraham HallHouse, Babraham, Cambridge CB22 3AT, United Kingdom. E-mail: adrian.liston@babraham.ac.uk. Or: Isabelle Meyts, MD, PhD, University Hospitals Leuven, Herestraat 49, Leuven, Belgium. E-mail: isabelle.meyts@uzleuven.be.0091-6749Ó 2020 The Authors. Published by Elsevier Inc. on behalf of the American Academy ofAllergy, Asthma & Immunology. This is an open access article under the CC BY-NCND license ).https://doi.org/10.1016/j.jaci.2020.03.0341
2 VAN NIEUWENHOVE ET ALBackground: The molecular cause of severe congenitalneutropenia (SCN) is unknown in 30% to 50% of patients.SEC61A1 encodes the a-subunit of the Sec61 complex, whichgoverns endoplasmic reticulum protein transport and passivecalcium leakage. Recently, mutations in SEC61A1 were reportedto be pathogenic in common variable immunodeficiency andglomerulocystic kidney disease.Objective: Our aim was to expand the spectrum of SEC61A1mediated disease to include autosomal dominant SCN.Methods: Whole exome sequencing findings were validated, andreported mutations were compared by Western blotting, Ca21flux assays, differentiation of transduced HL-60 cells, in vitrodifferentiation of primary CD34 cells, quantitative PCR forunfolded protein response (UPR) genes, and single-cell RNAsequencing on whole bone marrow.Results: We identified a novel de novo missense mutation inSEC61A1 (c.A275G;p.Q92R) in a patient with SCN who wasborn to nonconsanguineous Belgian parents. The mutationresults in diminished protein expression, disturbed proteintranslocation, and an increase in calcium leakage from theendoplasmic reticulum. In vitro differentiation of CD341 cellsrecapitulated the patient’s clinical arrest in granulopoiesis. Theimpact of Q92R-Sec61a1 on neutrophil maturation wasvalidated by using HL-60 cells, in which transduction reduceddifferentiation into CD11b1CD161 cells. A potential mechanismfor this defect is the uncontrolled initiation of the unfoldedprotein stress response, with single-cell analysis of primary bonemarrow revealing perturbed UPR in myeloid precursors andin vitro differentiation of primary CD341 cells revealingupregulation of CCAAT/enhancer-binding protein homologousprotein and immunoglobulin heavy chain binding proteinUPR-response genes.Conclusion: Specific mutations in SEC61A1 cause SCN throughdysregulation of the UPR. (J Allergy Clin Immunol2020;nnn:nnn-nnn.)Key words: Severe congenital neutropenia, SEC61A1, endoplasmicreticulum stress, unfolded protein response, whole exome sequencingSevere congenital neutropenias (SCNs) comprise a geneticallyheterogeneous group of inborn errors of immunity that arecharacterized by a differentiation arrest of granulopoiesis at thepromyelocyte stage. From early childhood, the low absolutenumber of circulating mature neutrophils predisposes patientswith SCN to life-threatening and recurrent infections, includingotitis, skin infections, deep abscesses, gingivitis, and septicemia.However, syndromic forms of SCN with extrahematopoieticmanifestations may also occur. Furthermore, patients are atincreased risk for the development of myelodysplastic syndromesor acute myeloid leukaemia.1,2 Autosomal dominant mutations inELANE, encoding for neutrophil elastase (NE) and autosomalrecessive mutations in HAX1, are the most common cause ofSCN,3 with mutations in 22 additional genes accounting for theremainder of the characterized cases. Despite genetic advances,around 30% to 50% of patients with a clinical diagnosis ofSCN are cared for without an identified pathogenic mutation.1,4,5The known monogenic defects disrupt distinct cellular pathways,demonstrating the value of gene discovery to provide insights intopathophysiologic mechanisms and potential targeted therapy.1Upregulation of unfolded protein response (UPR) in patientsJ ALLERGY CLIN IMMUNOLnnn 2020Abbreviations usedADTKD: Autosomal dominant tubulointerstitial kidney diseaseBiP: Immunoglobulin heavy chain binding proteinCHOP: CCAAT/enhancer-binding protein homologous proteinCVID: Common variable immune deficiencyDMSO: Dimethyl sulfoxideER: Endoplasmic reticulumG-CSF: Granulocyte colony-stimulating factorNE: Neutrophil elastaseqPCR: Quantitative polymerase chain reactionSCN: Severe congenital neutropeniaTM: Transmembrane helixUPR: Unfolded protein responseWT: Wild-typewith mutant ELANE,6,7 enhanced endoplasmic reticulum (ER)stress (G6PC3 and JAGN1),8,9 disturbed endosome trafficking(VPS13B and VPS45),10,11 and defective ribosome biogenesis(SBDS, DNAJC21, and EFL1) have all been implicated aspotential mechanisms.12-15 Cellular stress is a recurring themein SCN, indicating that the neutrophil differentiation process ishighly sensitive to deregulated cellular stress.SEC61A1 encodes for the a-subunit of the heterotrimericSec61 complex, the principal component of the human translocon. This structure is responsible for cotranslational or posttranslational signal peptide–dependent transport of newly synthesizedproteins into the ER and for the integration of nascent proteinsinto the ER membrane.16,17 In addition, the Sec61 channel alsopassively leaks calcium, contributing to the calcium balance ofthe cell. The term Sec61-channelopathies encompasses a familyof inherited or acquired diseases derived either from direct detrimental effects on Sec61 subunits or from indirect influence onSec61 channel gating.16 The intricate network involved in fulfilling Sec61 function implicates a broad spectrum of associated disease, including autosomal dominant polycystic liver disease(SEC6318 and SEC61B19) and diabetes (DNAJC320). Recently,autosomal dominant mutations were reported in tubulointerstitialkidney disease (ADTKD) with congenital anemia and in primaryantibody deficiency with variable penetrance characterized by anintrinsic deficiency in plasma cell differentiation.21,22Here, we identify a new SEC61A1 mutation with autosomaldominant SCN and report on the mechanisms by which the mutation disturbs neutrophil differentiation and maturation. Biochemical characterization reveals both a quantitative defect due toprotein instability and functional impairment with dysregulatedcalcium homeostasis. Through in vitro modeling we propose amechanistic pathway of mutation-induced upregulation of theUPR leading to cellular arrest of myeloid precursors.METHODSWritten informed consent was obtained from all participants, and the ethicscommittee of University Hospitals Leuven approved the study.Genetic analysisWhole exome sequencing and filtering were performed as previouslydescribed.23 For details, please refer to the Supplemental Data provided in thisarticle’s Online Repository at www.jacionline.org.
VAN NIEUWENHOVE ET AL 3J ALLERGY CLIN IMMUNOLVOLUME nnn, NUMBER nnVariant effect prediction on protein structureIn vitro protein transportMutations were analyzed by using the available cryo-EM structure (ProteinData Bank identifier 2wwb). All structural visualization was done by usingYASARA Structure (version 18.4.2424). Images were generated by usingRay-traced screenshots.Protein translocation experiments were performed as previouslydescribed.25,26 For a detailed description, please refer to the Supplemental Data.Western blottingFresh PBMCs and primary fibroblasts were solubilized in lysis buffercontaining 20 mM Tris-HCl (pH 7.5), 150 mM NaCl, 1 mM EDTA, 1 mMegtazic acid, 1% Triton-X, phosphatase inhibitor (PhosSTOP [Roche, Basel,Switzerland]), and protease inhibitor (Pierce Protease Inhibitor[ThermoFisher Scientific, Waltham, Mass]). A quantity of 50 mg of lysate,which was determined by using a Bradford Protein Assay (Bio-Rad, Hercules,Calif), was separated on a 4% to 12% bis-Tris acrylamide gel with3-(N-morpholino)propanesulfonic acid buffer (NuPAGE Precast Gel System[Thermo Fisher Scientific]) before blotting on polyvinylidene fluoridemembrane (GE Healthcare). After blocking, the membranes were incubatedwith specific primary antibodies: rabbit anti-Sec61a1 (Abcam, Cambridge,United Kingdom, Ab183046), rabbit anti-Actin (Sigma-Aldrich, St Louis,Mo, A2103), mouse anti–glyceraldehyde-3-phosphate dehydrogenase(Thermo Fisher Scientific, MA5-15738), and mouse anti-Vinculin (Sigma,V9264). Proteins were revealed by using ECL Prime (GE Healthcare,Chicago, Ill) or Western Lightning Plus-ECL (Perkin Elmer, Waltham,Mass) with the G:box Chemi-XRQ and quantified by using ImageJ software.RNA isolation and quantificationTotal RNA was isolated by using TRIzol reagent (Ambion, Thermo FisherScientific), except for CD341 cells, in which case the ReliaPrep RNA CellMiniprep System (Promega, Madison, Wis) was used. ComplementaryDNAwas synthesized by using the GoScriptTM Reverse Transcription System(Promega). Quantitative PCR was performed on a StepOnePlus real-time PCRsystem (ABI) with Fast SYBR Green Master Mix (Applied Biosystems, FosterCity, Calif) supplemented with gene-specific primers (see Table E1 in this article’s Online Repository at www.jacionline.org). Experiments were performed in duplicate and repeated thrice. For DDIT3 and HSPA5, TaqManGene Expression Assays were used (ThermoFisher Scientific) and expressionwas normalized to 18S.Confocal microscopyHL-60 cells were differentiated by using 1% dimethyl sulfoxide (DMSO)and allowed to attach to coverslips coated with poly-L-lysine (0.1%) (Sigma)by a 20-minute incubation in PBS at room temperature. After fixation with 4%paraformaldehyde (or with methanol for anti–protein disulphide isomerase),cells were permeabilized with 0.1% Triton X-100 in PBS and incubated inblocking buffer (PBS 1 2% BSA 1 10% donkey serum 1 0.1% TritonX-100). The specific primary antibodies used include rabbit anti-GM130(G7295, Sigma) for Golgi detection, rabbit anti-protein disulphideisomerase (3501S, Cell Signaling Technology, Danvers, Mass) for ER detection, and 4’,6-diamino-2-phenylindole (D1306; Molecular Probes, Eugene,Ore). The secondary antibody used was donkey anti-rabbit Alexa Fluor 555(A31572; Molecular Probes). Images were acquired with the Nikon A1Rconfocal unit mounted on an Eclipse Ti inverted microscope.Calcium fluxAfter labeling with Zombie Aqua (Biolegend, San Diego, Calif, catalog No.4231), cells were loaded with 1 mM FuraRed AM (Thermo Fisher Scientific,catalog No. F3020) in HBSS and incubated in calcium-free buffer (150 mMNaCl, 6 mM KCl, 10 mM HEPES, and 1.2 mM MgCl2 [pH 7.4]). Followingacquisition of background signals, 1 mM thapsigargin was added and acquisition was immediately resumed for 10 minutes by using BD FACSCanto II. FuraRed was recorded as the ratio of emission at 450/50 nm following excitationat 405 nm and emission at 670 nm following excitation at 488 nm. Thecollected data (FACSDiva software, BD Biosciences, San Jose, Calif) wereanalyzed as mean fluorescence ratio by using the Kinetics platform providedin FlowJo version 10.6.0 software (Tree Star Inc, Ashland, Ore).Differentiation of CD341 cells from peripheral bloodCD341 cells were isolated from PBMCs by using the CD34 MicroBead KitUltraPure (Miltenyi) and were differentiated by using SCF, FLT3L, TPO, IL-3,and G-CSF. For a detailed description, please refer to the Supplemental Data.Flow cytometryThawed PBMCs were stained in Brilliant Stain Buffer (BD Biosciences) forlive-dead and surface markers by using anti-human antibodies. Data werecollected on BD Symphony (BD Biosciences) and analyzed by using FlowJo forMac version 10.5 (Tree Star Inc). Primary neutrophils were isolated by using theEasySep Direct Human Neutrophil Isolation Kit (StemCell Technologies,Vancouver, British Columbia, Canada) and incubated with Fc block (MiltenyiBiotec, Bergisch Gladbach, Germany) before staining with mAbs. Flowcytometric analysis was performed with a FACS BD LSR Fortessa X20 (BDBiosciences). Analysis was performed with FlowJo software (LLC). For detailson the antibodies used, refer to the Supplemental Data.Single-cell sequencingSingle-cell RNA sequencing libraries were generated by using a commercial droplet platform (Chromium Controller system [10x Genomics, Pleasanton, Calif]). Briefly, the EasySep RBC Depletion Reagent (StemCellTechnologies) was used to deplete erythrocytes from whole bone marrowsamples collected in heparinized tubes. The cell count and viability of the cellswere assessed by using a LUNA dual fluorescence cell counter (LogosBiosystems, South Korea), and as per the 10x Genomics recommendations(Single-Cell 3’ Reagent Kits Version 2 User Guide; CG00052 Rev B), weaimed at a target recovery of 6,000 cells per sample. After the cell count andquality control, the samples were immediately loaded individually onto theChromium Controller. Single-cell RNA sequencing libraries were prepared byusing the manufacturer recommendations, and at the different check points thelibrary quality was assessed by using Qubit (ThermoFisher) and Bioanalyzer(Agilent, Santa Clara, Calif). With a sequencing coverage target of 50,000reads per cell, single-cell libraries were sequenced on the Illumina HiSeq4000platform by using paired-end sequencing workflow with 10x version 3 readparameters (28-8-0-91 cycles). For single-cell sequencing analysis, pleaserefer to the Supplemental Data provided.Annexin V and propidium iodide stainingPBMCs were treated for 24 hours with DMSO (vehicle control),thapsigargin (1 mM), brefeldin A (4 mg/mL), or tunicamycin (10 mg/mL).After the PBMCs had been stained with Zombie Aqua, cells were stained withallophycocyanin-annexin V (Invitrogen, Thermo Fisher Scientific) andpropidium iodide (00-6990) according to the manufacturer’s instructions,followed by acquisition using the BD FACSCanto II system.Lentiviral transductionHuman SEC61A1 (NM 013336.4) was cloned into the pWPXL backboneby using an In-Fusion HD Cloning Kit (Takara Bio USA, Mountainview, Calif).HEK293T cells were transfected with lentiviral vectors and second-generationpackaging plasmids by using X-tremeGEne HP Transfection Reagent (SigmaAldrich). Confluent HL60 cells were resuspended in filtered undiluted viruscontaining medium with 5 mg/mL of polybrene for 16 hours. TransducedHL-60 cells were sorted with BD FACSAria II gating on live GFP1 cells.Differentiation of HL60 cellsHL-60 cells were plated in T75 flasks and treated with 1% DMSO for 6 dayswith a refreshment of media on day 4. Differentiated cells were stained with
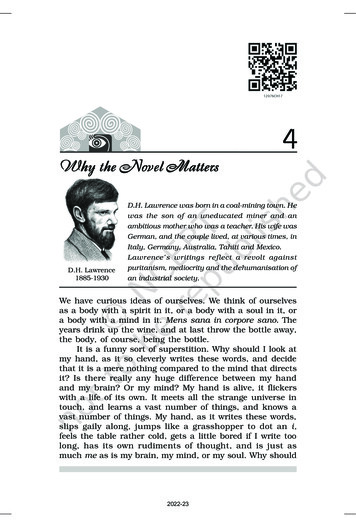
4 VAN NIEUWENHOVE ET ALZombie Aqua followed by surface staining with the antibodies anti-CD11ballophycocyanin-eFluor 780 (ICRF44, eBioscience, San Diego, Calif) andanti-CD16 PerCP (3G8, BioLegend). Cells were acquired by using the BDFACSCanto II system. For cytospin preparations, single-cell suspensions werespun on a glass slide and stained with hematoxylin and eosin. Cells werevisualized on a Leica DM 2000 microscope (Leica Microsystems, Wetzlar,Germany) for manual counting by 3 independent researchers.StatisticsStatistical analyses were performed by using a (un)paired t test or asindicated.Data sharing statementFor original data please contact Stephanie Humblet-Baron (E-mail address:stephanie.humbletbaron@kuleuven.be). The 10X Genomics RNA sequencingdata on bone marrow samples are available at the Gene Expression Omnibusunder accession number GSE137496.RESULTSIdentification of a de novo mutation in SEC61A1 in apatient with SCNThe index patient is a 19-year-old female who was born at termas the only child to nonconsanguineous parents of EuropeanBelgian descent. Her birth weight was 2750 g (–1.8 SD) (Fig 1, A).At the age of 4 months she presented with a retroauricularStaphylococcus aureus abscess and subsequently suffered fromrecurrent otitis, bronchitis, sinusitis, and tonsillitis thatnecessitated a tonsillectomy at age 5 years. At the age of 1year, she was treated for varicella that was complicated bybacterial superinfection treated with oral antibiotics. Aside fromher infectious susceptibility, she presented with oral aphthosis,problematic wound healing, gingivitis, and an episode of limitedverrucae plantaris. She was diagnosed with SCN when herneutrophil levels were analyzed during hospitalization forenteritis at the age of 2years. At 7 years of age, she developedpneumonia with Streptococcus viridans complicated byempyema. Aside from prophylactic antibiotics, she beganreceiving subcutaneous granulocyte colony-stimulating factor(G-CSF) at times of infection from the age of 7 years. Followingan Escherichia coli abscess in her facial region at the age of 15years and septicemia secondary to a gluteal E coli abscess ayear later, she began receiving daily G-CSF. When G-CSFtherapy was tapered to every 2 days, she developed a refractoryperianal abscess with Proteus mirabilis that cleared only aftersurgical drainage, intravenous antibiotic treatment, andlong-term administration of G-CSF at a rate of 12 mg/kg perday. Her neutrophil counts were repeatedly below 0.5 3109/Lbut responsive to G-CSF treatment (see Fig E1 in this article’sOnline Repository at www.jacionline.org). Before any initiationof G-CSF treatment at age 3 years, her complete blood countshowed a total leukocyte level of 4.79 3 109/L with a neutrophillevel of 0.048 3 109/L, lymphocyte level of 2.108 3 109/L,monocyte level of 1.916 3 109/L, eosinophil level of0.287 3 109/L, and basophil level of 0.096 3 x109/L. The resultof testing for anti-granulocyte antibodies was negative, andfurther laboratory work-up revealed hypergammaglobulinemiabefore the initiation of daily G-CSF (in particular, IgG2 andIgA [see Fig E1]), mild thrombocytopenia (a nadir of 104[reference range 150-450 3 109/L]), and discrete intermittentanemia (a nadir of 10.2 [reference range 12.0-16.0g/dL]). UnderJ ALLERGY CLIN IMMUNOLnnn 2020daily G-CSF treatment her total leukocyte numbers increased to9.19 3 109/L (reference range 4.0-10.0), with a myelocyte level0%]), neutrophil levelof 0.1 3 109/L (1% [reference percentage of 3.4 3 109/L (37% [reference range 38%-77%]), lymphocytelevel of 2.2 3 109/L (24% [reference range 20%-50%]), basophil1%]), relativelevel of 0.2 3 109/L (2% [reference percentage monocytosis with a monocyte level of 2.4 3 109/L (26%[reference range 2.0%-10.0%]), and relative eosinophilia withan eosinophil level of 1.0 3 109/L (10% [reference range 6%]). Bone marrow analysis before G-CSF treatment showeda maturation arrest in granulopoiesis at the level of thepromyelocytes and myelocytes (Fig 1, B).Whole exome sequencing was performed after negative geneticscreening of SBDS, GATA2, and CXCR4 through Sangersequencing and negative genetic screening of known genes forSCN (ELANE, G6PC3, GFI1, HAX1, LAMTOR2, SLC37A4,USB1, VPS13B, SBDS, VPS45, WAS, and JAGN1) and inborn errors of immunity through custom-designed gene panels. Throughfiltering for rare de novo or recessive variants, we identified anovel heterozygous mutation in SEC61A1 (NM 013336),c.A275G:p.Gln92Arg, that was not registered in any publicdatabase and had functional scores predicted as damaging byPolymorphism Phenotyping, Sorting Intolerant fromTolerant, and Combined Annotation-Dependent Depletion(CADD 24.500; mutation significance cut-off 6.099) analyses(Fig 1, C). To date, mutations in SEC61A1 have been reportedin 2 kindreds with ADTKD (c.T200G:p.Val67Gly andc.A553G:p.Thr185Ala)21 and 2 kindreds with common variableimmune deficiency (CVID) with incomplete penetrance(c.T254A:p.Val85Asp and c.G1325T:p.Glu381*)22 (Fig 1, Dand see Table E2 in this article’s Online Repository at www.jacionline.org). Although neutropenia was observed in thep.V67G kindred in addition to the well-described late-onsetADTKD and congenital anemia, it was not further investigated.21In light of our patient, the cosegregation of SCN in the p.V67Gkindred may also be attributable to mutant SEC61A1. Conversely,we investigated the possibility of subclinical renal dysfunction inour patient. Ultrasound imaging revealed small bilateral kidneys(right kidney, 9.6 cm [–3.2 SD]; left kidney 9.8 cm [–2.5 SD]) thatwere morphologically normal. Her urine sediment analysis resultsand kidney function remained normal. However, her uric acidlevels were slightly elevated over the past year (6.6 mg/dL[reference range 2.6-6.0 mg/dL]). Otherwise, no evidence forextramedullary involvement was found. In view of our currentfindings, we conclude that mutations in SEC61A1 can give riseto a clinical spectrum of disease including SCN.Biochemical impact of SEC61A1 mutationsFirst, we investigated the structural consequences of theresulting mutations. Both of the neutropenia-associated mutationsaffect the well-conserved amino acid residues Gln92 (Q92) andVal67 (V67) (Fig 1, E). The heterotrimeric Sec61 translocon complex comprises Sec61b, Sec61g, and Sec61a1, with the lattercontaining 10 transmembrane helices (TMs) that form the centralchannel of Sec61. In the closed conformation, a so-called plugdomain between TM1 and TM2 interacts with the center of transmembrane helix bundle, thereby blocking and stabilizing thepore.21 It is believed that signal peptides of nascent proteins intercalate between TM2 and TM7, with displacement of TM2 andsubsequent opening of the ‘‘lateral gate’’ of the Sec61 complex
J ALLERGY CLIN IMMUNOLVOLUME nnn, NUMBER nnVAN NIEUWENHOVE ET AL 5FIG 1. Autosomal dominant mutations in SEC61A1 cause SCN. A, Pedigree of a family with segregation ofthe p.Q92R mutant allele. The index patient is denoted by a black symbol. B, May-Gr unwald Giemsa stainingof representative bone marrow smears from the index patient. Promyelocytes are marked by the symbol %,and myelocytes are marked by the symbol *. Magnification, 3500. C, Sequencing profiles demonstratingthe heterozygous SEC61A1 c.A275G:p.Gln92Arg mutation in the kindred. D, Table of all reported mutationsin SEC61A1 with associated phenotypes. E, Multiple alignment to display conservation exported by usingHomoloGene (National Center for Biotechnology Information). F-H, Illustration of mutated residues in greenobtained using available cryo-EM structure (Protein Data Bank identifier 2wwb), with lumenal view in (F)and cytosolic view in (H). The plug domain is visible in red, the Sec61b protein is visible in blue, and theSec61g subunit is visible in orange.comprising these 2 TMs. Utilizing the available cryo-EM structure (Protein Data Bank identifier 2wwb),27 we determined thatboth Q92 and V85 are located in TM2 (Fig 1, F-H). In the closedconformation, Q92 points into the core to form a hydrogen bondwith a neighboring residue, whereas in the open conformation, itforms a hydrogen bond with the translocating peptide. V85 islocated closer to the core of the helix bundle. Both Q92R andV85D introduce a buried charge in the hydrophobic core of theTM bundle without the presence of a counter charge and are therefore predicted to severely destabilize the helix bundle thermodynamically. V67 is situated in the middle of an a-helical part of theplug domain, and mutating this residue to a glycine is likely destabilizing (Fig 1, F-H). Glycine mutations notoriously destabilizea-helices thermodynamically, especially when occurring at internal positions.28 Thus, this mutation potentially affects the proteintranslocation regulatory function of the plug domain.Additionally, in the closed conformation, the wild-type (WT)side chain of V67 forms hydrophobic interactions with TM5and TM10 that are completely removed by the truncation toglycine, further decreasing the interaction energy between theplug domain and the 2 transmembrane helices. Mapping the electrostatic potential on the molecular surface of Sec61 revealed thatthe WT is positively charged, maintaining a constant distributionof the potential around the internal surface of the channel (see FigE2, A in this article’s Online Repository at www.jacionline.org).Although V67G does not disturb the electrostatic potential (seeFig E2, B), V85D increases the negative charge at the bottom ofthe channel (see Fig E2, C), in contrast to the Q92R, which insteadraises the positive charge on the inside of the channel (see Fig E2,D). These opposing alterations may directly disturb the conformational changes of the Sec61 complex or affect its ability to interactwith or translocate newly synthesized polypeptide chains. Using
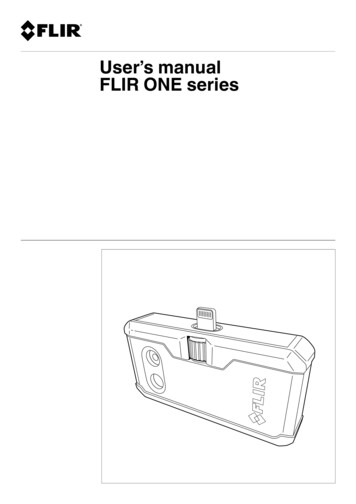
6 VAN NIEUWENHOVE ET ALJ ALLERGY CLIN IMMUNOLnnn 2020FIG 2. Mutations in SEC61A1 affect protein stability and disrupt ER/cytosol calcium homeostasis. A,Sec61a1 expression in healthy controls (HCs) and the patient (with P’ indicating the patient’s status as ofApril 2019 and P’’ indicating the patients status as of June 2018). B, Quantification of (A) normalized tothe average of the HCs. C, SEC61A1 mRNA expression in PBMCs (n 5 3) and primary fibroblasts from 2different passages (n 5 4), normalized to the average of the HCs. Unpaired t test. D, HL-60 cells transducedwith SEC61A1–green fluorescent protein (GFP) stained with anti–protein disulphide isomerase (PDI) (left)and anti-GM130 (right) (n 5 2). E, Ratio of cells with colocalization of Sec61a1 and GM130 over the totalnumber of cells from (D), normalized to WT. F, Calcium flux measurements in transduced HL-60 cells.Mean of 3 independent experiments with duplicates. G, Amplitude of calcium efflux following thapsigargin
J ALLERGY CLIN IMMUNOLVOLUME nnn, NUMBER nnthese structural predictions, we noted that pathogenic mutationscluster in the pore-forming region.In support of the predicted impact of
and Immunology, Laboratory of Molecular Immunology, Rega Institute for Medical . Allergy, Asthma & Immunology. This is an open accessarticle under the CC BY-NC- . CHOP: CCAAT/enhancer-binding protein homologous protein CVID: Common variable immune deficiency DMSO: Dimethyl sulfoxide ER: Endoplasmic reticulum G-CSF: Granulocyte colony .