Transcription
Advancing Patient Safetyin Cataract SurgeryA BETSY LEHMAN CENTER EXPERT PANEL REPORTMay 2016
The Betsy Lehman Center is a non-regulatory state agency that uses communications, research, and datato catalyze the efforts of providers, policymakers, and consumers working toward safer health care inMassachusetts.The Center is named for Betsy Lehman, a talented Boston Globe health reporter and mother of two young girlswho died in 1994 as the result of a preventable medical error when she was being treated for breast cancer. Hershocking and tragic death became a catalyst for change in approaches to patient safety both in Massachusettsand nationally.EXECUTIVE DIRECTORBOARD MEMBERSBarbara FainMaura HealeyAttorney GeneralMarylou SuddersSecretary ofHealth and HumanServices 2016 Betsy Lehman Center for Patient Safety and Medical Error ReductionJohn C. ChapmanUndersecretary ofConsumer Affairsand BusinessRegulationÁron BorosExecutive Directorof the Center forHealth Informationand Analysis
Advancing Patient Safety in Cataract SurgeryExpert PanelMichael Morley, MD, ScM [Co-chair]Assistant Clinical Professor of Ophthalmology,Harvard Medical SchoolOphthalmic Consultants of BostonKaren Nanji, MD, MPH [Co-chair]Assistant Professor of Anesthesia, Harvard Medical SchoolDepartment of Anesthesia, Critical Care and Pain MedicineMassachusetts General HospitalNicolas Argy, MD, JDQuality and Patient Safety Committee,Massachusetts Board of Registration in MedicineFellow in the Department of Health Law, Policy and ManagementBoston University School of Public HealthPatrice Baril, MS, RNNurse Manager, Surgical ServicesLahey Medical Center PeabodyJoseph Bayes, MDCommittee on the Quality of Medical Practice,Massachusetts Medical SocietyAssistant Professor of Anesthesia, Harvard Medical SchoolMassachusetts Eye and Ear InfirmaryMichael Chang, MDChair, Clinical Quality and Ethics Committee,Massachusetts Society of Eye Physicians and SurgeonsOphthalmologist, Eye Health ServicesTeresa Chen, MDAssociate Professor, Ophthalmology, Harvard Medical SchoolChief Quality Officer for Ophthalmology, Massachusetts Eye and EarInfirmary Glaucoma ServiceStefan Ianchulev, MDDirector Quality Assurance and ImprovementDepartment of Anesthesiology, Tufts Medical CenterKatie Murphy, RNAdministrator, Plymouth Laser & Surgical CenterCataract & Laser Center Centralwww.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction i
Advancing Patient Safety in Cataract SurgeryNatalie Nathan, MArch, MThPatient Family Advisory Council memberBeth Israel Deaconess Medical CenterSpiro Spanakis, DOAssistant Professor of Anesthesiology and Pediatrics,University of Massachusetts Medical SchoolDirector of Quality and Safety, UMass Memorial Medical Center,Department of AnesthesiologyNicola Truppin, JDPatient Family Advisory Council memberBeth Israel Deaconess Medical CenterPrincipal PartnersThe following organizations were critical to launching and sustainingthis initiative:Massachusetts Department of Public HealthMassachusetts Society of AnesthesiologistsMassachusetts Society of Eye Physicians and SurgeonsQuality and Patient Safety Division at the Board of Registration inMedicineSteering CommitteeWe gratefully acknowledge the following individuals for their essentialroles in convening the expert panel, supporting its data gathering, anddisseminating its findings.Beth E. ArnoldExecutive Secretary, Massachusetts Society of AnesthesiologistsJeffrey B. Cooper, PhDProfessor of Anesthesia, Harvard Medical School,Department of Anesthesia, Critical Care & Pain Medicine,Massachusetts General HospitalGregory P. DeConcillis, PA-C, CASCPresident, Massachusetts Association of Ambulatory Surgery CentersAnuj K. GoelVice President, Legal and Regulatory Affairs,Massachusetts Hospital Associationwww.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction ii
Advancing Patient Safety in Cataract SurgeryTara GregorioExecutive Director,Massachusetts Society of Eye Physicians and SurgeonsMaureen T. Keenan, RN, JDFormer Associate Director, Quality and Patient Safety Division,Massachusetts Board of Registration in MedicineElaine B. KirshenbaumVice President of Policy, Planning and Member Services,Massachusetts Medical SocietyPatricia McGaffigan, RN, MSChief Operating Officer & Sr. Vice President, Programs,National Patient Safety FoundationReviewersSeveral individuals generously offered their time and expertise toreview early drafts of this report. Their thoughtful scrutiny and inputwere integral to producing this final publication.Theresa V. Arnold, DPMManager, Clinical AnalysisPennsylvania Patient Safety AuthorityJeffrey B. Cooper, PhDProfessor of Anesthesia, Harvard Medical School,Department of Anesthesia, Critical Care & Pain Medicine,Massachusetts General HospitalKatherine T. Fillo, RN-BC, MPH, MAQuality Improvement Manager, Bureau of Health Care Safety andQuality, Massachusetts Department of Public HealthSusan Giordano, JDActing Director, Quality and Patient Safety Division,Massachusetts Board of Registration in MedicinePaula Griswold, MSExecutive Director,Massachusetts Coalition for the Prevention of Medical ErrorsBonnie Henderson, MDTreasurer, Executive Committee,American Society of Cataract and Refractive SurgeryMary C. Magee, RN, MSN, CPHQ, CPPSSenior Patient Safety/Quality Analyst,Pennsylvania Patient Safety Authoritywww.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction iii
Advancing Patient Safety in Cataract SurgeryLauren B. Nelson, JDDirector of Policy and Quality Improvement, Bureau of Health CareSafety and Quality, Massachusetts Department of Public HealthKristina Philipson, MPH, MADirector of Quality, Health Analytics and Finance,Center for Health Information and AnalysisSara Singer, PhDAssociate Professor of Health Care Management and Policy,Harvard T. H. Chan School of Public HealthMarian Wrobel, PhD, MPPDirector for Research and Analysis,Massachusetts Health Policy CommissionAcknowledgementsMany other individuals and organizations contributed in a multitudeof ways to this initiative. We wish to thank:Our data partners for sharing and analyzing information to informthe panel’s work: American Society of Anesthesiologists, AnesthesiaQuality Institute, CRICO, Health Research & Educational Trust,Harvard T. H. Chan School of Public Health, Pennsylvania PatientSafety Authority and ECRI Institute, and the Massachusetts HealthPolicy Commission.Leading organizations and their representatives who provided inputand information throughout the process: American Society of Cataractand Refractive Surgery, Center for Health Information and Analysis,Coverys, Medically Induced Trauma Support Services, OphthalmicMutual Insurance Company, and Tufts Health Plan.Our consultants: Mathematica Policy Research for supporting thepanel’s research work including its key informant interviews andevaluation work; and Martha Hayward for her contributions tointegrating patient advisors in the work of expert panels.The many unnamed individuals who contributed to this effort on ananonymous basis including: 12 national and international patientsafety experts, as well as 12 Massachusetts cataract surgeons, whoserved as key informants; over 100 Massachusetts cataract surgeonsand other facility staff who responded to our anesthesia survey;and more than 30 providers from local facilities who participated inconfidential conversations with Betsy Lehman Center staff. We aregrateful for their time, candor, and collective insights.www.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction iv
Advancing Patient Safety in Cataract SurgeryPrefaceWhen the Massachusetts Department of PublicHealth alerted the Betsy Lehman Center to anincrease in reports of Serious Reportable Events(SREs) associated with cataract surgery in early2015, we saw an opportunity to address an issuethat had emerged during the Center’s recent workto assess the current patient safety landscape inMassachusetts. Providers told us they were frustratedthat there were not more opportunities for sharedlearning of actionable information from the adverseevents and other patient safety data they collectivelyreport to state and federal agencies.It is well understood that a key obstacle to reducingthe incidence of preventable harm to patients acrossmedicine is the lack of good metrics. As they say, youcan’t fix what you don’t measure. The recent cluster ofcataract surgery adverse events allowed us to explorehow that limited data set might be leveraged to“signal” the existence of risks to patient safety acrossa medical specialty. We also wanted to test newmechanisms for the dissemination of timely alerts andrecommendations about notable patient safety risksand trends directly to providers who practice in thosefields here in Massachusetts.Our decision to focus on cataract surgery does notreflect a judgment that this particular procedurerepresents the most critical patient safety risk facingMassachusetts today. On the contrary, recent studiesshow that medication and diagnostic errors in allclinical settings are among the leading causes ofpreventable patient harm and death nationally.As noted in the expert panel report that follows,cataract removal is the most frequently performedsurgery in the United States and improves qualityof life for most patients. Because many individualwww.betsylehmancenterma.govcataract surgeons will never be personally involved ina serious harm event, they may not recognize the risk.Yet the large numbers of cataract surgeries mean thateven tiny rates of preventable error will result in largenumbers of patients harmed unnecessarily.The cataract surgery errors reported as SREs inMassachusetts represent so-called “never events”that were entirely preventable. By looking beneaththe surface to understand the systems and actionsthat allowed harm to occur in these cases, there ispotential to have an enormous impact by driving thenumber of adverse events in cataract surgery to zero.It is impossible to overstate the importance of havingwilling partners among the state’s professionalassociations, particularly the Massachusetts Society ofEye Physicians and Surgeons and the MassachusettsSociety of Anesthesiologists. In addition to theexpertise they contributed, their collaboration hasopened up communication channels with front linephysicians enabling us to gather information anddisseminate this work in ways that otherwise wouldnot be possible. We are grateful for their willingnessto take a leadership role in spreading the word thatpatient safety gains are made when practitionerscontinually look at their own work and ask, ‘How can Imake this even safer for my patients?’And there is more to come. As a next step, we aredeveloping a practical set of tools that providers canuse to improve the safety of their cataract surgerypractices. We also will be evaluating this initiative tounderstand how it can be repurposed to supportmeaningful, measurable change in other areas ofhealth care—with the ultimate goal of eliminatingpreventable patient harm in Massachusetts. 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction v
Advancing Patient Safety in Cataract SurgeryTable of ContentsEXECUTIVE SUMMARY 1INTRODUCTION 5I. A CALL TO ACTION 6II. CATARACT SURGERY IN MASSACHUSETTS TODAY 8The practice of cataract surgery in Massachusetts 8Errors in cataract surgery 8What is the risk? 8How do cataract surgeons perceive the risk? 10The meaning of “harm” in cataract surgery 11III. FINDINGS AND RECOMMENDATIONS 12Guiding principles 12Wrong lens, wrong eye, wrong patient 14Risk 1: Implantation of the wrong lens 14Risk 2: Surgery or anesthesia on the wrong eye 16Risk 3: Wrong patient surgery 17Shared contributors and cross-cutting recommendations19Injuries related to anesthesia 20Risk 4: Anesthesia choice and administration 20Safety profiles of eye anesthesia techniques 21Cataract anesthesia practices in Massachusetts today 24Anesthesia recommendations 26IV. ACTION STEPS 29Facility leaders and administrators 30Cataract surgeons 31Anesthesiologists 32Nurses and other clinical staff 32Nonclinical staff 32All clinicians and staff 32Patients 32CONCLUSION 33REFERENCESwww.betsylehmancenterma.gov34 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction
Advancing Patient Safety in Cataract SurgeryExecutive SummaryCataract surgery is among the safest procedures in medicine. Serious,permanent complications are rare, and most patients report asignificant increase in their quality of life following surgery.This combination of low risk and high benefit—and the fact thatabout half of all Americans develop cataracts that affect their visionby the age of 75—have helped make cataract surgery the singlemost common operation in the U.S. Almost four million cataractsurgeries were performed in 2015 nationally—more than 60,000 inMassachusetts alone—and these numbers are expected to grow infuture years as the population ages.Yet, like most surgery, cataract removal involves complex processesprone to occasional systems failures that can result in serious harmto patients. While the risk to any individual patient is low, the largevolume of procedures means that even a miniscule error rate can addup to many patients harmed.In early 2015, the Massachusetts Department of Public Health alertedthe Betsy Lehman Center to an uptick in reports of Serious ReportableEvents (SREs) associated with cataract surgery. These “never events”involved preventable errors that should not have resulted in harm topatients. The Center’s review of the data for the previous five yearsrevealed that the most frequent type of SRE associated with cataractsurgery was implantation of the wrong intraocular lens—that is, a lensnot intended for the patient. There were also multiple mistakes in theadministration of anesthesia, in some cases resulting in permanentloss of vision. Other errors included surgeries performed on thewrong eye and, in one case, on the wrong patient.What can be learned from these events? Over the course ofseven months, an expert panel of respected ophthalmologists,anesthesiologists, nurse managers, and patient representativesconvened by the Betsy Lehman Center examined the issues. Thepanel relied on a unique collection of national and local data—including confidential conversations with several of the facilitiesthat reported the SREs, surveys of Massachusetts cataract surgeonsand facilities, key informant interviews, guidelines from professionalorganizations, and queries of other databases including malpracticeinsurance claims data—to develop findings and recommendations.www.betsylehmancenterma.govTo advance safe andreliable cataract surgery inMassachusetts Foster a safety culture inwhich preventing patientharm is the top priority Engage physicians and staffat all levels to develop andimplement a patient safetyprogram Standardize and adhere toprotocols and processes,including effective timeouts Reassess anesthesiapractices Conduct a meaningfulinformed consent processthat engages patients inlens and anesthesia choices Recognize that even thebest-engineered systemsrequire continuousimprovement to addresspersistent and emergingrisks 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 1
Advancing Patient Safety in Cataract SurgeryMany of the reported events stemmed from: Breakdowns in communication Failure to conduct an effective time-out Lack of standardization within facilities—from lens orderforms to surgical site markings Issues related to safety cultureThe anesthesia-related incidents prompted deliberation over thechoice of anesthesia technique and credentialing and orientation ofnew anesthesia staff.KEY RECOMMENDATIONSIn addition to the more general principles for advancing safe andreliable cataract surgery noted above, the panel developed thefollowing recommendations:To prevent wrong lens, wrong eye, wrong patient errors– Institute a formal lens management policy that defines uniformprocesses for ordering, storing, selecting, and verifyingintraocular lenses Adopt a uniform, facility-wide policy for marking the operativeeye, and perform a separate time-out prior to a nerve block Use multiple patient identifiers and engage patients usingactive verification Perform robust time-outs before every key step in the procedureTo prevent injuries related to anesthesia– Use the least invasive form of anesthesia appropriate to the case Stay current on evidence-based practices for minimizing the riskof patient harm from anesthesia Engage patients in decisions about anesthesia and sedation Strengthen “onboarding” of new and contracted anesthesiastaff including thorough credentialing, formalized orientations,and observed eye block assessmentsThe call to action is for all who participate in the delivery of cataractsurgery to put themselves in the shoes of their peers who oncethought, “It will never happen to me.” The panel’s recommendationsencourage providers to promote a culture of safety and to implementpatient safety programs and evidence-based best practices toprevent events like the ones reported in Massachusetts fromhappening again.www.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 2
Advancing Patient Safety in Cataract SurgeryAdvancing Patient Safetyin Cataract SurgeryCataract surgery is among the safest procedures inmedicine. Serious, permanent complications are rare,and the vast majority of patients report a dramaticincrease in their quality of life.1This combination of low risk and high benefit—and thefact that about half of all Americans develop cataracts that affect theirvision by the age of 75—have helped make cataract surgery the singlemost common operation in the U.S.2,3 Almost four million cataractsurgeries were performed in 2015 nationally4—more than 60,000 inMassachusetts alone5—and these numbers are expected to grow infuture years as the population ages.6Yet, like most surgery, cataract removal involves complex processesprone to occasional systems failures that can result in serious harmto patients. While the risk to any individual patient is low, the largevolume of procedures means that even a miniscule error rate can addup to many patients harmed.In 2015, the Massachusetts Department of Public Health took noteof an uptick in hospital and ambulatory surgery center reports ofSerious Reportable Events (SREs) associated with cataract surgeryduring the previous year. These SREs are also known as “neverevents”—preventable errors that should not have resulted in patientharm. The Betsy Lehman Center’s review of the data for the previousfive years revealed that the most frequent type of SRE associated withcataract surgery was implantation of the wrong intraocular lens—thatis, a lens not intended for the patient. There were also multiple errorsin the administration of local anesthesia, in some cases resulting inpermanent loss of vision. Other errors included surgeries performedon the wrong eye and, in one case, on the wrong patient.These incidents took place in a wide range of settings, fromhospitals to ambulatory surgery centers, large and small, academicand non-academic, spanning the state from Cape Cod to WesternMassachusetts. One commonality was a sincere belief by the careteam—physicians, nurses, and administrative staff—that they werenot at risk for the types of errors that occurred or for the harm thatresulted not only to patients, but to themselves and in some cases tothe facility’s reputation.www.betsylehmancenterma.govHow could this havehappened [here]? we are allright on top of it we are very,very careful.- Operating room nurse at ahospital-affiliated surgery centerConfidential providerconversationsThe Betsy Lehman Centerconducted voluntaryconfidential conversations withseveral of the facilities thatreported adverse events to thestate. These sessions includedface-to-face interviews with 32surgeons, nurses, technicians,and administrators from threefacilities—an ambulatory eyesurgery center, a hospitalowned outpatient multispecialty surgery center, anda teaching hospital—plusa phone interview with arisk management directorfrom a fourth facility. Theconversations yieldedcompelling qualitativeinformation that was influentialin the panel’s deliberations.The quotations that appearthroughout this report aredrawn from these sessions. 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 5
Advancing Patient Safety in Cataract SurgeryA basic tenet of medicine dating back to Hippocrates has beento do no harm to patients. Thus, the cluster of cataract surgerySREs presents a unique set of challenges and opportunities. First,to leverage this “signal” data to promote safety culture and theimplementation of patient safety programs in a medical field that iswidely considered safe despite the fact that some patients continueto experience preventable harm. Second, to determine how best tomotivate health care professionals to accept the need for processimprovements in a high volume, low risk specialty where many ofthem may never be individually responsible for a serious harm event.I. A “call to action” to improve patient safetyin cataract surgery in MassachusettsIn response to the 2014 cluster of cataract-associated SREs, theMassachusetts Department of Public Health, the MassachusettsSociety of Eye Physicians and Surgeons, and the MassachusettsSociety of Anesthesiologists joined the Betsy Lehman Centerin a collaborative effort to issue an advisory for the purpose ofincreasing awareness of these potential patient safety threats amongophthalmologists, anesthesiologists, and staff at the facilities wherecataract surgeries are performed. In the fall of 2015, the Centerconvened an expert panel to identify and disseminate actionablestrategies for reducing the risk of future harm. The panel includedleading frontline providers in Massachusetts: ophthalmologists,anesthesiologists, cataract surgery nurses, and facility administratorsfrom diverse settings. Its members also included two patient advisorswho contributed important perspectives as medical consumers.Why focus on patient safetyin cataract surgery? Increasingly large numbers ofcataract surgeries performedeach year mean that evenlow rates of adverse eventswill impact large numbers ofpeople. Although severe permanentharm to patients is rare, therate of preventable errorin eye surgery is at leasttwice as high as most othersurgical specialties due torisks associated with left-rightside confusion and the use ofimplants. 7-9 Proven “best practices”already exist to mitigatevirtually all of the risks ofpatient harm in cataractsurgery, so major advancesin patient safety are withinreach.The goal of the panel’s work was to learn as much as possible fromavailable data and literature, increase awareness of common safetyrisks, and trigger the implementation of evidence-based bestpractices at all Massachusetts cataract surgery facilities. Providersoften implement process improvements after experiencing asignificant adverse event. The call to action is for all who participate inthe delivery of cataract surgery to put themselves in the shoes of theirpeers who once thought, “It will never happen to me.” This initiativeencourages surgeons, anesthesiologists, nurses, technicians, andadministrators to scrutinize their current practices and implementsteps to prevent events like the ones reported in Massachusetts fromhappening again.www.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 6
Advancing Patient Safety in Cataract SurgeryThe expert panel’s work and what informed itThe expert panel worked under the auspices of the Betsy Lehman Center, and was charged withdeveloping evidence-based recommendations for improving patient safety in cataract surgeryin Massachusetts. The panel held five in-person meetings over a seven-month period. Additionalsubgroup and member-to-member communications took place in between meetings. The panel’sdeliberations were informed by a thorough literature review and other essential research andanalysis conducted by Center staff, partner organizations, and expert panel members, including: Analysis of data from mandatory adverse event reporting systems in Massachusetts operatedby the Department of Public Health and the Quality and Patient Safety Division at the Boardof Registration in Medicine Surveys of Massachusetts cataract surgery providers regarding anesthesia practices:оо Cataract surgeons, in collaboration with MassachusettsSociety of Eye Physicians and Surgeonsоо Ambulatory Surgery Centers, in collaboration with the MassachusettsAssociation of Ambulatory Surgery Centersоо Hospitals, in collaboration with Massachusetts Hospital Association Key informant interviews:оо 12 Massachusetts cataract surgeonsоо 12 national experts in ophthalmology, anesthesiology, patient safety, and patient advocacy Analysis of payer claims by Massachusetts providers to detect practice patterns and errorsand complications related to cataract surgery:оо Massachusetts All Payer Claims Database (APCD), inpartnership with the Health Policy Commissionоо Medicare claims data, in partnership with the Department of Health Policyand Management at the Harvard T.H. Chan School of Public Health Queries by the Pennsylvania Patient Safety Authority of its adverse event databases forerrors and “near misses” associated with eye surgery during 2004 – 2015 Analysis of malpractice claims data related to cataract surgery:оо Anesthesia Closed Claim Project of the Anesthesia Quality Instituteоо CRICO Comparative Benchmarking System Analysis of data from national voluntary reporting systems and surveys:оо National Anesthesia Clinical Outcomes Registry (NACOR)оо ASC Quality Collaborationоо Anesthesia Incident Reporting System (AIRS)оо Annual national survey of American Society of Cataractand Refractive Surgeons (ASCRS) memberswww.betsylehmancenterma.gov 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 7
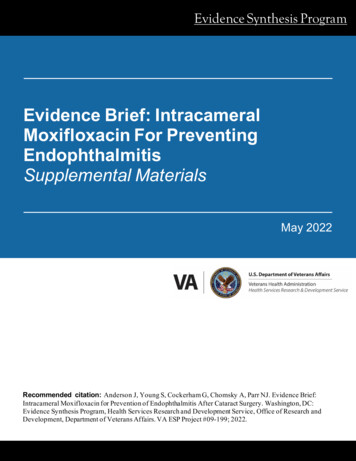
Advancing Patient Safety in Cataract SurgeryII. Cataract surgery in Massachusetts todayA. The practice of cataract surgery in MassachusettsAnalyses of Medicare, MassHealth (Medicaid), and commercial billingclaims data indicate that approximately 62,000 cataract surgeriestook place in Massachusetts in 2015 – likely an underestimate giventhat this figure does not include procedures performed in the state’sVeterans Health Administration facilities. Approximately 75% ofprocedures were performed on Medicare patients, most of whom areage 65 and over. Nearly 65% were performed in ambulatory surgerycenters (ASCs).10,11B. Errors in cataract surgeryi. What is the risk?During 2014 and 2015, six hospitals and six ASCs in Massachusettsreported a total of 16 SREs related to cataract surgeries to theDepartment of Public Health (DPH). Over this same period, theQuality and Patient Safety Division at the Board of Registration inMedicine (QPSD at BORIM) received confidential reports of sixadditional cataract surgery incidents that met its definition of areportable “major incident” but were not reported as SREs; QPSDat BORIM de-identified and summarized the information from theconfidential reports for the Betsy Lehman Center. The Center alsoreviewed SRE data from 2011-2013, which contain reports of anadditional 12 cataract surgery events. The SRE data are summarizedin Table 1.About cataract surgeryA cataract is a clouding ofthe lens. During surgery, theophthalmologist replacesthe natural eye lens withan artificial one. In mostcases, patients receive localanesthesia, either through anerve block (injection of localanesthetic into the spacesurrounding the nerves thatprovide sensation to the eye),or with topical numbing eyedrops. Cataract surgery isalmost always performed onan outpatient basis. Patientsusually make a quick recovery,with little pain and improvedvision within a day.Figure 1. Lens implantationTable 1. Cataract surgery “never events” reported as SREs to theMassachusetts Department of Public Health in 2011-15Event typeNumber2011-15 (2014-15)Wrong lens implanted15 (7)Surgery on wrong patient1 (1)Surgery on wrong eye1 (0)Wrong eye anesthetized5 (3)Nerve block causing loss of vision5 (5)Other1 (0)TOTAL28 (16)www.betsylehmancenterma.govReprinted with permission from the American Academyof Ophthalmology (2016). 2016 Betsy Lehman Center for Patient Safety and Medical Error Reduction 8
Advancing Patient Safety in Cataract SurgeryAlso included in both the DPH and QPSD at BORIM data are severalreports of retained foreign objects, infections, and other preventableadverse events. For example, three of the non-SRE cases involvedsuspected Toxic Anterior Segment Syndrome (TASS), often associatedwith deficiencies in instrument sterilization. It is worth noting thatalthough there were no recent Massachusetts reports of medicationerror in cataract surgery, improper eye blocks involving the wrongtype or concentration of anesthetic have been reported elsewhere.12While data from these state-mandated reporting systems offer awindow into the types of preventable harm events that are occurringin Massachusetts, they do not answer the question of how oftenthese events take place. Data on incidence are limited for severalreasons. It is well-established that adverse events are underreported throughout medical practice, not primarily from intentionalnoncompliance but because providers often fail to detect the adverseevents that are happening within their own practices.
We wish to thank: Our data partners for sharing and analyzing information to inform the panel's work: American Society of Anesthesiologists, Anesthesia Quality Institute, CRICO, Health Research & Educational Trust, Harvard T. H. Chan School of Public Health, Pennsylvania Patient Safety Authority and ECRI Institute, and the Massachusetts Health