Transcription
Share Learn Protect Executive BriefECRI Institute PSO Deep DiveOpioid Usein Acute CareXXIn-depth look at patientsafety events related toopioid use in acute careXXSystems-focused learningXXLeadership strategiesXXOnline resources
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareECRI INSTITUTE PSORonni P. Solomon, JD, Executive Vice President and General CounselAmy Goldberg-Alberts, MBA, FASHRM, CPHRM, Executive Director,Partnership SolutionsWilliam M. Marella, MBA, MMI, Executive Director, Operations and AnalyticsCatherine Pusey, RN, MBA, Associate Director, PSOBarbara G. Rebold, BSN, RN, MS, CPHQ, Director, Engagement and ImprovementPaul A. Anderson, Director, Risk Management PublicationsLeah M. Addis, MA, CPASRM, Risk Management AnalystJulia L. Barndt, MA, Associate EditorCarol Clark, BSN, RN, MJ, Patient Safety Analyst and ConsultantElizabeth Drozd, MS, MT(ASCP)SBB, CPPS, Patient Safety Analyst and ConsultantEdward Finley, Clinical Informatics AnalystRobert C. Giannini, NHA, CHTS-IM/CP, Patient Safety Analyst and ConsultantAmbily Gracebaby, MS, Clinical Informatics Analyst and ConsultantKelly C. Graham, BS, RN, Patient Safety Analyst and ConsultantGail M. Horvath, MSN, RN, CNOR, CRCST, Patient Safety Analyst and ConsultantRuth Ison, MDiv, STM, Patient Safety Analyst and ConsultantNancy Napolitano, PCHA, Patient Safety Analyst and ConsultantPatricia Neumann, RN, MS, HEM, Senior Patient Safety Analyst and ConsultantMary Parsons-Snyder, RN, BSN, MBA, Patient Safety Analyst and ConsultantSheila Rossi, MHA, Senior Patient Safety Analyst and ConsultantMelva Sanzon, Informatics AnalystStephanie Uses, PharmD, MJ, JD, Patient Safety Analyst and ConsultantJosi Wergin, CPHRM, CPASRM, ELS, Risk Management AnalystDiana Winters, CopyeditorAndrea J. Zavod, Managing EditorContributor: Christina Michalek, RPh, BScPharm, FASHP, Medication SafetySpecialist, Institute for Safe Medication PracticesADVISORY COUNCILHani Abujudeh, MD, MBA, FSIR, FACR, Cooper University HealthcareKatrina Belt, MPA, Healthcare Authority for Baptist HealthNancy E. Foster, American Hospital AssociationStephen T. Lawless, MD, MBA, Nemours Children’s Health SystemDavid C. Levin, MD, Jefferson Health SystemDavid L. Mayer, PhD, New York Metropolitan Transportation Authority (MTA)Michael A. Olympio, MD, Wake Forest University School of MedicineRichard G. Roberts, MD, JD, University of Wisconsin School of Medicineand Public HealthDebora Simmons, PhD, RN, CCNS, Independent ConsultantRobert M. Wachter, MD, University of California, San FranciscoMISSION STATEMENTECRI Institute PSO is a federally listed patient safety organization that is acomponent of ECRI Institute.ECRI Institute, a nonprofit organization, dedicates itself to bringing thediscipline of applied scientific research in healthcare to uncover the bestapproaches to improving patient care. As a pioneer in this science for nearly50 years, ECRI Institute marries experience and independence with theobjectivity of evidence-based research.ECRI Institute PSO Deep DiveTM: Opioid Use in Acute Care is published byECRI Institute, 5200 Butler Pike, Plymouth Meeting, PA 19462, USA;(610) 825-6000 (telephone); (610) 834-1275 (fax); info@ecri.org (e-mail).For more information about ECRI Institute PSO, send an e-mail to: pso@ecri.org.Share Learn ProtectiiTMShare Learn ProtectTMShare Learn ProtectTM 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.Share Learn ProtectTMShare Learn ProtectTMShare Learn ProtectTMSeptember 2017
Share Learn Protect Executive BriefECRI Institute PSO Deep DiveOpioid Usein Acute Care
About ECRI Institute PSOECRI Institute PSO is one of the first patient safety organizations (PSOs) to be federally certified under the provisions of the PatientSafety and Quality Improvement Act (PSQIA).PSQIA gives healthcare organizations a unique opportunity to voluntarily share their safety surveillance data in a protected environmentso PSOs can aggregate and analyze the data. The law also charges PSOs with the responsibility to share the findings and lessonslearned. The release of ECRI Institute PSO Deep Dive : Opioid Use in Acute Care is in keeping with that responsibility.September 2017
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareAcknowledgmentsECRI Institute PSO thanks its collaborating member organizations and partner patient safety organizations (PSOs) for sharing theiropioid-related events for this Deep Dive report. Over the course of six Deep Dive projects, participating healthcare organizationshave explored multiple safety topics through the aggregated analysis of shared events. ECRI Institute PSO encourages its membersto review ECRI Institute PSO Deep Dive : Opioid Use in Acute Care and convene a multidisciplinary team to discuss the applicabilityof the findings to their organizations.In addition to the many individuals at ECRI Institute who contributed to this report, ECRI Institute PSO acknowledges the followingindividuals for their insights:XXSameer Awsare, MD, FACPAssociate Executive Director,The Permanente Medical GroupXXAaron Bailey, PharmDSystem Director of Pharmacy Services,CHRISTUS HealthXXMason Brown, MD, MBAChief Medical Information Officer,Baptist Health (Montgomery, Alabama)XXPhilip W. Brummond, PharmD, MSDirector of Pharmacy,Froedtert & The Medical College of WisconsinHealth Network, Froedtert HospitalXXMario De Pinto, MDMedical Director, Pain Management Center (PMC)and Chronic Pain Service,University of California, San FranciscoXXVitaly Gordin, MDProfessor of Anesthesiology,Penn State College of Medicine, andAssociate Vice Chair of Pain Management,Hershey Medical CenterXXCraig Havican, BSN, RNCertified Epic Application Analyst,Sparrow HospitalXXNishaminy Kasbekar, PharmD, FASHPCorporate Director of Pharmacy,University of Pennsylvania Health SystemXXLee A. Kral, PharmD, BCPS, CPEClinical Pharmacy Specialist, Pain Management,The University of Iowa Hospitals & ClinicsXXSteve Mrozowski, MHADirector of Patient Safety,Hershey Medical CenterXXAnn Quinlan-Colwell, PhD, AHNBC, RN-BCClinical Nurse Specialist, Pain Management,New Hanover Regional Medical CenterXXJim Russell, RPhDirector of Pharmacy,Epic Systems CorporationXXMark Segal, PhD, FHIMSSVice President, Government and Industry Affairs,GE Healthcare DigitalXXDavid Showalter, PharmD, MBADirector of Pharmacy Services,Main Line HealthXXNeil SimonChief Operating Officer,Aprima Medical SoftwareXXMarvin Skinner, RPhDirector of Pharmacy Informatics,CHRISTUS HealthXXAshley Sweet, BSN, RN-BC, PCCNClinical Nurse Educator,Sparrow HospitalXXRegina Vukson, RN, BSBA, CPHQ, CPHRMSenior Risk Consultant,Optima Healthcare Insurance ServicesSeptember 2017 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.3
ECRI Institute PSO Deep Dive: Opioid Use in Acute Care4 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.September 2017
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareExecutive BriefBackground*Pain is common among patients in acute care settings, and it is not always effectively controlled through means other thanopioids. Many hospital patients do have legitimate indications for opioids.However, opioid therapy carries risks of harm, ranging from nausea or vomiting, itching, constipation, confusion, delirium,and allergic reactions to respiratory distress, respiratory depression with permanent injury, and possibly death. In addition toposing serious threats to patient safety, adverse events related to opioids can add substantial costs, in terms of both healthcarecharges and liability. The public health crisis of opioid-related substance use disorder has heightened concerns about diversionof controlled substances in hospitals, particularly opioids. Opioid use—and misuse—is increasingly being addressed throughlaws, regulations, and standards. The use of opioids in acute care is also part of a larger discussion about the effective and safemanagement of pain. All of these factors contribute to making opioid therapy a prime concern for healthcare organizations. ECRIInstitute PSO explored these issues, through the aggregated analysis of events shared by PSO members, in its sixth Deep Dive:ECRI Institute PSO Deep Dive : Opioid Use in Acute Care.* A free download of this Executive Brief and more information about the full report, ECRI Institute PSO Deep Dive :Opioids in Acute Care, is available at http://www.ecri.org/opioids.September 2017 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.5
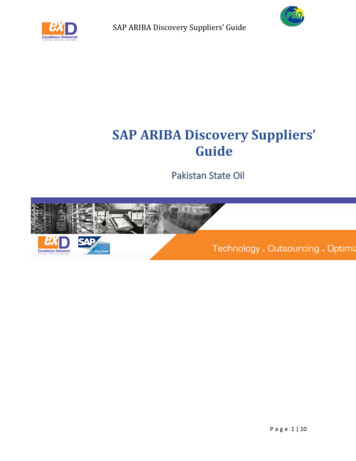
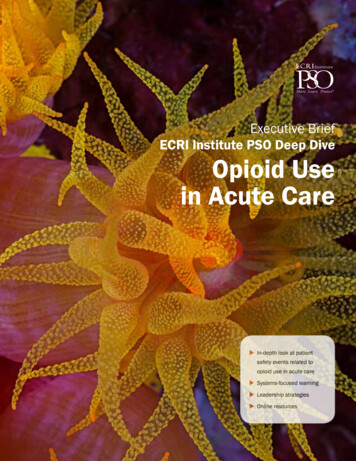
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareOpioids are thesecond mostfrequent class ofmedications tocause adverse drugreactions in hospitalsSource: Davies et al.1. Loopdiuretics2. Opioidanalgesics3. SystemiccorticosteroidsPatient HarmOpioid-related adverse events can cause significant morbidity,even mortality. Unfortunately, opioid-related harm is not rare.Opioids are the second most frequent class of medications tocause adverse drug reactions in hospitalized patients, trailingonly loop diuretics (Davies et al.).Oversedation and respiratory depression, which can leadto death if not quickly recognized and reversed, are primeconcerns. In reviews of medication utilization, administrationof naloxone, an agent used to reverse the effects of opioids,is often considered a general indicator that the patient suffered opioid-induced respiratory depression, although notevery instance of naloxone administration represents a caseof preventable opioid-induced respiratory depression. One estimate suggests that naloxone is given to about 0.2% to 0.7%of patients receiving opioids postoperatively (Weinger andLee). Although these percentages might seem low comparedwith rates of surgical complications, for example, even low6Naloxone, areversal agent, isSource: Weinger andLee to 2 to 7givenNaloxoneof every 1,000postoperativepatients on opioidsSource: Weinger and Lee.percentages can extrapolate to large numbers of patients.A rate of 0.5%, for example, equates to 1 patient out of 200—a substantial number given how many hospital patients receiveopioids.Oversedation and respiratory depression are not the onlyconcerns. Opioids may also be associated with delirium, euphoria, dysphoria, hallucinations, dizziness, falls, nausea, vomiting,aspiration pneumonia, constipation, hypotension, itching,and allergic reaction, among other adverse effects (JointCommission “Safe Use”; Hooten et al.). Long-term opioid use isassociated with heightened sensitivity to pain and opioid tolerance (DuPen et al.). 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.September 2017
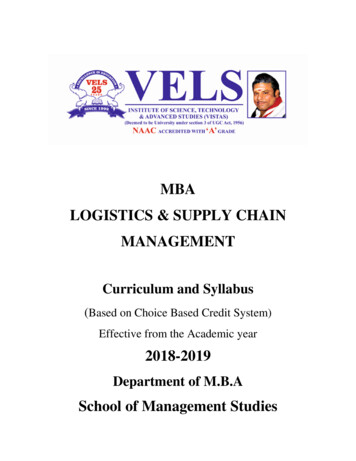
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareCases of postoperative opioid-induced respiratory depression in an anesthesia closed claims analysis:77%Source: Lee et al.resulted indeath orsevere braindamageThe medianpayment was 216,750, butabout 1 in 4payments wasgreater than 600,00097% werepreventableSource: Lee et al.97%Source: Lee et al.LiabilityOpioid-related liability claims can be costly. In a review of 357anesthesia closed malpractice claims related to acute pain,researchers identified 92 cases in which postoperative opioidinduced respiratory depression definitely, probably, or possiblyoccurred. Nearly all cases of respiratory depression (97%)were preventable, according to physician reviewers, and 77%resulted in death or severe brain damage. Payment was madein 45% of cases. The median payment was 216,750, butabout one in four payments was greater than 600,000.(Lee et al.)Laws, Regulations, and StandardsMany laws, regulations, and standards pertain to opioids, andsome have implications for use in acute care. Depending onthe circumstances, problems involving opioids may invite scrutiny by any or all of the agencies discussed below.The U.S. Food and Drug Administration (FDA) approves andregulates medications, including opioids and naloxone. Aswith other medications, FDA’s involvement extends to approving product labeling and boxed warnings. (U.S. FDA) The U.S.Drug Enforcement Administration is responsible for enforcingthe federal Controlled Substances Act and the regulations thatimplement it, ensuring that all transactions involving controlledsubstances occur within a “closed system” of distribution(U.S. DEA).September 2017Several Centers for Medicare and Medicaid Services(CMS) regulations and interpretive guidelines—particularlythose addressing nursing services, the medical record, andpharmacy services—discuss medication safety in detail. Forpatients receiving opioids, the interpretive guidelines stressthe importance of timely assessment and appropriate monitoring. (CMS “State Operations Manual”)The opioid misuse epidemic has also made opioids ingeneral an increasing focus for CMS. Although the agency’s“Opioid Misuse Strategy 2016” focuses on outpatient prescribing, one of the strategy’s four broad priorities is to “increasethe use of evidence-based practices for acute and chronic painmanagement.” The two objectives under this priority area areto expand the use of best practices and to promote the use ofnonpharmacologic, non-opioid pharmacologic, and multimodaltherapies as first-line strategies for managing pain. (CMS“Opioid Misuse Strategy 2016”)State laws and regulations address controlled substancesand the practice and licensure of healthcare workers.Hospitals must report certain professional review actions tothe National Practitioner Data Bank (NPDB) and the statelicensing board, and malpractice payers, including self-insuredorganizations, must report certain medical malpractice payments to the NPDB. In recent years, many state initiatives,such as prescription drug monitoring programs (which often 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.7
Opioid-Related Efforts at the Federal Level:Implications for Acute CareIn July 2017, the President’s Commission onCombating Drug Addiction and the Opioid Crisisissued its draft interim report to the president,which included several recommendations.Although the report is aimed largely at outpatientprescribing, following are recommendations fromthe report that may have implications for acutecare settings:ZZ Require education for prescribers regardingopioid prescribing and the risk of substanceuse disorder, such as through medical anddental school curricula, required courses forall U.S. Drug Enforcement Administration registrants, and continuing education.ZZ Expand access to medication-assisted treat-ment (MAT) for substance use disorder.——The complexity of the medications used inMAT underscores the importance of prescribercompetence in managing acute pain inpatients undergoing MAT and coordinationof acute pain management with providers ofsubstance use disorder treatment.ZZ Require that naloxone be prescribed whenevera high-risk opioid is prescribed.ZZ Supply federal funding and technical supportfor sharing of information among state andfederal (e.g., Veterans Health Administration)prescription drug monitoring programs.ZZ Harmonize patient privacy laws specificallyaddressing substance use disorder with theHealth Insurance Portability and AccountabilityAct (HIPAA).——Under 42 CFR Part 2, providers of substanceuse disorder treatment who receive federalassistance must get the patient’s writtenconsent in order to share information with thepatient’s other healthcare providers. In July2017, the Overdose Prevention and PatientSafety Act was introduced in the U.S. House ofRepresentatives to align 42 CFR Part 2 withHIPAA.Healthcare organizations should remain alertfor the final report, which was due to be issuedin fall 2017, and for any federal or state activityrelated to opioids.Sources: President’s Commission on Combating Drug Addiction and the Opioid Crisis. Draft interim report. 2017 Jul 31 [cited 2017 Aug /files/ondcp/commission-interim-report.pdf; Office of Tim Murphy, U.S. Congressman for the 18thDistrict of Pennsylvania. Murphy introduces legislation to prevent overdose deaths, protect patients [press release]. 2017 Jul 28 [cited 2017 Aug tect-patients/8 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.September 2017
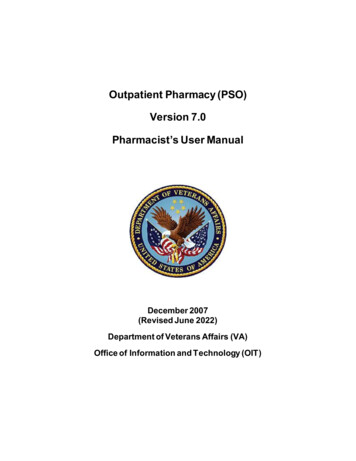
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareA case of postoperative respiratory failure adds:DescriptionAdditional healthcarecharges for postoperativerespiratory failureDebitCredit 54,0009 days to length of stay 54,000 in additionalhealthcare chargesSource: Zhan and MillerSource: Zhan and Millerrequire prescribers to check the state prescription databasebefore prescribing opioids), have focused on outpatient prescribing; however, organizations must be familiar with anyrequirements that pertain to inpatient settings as well. Criminalcodes may apply in the event of drug diversion or other unlawful possession or use.Accrediting agencies also address pain management.Joint Commission recently made changes to its standardsand elements of performance related to pain management.The agency revised its existing pain management standard;created an additional standard requiring hospitals to make“pain assessment and pain management, including safeopioid prescribing,” an organizational priority; and added elements of performance addressing pain management to otherexisting standards. One element of performance for the newstandard specifically states that hospitals should offer nonpharmacologic pain management modalities. (Joint Commission“Prepublication Requirements”)September 2017Healthcare organizations should watch for more laws, regulations, and standards related to opioids. At the federal level,the White House and legislators are contemplating actions totake in response to the opioid epidemic. Several of the stepsbeing considered would have implications for acute care settings. For more information, see “Opioid-Related Efforts at theFederal Level: Implications for Acute Care.”CostsOpioid-related adverse events can dramatically increasehealthcare charges. Using a sample of more than seven millionhospital discharges, researchers matched each case involvingspecific types of medical injury during hospitalization with control subjects who received care at the same hospital and hadthe same sex, age (within 10 years), race (white or nonwhite),and diagnosis-related group. Case and control subjects werealso matched based on mortality risk due to comorbidity. Theresearchers calculated the charges attributable to the medical injury by comparing the total charges for the case with themean for the matched controls. The study found that nearly 54,000 in excess charges could be attributed to postoperativerespiratory failure (resulting from any cause, not just opioids).This injury was also associated with an excess hospital lengthof stay of nine days. (Zhan and Miller) 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.9
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareResultsHarm ScoresA. Circumstances that couldcause adverse events (e.g.,look-alike medications, confusing equipment, etc.)ECRI Institute PSO searched its database for opioid-relatedevents that occurred between January 1, 2014, and November30, 2016. Of the 11,388 events analyzed by ECRI InstitutePSO, 7,218 (63%) were deemed relevant and further classifiedaccording to the taxonomy that ECRI Institute PSO developedfor analysts to use when classifying events. Hereafter, all datain this report refer to reports deemed relevant.B1. An event occurred but itdid not reach the individual(near miss or close call)because of chance aloneB2. An event occurred but itdid not reach the individual(near miss or close call)because of active recoveryefforts by caregiversTaxonomy CategoriesThe taxonomy is based on stages of the medication use process, with additional categories for adverse drug reactions anddrug diversion. For all of these categories except adverse drugreactions, the taxonomy includes several failure modes thatanalysts could select when reviewing events. Analysts couldselect more than one taxonomy category and more than onefailure mode for each event.C. An event occurred thatreached the individual but didnot cause harm and did notrequire increased monitoring(an error of omission such as amissed medication dose doesreach the individual)Figure 1. Event Breakdown by Taxonomy CategoryD. An event occurred thatrequired monitoring to confirmthat it resulted in no harmand/or required interventionto prevent harm2,536(35%)2,056(28%)E. An event occurred thatcontributed to or resulted intemporary harm and requiredtreatment or intervention1,181(16%)1,028(14%)F. An event occurred thatcontributed to or resultedin temporary harm andrequired initial or prolongedhospitalization553(8%)nG. An event occurred thatcontributed to or resulted inpermanent harmversioH. An event occurred thatresulted in a near-death event(e.g., required ICU care orother intervention necessaryto sustain life)DiMonitoringAdvere rseac dtio run ibing174(2%)Numbers add up to more than 7,218 and percentages add up to more than 100because more than one category could be selected for each event.10MS17355N 7,218 events with at least one failure mode in the category. 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.I. An event occurred that contributed to or resulted in deathICU: intensive care unitSeptember 2017
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareWithin the taxonomy developed by ECRI Institute PSO, theadministration and diversion categories accounted for the highest numbers of events. See Figure 1. Event Breakdown byTaxonomy Category.ECRI Institute PSO analysts could identify multiple failuremodes in a single event. For example, the following case involvedfailure modes in prescribing, transcribing, and dispensing:An emergency department (ED) technician entered 60 mgimmediate-release morphine, twice a day, as a medication thatthe patient took before admission. A nurse practitioner orderedthe medication for the patient, and a pharmacist verified theorder. Both the nurse practitioner and the pharmacist overrodeclinical decision support warnings indicating that the orderexceeded the maximum dose. A staff member noticed theerror: immediate-release morphine is not given in a dosage of60 mg twice a day. The patient confirmed that she took 60 mgof extended-release morphine twice a day.HarmEven so, it is notable that harm(categories E–I) was reported in20% of events in which a harmscore was indicated; in another64% of cases, the event reachedthe individual but no harmoccurred (categories C and D).See Figure 2. Event Breakdownby Harm Score (for Events with aHarm Score Indicated). Becauseopioid-related harm is sometimesdelayed or not detected (e.g., anoverdose death following thepurchase of medications thatwere diverted from a hospital),September 2017Figure 2. Event Breakdown by Harm Score(for Events with a Harm Score Indicated)A131 (4%)B400 (12%)C1,692 (50%)D476 (14%)E648 (19%)F35 (1%)G 0 (0%)H 12 (0%)I2 (0%)02004006008001,000 1,200 1,400 1,600 1,800Circumstances that could cause adverse eventsEvent that did not reach the individualEvent that reached the individual, no harmEvent that reached the individual, harm or deathN 3,396 events with a harm score indicated.See “Harm Scores” for definitions and groupings of harm scores. 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.MS17356A total of 3,396 event reports(47%) indicated the level of harmthat occurred. Harm scores, whichare based on the National Coordinating Council for MedicationError Reporting and Prevention’s“Index for Categorizing Medication Errors,” were indicated bythe individual reporting the eventrather than ECRI Institute PSOanalysts. The harm scores mayrepresent correlation, contribution, or causation; ECRI InstitutePSO analysts did not attempt todetermine causation or contribution based on the often limitedinformation available in reports.11
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareFigure 3. Distribution of Harm in Each Taxonomy Category1%0%2%7%11%3%3%1% es that could cause adverse events (A)Event that did not reach the individual (B)Event that reached the individual, no harm (C-D)N 3,396 events with a harm score indicated.Percentages do not always add up to 100 because of rounding.See “Harm Scores” for definitions and groupings of harm scores.these data may not reflect a complete picture of the harm associated with opioids in hospitals.Patient death occurred in two cases in which a harm scorewas reported but also in other cases in which no harm score wasreported. Although it was usually not possible to tell whether thefailure mode caused or contributed to the death, staff membersreporting the event sometimes suggested that it had, as in thefollowing event:Deviation from dosage for hydromorphone. The eventreached the patient; the patient died after the medication wasadministered. Referred for peer review.12MS17357Event that reached the individual, harm or death (E-I)Harm was not evenly distributed among the major taxonomycategories. In fact, the percentage of events that were associated with harm varied greatly among the categories. Aside fromevents involving adverse drug reactions, the two categories withthe highest percentages of harm were prescribing and monitoring. Therefore, although prescribing and monitoring were notamong the taxonomy categories with the highest numbers ofevents, they still pose significant concerns regarding the potential for significant harm. See Figure 3. Distribution of Harm inEach Taxonomy Category. 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.September 2017
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareFigure 4. Distribution of Harm in Each Location9%1%5%12%16%3%17%14%25%15%24%0% 0% 0%7% es that could cause adverse events (A)Event that did not reach the individual (B)Event that reached the individual, no harm (C-D)Event that reached the individual, harm or death (E-I)MS17358N 1,716 events for which both the location and harm score were indicated.Percentages do not always add up to 100 because of rounding.See “Harm Scores” for definitions and groupings of harm scores.OR: operating room; PACU: postanesthesia care unit.LocationA location, based on the Agency for Healthcare Research andQuality’s (AHRQ) Common Formats location categories, wasknown and indicated in 2,993 events (41%). Locations wereindicated by the individual reporting the event rather thanECRI Institute PSO analysts, and only one location could beselected for each event. By far the most frequently implicatedlocation was inpatient general care areas, such as medicalsurgical units (43% of events with a location indicated). Otherfrequent locations included the pharmacy (13%), critical careSeptember 2017areas (12%), the ED (10%), and operating rooms (ORs) or procedure areas such as the cardiac catheterization laboratoryand endoscopy area, including recovery areas such as the postanesthesia care unit (PACU) (9%).Harm varied by location as well (see Figure 4. Distributionof Harm in Each Location). It is notable that some of the settings with the highest proportions of harm are those wherepatients’ time on the unit is only temporary, such as for imaging, procedures, or outpatient care. This may suggest the need 2017 ECRI Institute. May be disseminated for internal educational purposes solely at the subscribing site.For broader use of these copyrighted materials, please contact ECRI Institute to obtain proper permission.13
ECRI Institute PSO Deep Dive: Opioid Use in Acute CareFigure 5. Distribution of Harm in Each Age Group12%28%1%1%10%9%9%64%68%6%26%23%39%68%50%45%2% 11%15%60%39%10%20%31%Infant( 2(0 N-2 eo8 nada te8ysda)ys 4yeadaruls)t(85 years)61%1%7%33%27%9%13%2
Penn State College of Medicine, and Associate Vice Chair of Pain Management, Hershey Medical Center XXCraig Havican, BSN, RN Certified Epic Application Analyst, Sparrow Hospital XXNishaminy Kasbekar, PharmD, FASHP Corporate Director of Pharmacy, University of Pennsylvania Health System XXLee A. Kral, PharmD, BCPS, CPE