Transcription
May 2019Leveraging Public Health Assets inMedicaid Managed CareState and territorial health agencies (S/THAs) and Medicaid agencies each serve at-risk populations andmay seek to align their resources to efficiently meet their goals. However, the two types of agencieshave differences in terminology, tools, and orientation that can present barriers to alignment andcollaboration.This three-part guide maps the public health capacities, assets, and resources onto the obligations anddirection of Medicaid agencies and their managed care health plans. Part I describes the current Medicaid and managed care context. This background sectionprovides a summary of Medicaid mandatory and optional benefits and populations. Thissegment of the report is intended to be used for introductory learning and as a resource forreferences. Part II describes the Medicaid managed care life cycle. This summary section is intended toassist state and territorial health officials (S/THOs) in strategically and effectively timingoutreach and partnership with Medicaid with respect to influencing managed care by describingthe different phases of Medicaid managed care. Part III describes Medicaid managed care key obligations and goals and identifies public healthassets that can assist Medicaid in meeting these obligations. This final and critical section ofthe guide equips S/THOs to lead strategic coordination efforts between S/THAs and stateMedicaid agencies by elevating the public health assets that can inform network adequacy,quality oversight and monitoring, quality and care delivery improvement, and consumersupports. This section provides the content and public health expertise that would be mostattractive to Medicaid managed care and could serve as the basis for ongoing partnership.Medicaid managed care is by no means the only context for a collaboration between state public healthand Medicaid agencies, but because of the prevalence of managed care arrangements in Medicaid, itwarrants a specific discussion. While this guide is intended for state and territorial health officials, it mayalso be used by other members of a health department team.
Table of ContentsPart I: Medicaid Managed Care Context .3Part II: Medicaid Managed Care Life Cycle .5Checklist for Engaging with Medicaid about Managed Care in Your State . 5Phase 1: Developing and Releasing the Request for Proposals . 8Phase 2: Selecting Plans and Preparing for Launch . 10Phase 3: Ongoing Plan Oversight and Care Improvement . 10Part III: Medicaid Obligations and Public Health Supports . 112Obligation: Network Adequacy . 13Obligation: Quality Oversight and Monitoring . 15Obligation: Quality and Care Delivery Improvement. 17Obligation: Consumer Supports . 19Conclusion . 20Acknowledgements. 20Appendix A: Additional Resources . 21Appendix B: State Medicaid Managed Care Enrollment Data Summary and Share of Medicaid Enrolleesin Managed Care . 24Appendix C: Medicaid Mandatory and Optional Benefits and Covered Populations . 27Appendix D: Index of Public Health Assets Mapped to Medicaid Managed Care Organization Obligations. 29References. 342
Part I: Medicaid Managed Care ContextMedicaid is a federal-state partnership that provides jointly-funded health insurance coverage toapproximately 73 million low-income people in the United States.i Medicaid primarily serves low-incomepeople who meet specific criteria in the following categories: children, senior citizens, people living withdisabilities, and pregnant women.ii Each state can elect to have a Medicaid program, but no state isrequired to do so.iii If a state chooses to have a Medicaid program, it must provide certain services,known as mandatory services, to certain groups of people, known as mandatory populations. AppendixC describes mandatory and optional services provided to Medicaid participants, as well as mandatoryand optional populations who may be eligible for Medicaid coverage. In return for meeting thesebaseline requirements, the federal government pays a fixed percentage (never less than 50%) of thecost of the provided services; states must pay the remaining proportion of costs. States can tailor theirprograms with respect to how they deliver services, what range of services they offer, and who iseligible for services by electing to cover optional services and optional populations.Medicaid programs across the nation are increasingly contracting with managed care organizations(MCOs) to provide healthcare services to Medicaid participants. In fact, more than 75 percent of the 73million Medicaid enrollees receive some or all of their Medicaid services through managed carearrangements.iv Understanding the relationship between a Medicaid agency and managed care healthplans can help S/THOs collaborate effectively with Medicaid leadership to strategically deploy publichealth interventions within a Medicaid program.Medicaid managed care generally describes a healthcare payment and delivery system in which a stateMedicaid program pays a fixed, per-person rate (referred to as a capitated or per member per monthrate) to an MCO for the delivery of Medicaid services.An MCO usually refers to a health plan that manages the risk of coverage, contracts with providers forprovision of services, processes provider claims or bills, and is paid by the purchaser of coverage. Thepurchaser in this instance is a state Medicaid program.Many different payment and delivery arrangements are commonly included under the umbrella term ofMedicaid managed care.1,2 In addition to the MCO model noted above, there are two common prepaid,limited benefit plans that can be thought of as managed care for a specific subset of services (e.g.,dental care or inpatient psychiatric care). These limited capitated arrangements are referred to asprepaid inpatient health plans (PIHPs) and prepaid ambulatory health plans (PAHPs).Primary care case management (PCCM) is another reimbursement arrangement under Medicaidmanaged care. This model is focused at the primary care level and includes a per-person fee paiddirectly to providers for the provision of a set of support services such as case management, diseasemanagement, and/or patient navigation. States may use a combination of all these arrangements foriMedicaid only enrollment is 65.9 million. The 73 million figure includes Children Health Insurance Program (CHIP) enrollment.Accessed from: https://www.medicaid.gov/medicaid/index.html.ii The subgroups described here are general categories, and often differ by each individual state.iii At date of publication, all 50 states and the District of Columbia have elected to have a Medicaid program.iv In a handful of states, the entire Medicaid benefit package—from physician services to long-term care to behavioral health—is provided by managed care health plans.3
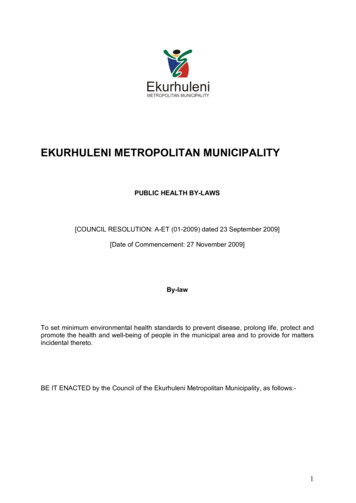
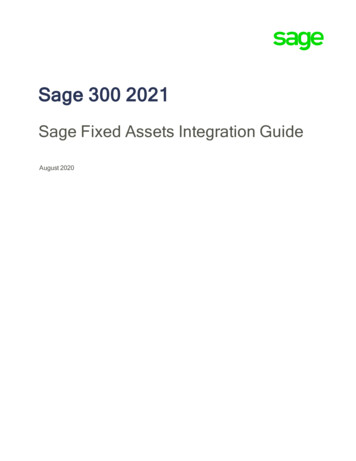
different populations and/or service sets.3 This guide focuses on MCOs, PIHPs, and PAHPs.v Appendix Boutlines the number of MCOs in each state.Figure 1: Share of Medicaid Population Covered Under Different Delivery Systems: Types of ManagedCare in Place (as of July 1, 2017)4Medicaid managed care has grown in prevalence and reach for several decades. Figure 1 illustrates thebreadth of Medicaid managed care across states, but there are major differences in levels of managedcare saturation and involvement among the states. Some states use managed care arrangements toprovide most of their Medicaid services, including community-based long-term care and dental andbehavioral health. In other states, only hospital and physician services are completely provided throughmanaged care, while other specialty services remain in the fee-for-service (FFS) environment. Likewise,some states enroll all Medicaid-eligible populations in managed care, while other states keep specificpopulations in fee-for-service care.vPIHP and PAHP arrangements are included under the “MCO” designation in Figure 1 and throughout the remainder of thedocument.4
Part II: Medicaid Managed Care Life CycleIn general, Medicaid programs that use MCOs to administer benefits follow a similar procurementprocess across states. To initiate a Medicaid managed care program, a Medicaid agency develops andpublishes a request for proposals (RFP) that lays out the general structure of the program, includingperformance expectations, quality measures, coverage rules, and reporting requirements for healthplans. Health plans develop and submit applications in response to the RFP and, based on theircompetitive scores, are selected to enter into contracts with the state for the provision of thecorresponding services. In most instances, states must offer a minimum of two plans to meet federalobligations.viOnce the state executes the contract, each health plan can develop its own approach to meeting therequirements of the contract in a manner that is consistent with federal and state requirements.5,6 As aresult, there are as many ways of delivering Medicaid managed care as there are health plans. While thestate may be prescriptive in a specific area or treatment protocol, it generally dictates the frameworkand coverage requirements, leaving it to health plans to decide specific elements, such as whether theyshould use alternative providers such as community health workers (CHW), offer telephonic or in-persondisease management, or contract with S/THAs for specialized services, such as sexually transmitteddisease (STD) identification and treatment.Although Medicaid serves only a portion of the lives within a jurisdiction for which a State Health Officialis responsible for all the lives, Medicaid population are frequently complex, underserved, and fragilesubpopulations who experience disparities in health status and health outcomes. S/THAs can providevaluable direction to Medicaid programs about how to address those complexities and mitigatedisparities through evidence-based practices to improve population health, strategies to engageconsumers and connect them to clinical and community services, and robust data to inform decisionmaking. Many state Medicaid agencies utilize MCOs to manage and deliver clinical care services;consequently, it is critical that S/THAs engage with Medicaid agencies in the development andimplementation of MCO contracts as a primary component of their Medicaid partnership activities.Checklist for Engaging with Medicaid about Managed Care in Your StateMedicaid MCO coverage and contracting processes vary by state and may require thoroughly examininga state’s Medicaid website and publicly available information. S/THA staff may also wish to engageMedicaid contacts in the state, if known, or build a relationship with appropriate Medicaid staff. Thefederal Medicaid website lists contact information for each state Medicaid agency.vi42 C.F.R. 438.52 2016. Available at p-delivered. Accessed 06-12-18. Managed careworks under a set of federal rules that were revised in 2016 and again in 2018. This rule (CMS-2390-F) touches many aspects ofmanaged care arrangements, and serves as the basis for state programs. State Medicaid agencies must submit managed careRFPs, contract templates, and rate structures to CMS for review.Appendix A lists links to the rule and materials explaining key aspects of the rules. Some elements of these rules have yet to befully implemented, and others are still evolving.5
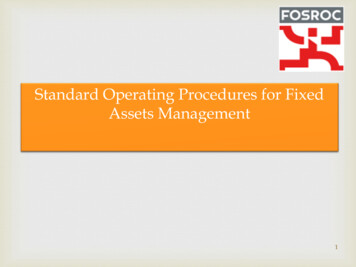
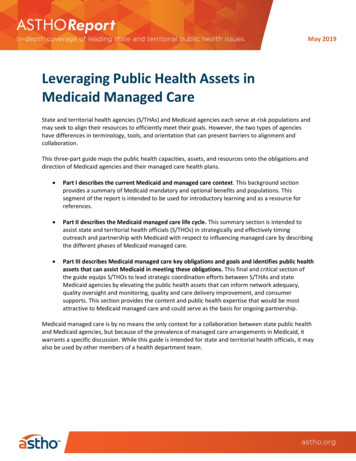
Use the following steps to engage with Medicaidabout managed care.Know who is in and who is out of managed care.At a Glance:Checklist for Engaging with MedicaidAbout Managed Care in Your StateThe first recommended step in approaching a state Know who is in and who is out.Medicaid agency is to assess which Medicaid Know what is included in your state’spopulations are enrolled in managed care in yourmanaged care arrangements.state. This will help determine how to most effectively Identify your state’s phase oftarget specific public health tools and programs tomanaged care.Medicaid. For example, public health efforts to Assemble the S/THA team andprevent prediabetic adults under 65 from progressingto fully developed diabetes will have less relevance indevelop a targeted, focused plan ofa state where Medicaid primarily covers older,approach.disabled adults. Likewise, a state that excludes dentalservices from its managed care plans may have less motivation to tackle that issue than a state wherehealth plans bear risk for their performance on preventive dental care quality measures. See Appendices3 and 4 for more information about each state’s Medicaid enrollment in managed care. S/THA staff canalso find state-by-state information about which Medicaid populations are enrolled in managed care inthe 2016 Medicaid Managed Care Enrollment Report.Know what is included in your state’s managed care arrangements.The second step is to assess which services are provided through your state’s managed care deliverysystem. For example, some states contract with a single group of health plans for all services. However,frequently there are also different health plans for different service lines. For example, a state maycontract with three health plans for traditional clinical services but may contract with two others forlong-term care services, and still another health plan entirely for behavioral health services. Some statesalso carve out prescription drug coverage, meaning those services may be delivered through differentpayment and delivery system entities.viiIdentify your state’s phase of managed care.The third step in engaging your state Medicaid agency is to identify which phase of the managed carelife cycle your state is in. Each state program is different, and even within a state, the current phase ofmanaged care may differ for different service lines. Regardless, managed care contracting generallyfollows a standard process (see Figure 2).viii Depending on where a state stands with respect to itscurrent phase of Medicaid managed care, certain activities will have more relevance and impact thanothers. States may also vary regarding how publicly accessible their MCO RFPs and contracts are. S/THAstaff should examine state Medicaid websites and engage the Medicaid office for this information.States may also seek Section 1115 research and demonstration waivers for certain aspects of theirdelivery system, which would likely occur prior to the life cycle described in this document. For moreinformation on the Section 1115 Demonstration waiver process, see the Medicaid About Section 1115Demonstrations web page.viiPlease note that health plans may not have direct control over drug utilization in a state where the Medicaid program uses apharmacy benefits manager.viii Managed care contracts vary in length but are generally issued in intervals of two to five years.6
Figure 2: Life Cycle of Managed Care Programs and Contracting ProcessDevelopment andRelease of RFPs(6 months-1 year)Governor or legislatureinitiates managed caretransition (or contract periodwill need to be renewedsoon).Planning is often ongoing anddependent on legislative andadministrative processes.Ongoing Plan Oversightand Care ImprovementAwarding Contracts andPreparing for Launch(2-5 years)(8 months-1 year)Assemble the state or territorial health agency (S/THA) team and develop a targeted, focusedplan of approach.The fourth step in the checklist is to identify potential areas for collaboration with your state Medicaidagency based on current statewide health trends. Medicaid and S/THAs share many common pressuresand demands, and often serve different cross-sections of the same populations. As a result, identifyingthree to five overarching common goals—such as introducing Medicaid to the state health improvementplan (SHIP) and its top priorities or reducing the prevalence and incidence of diabetes across the state—is helpful before focusing in on a more targeted set of objectives specific to the Medicaid population.S/THOs can target a few areas of mutual priority and help ensure that the business case for partnershipis oriented toward meeting Medicaid’s obligations as well as public health goals. One example of thistype of collaboration is CDC’s 6 18 Initiative: Accelerating Evidence into Action.7 Through this program,CDC provides technical assistance to state teams led by Medicaid and S/THAs to target six common andcostly health conditions through 18 evidence-based interventions to prevent and reduce the impact ofthose conditions. Many states have implemented this framework to create effective collaborationsbetween Medicaid agencies and S/THAs to address shared areas of focus. ASTHO’s Guide on GettingStarted with the CDC’s 6 18 Initiative provides more information on how interested states can pursuethe 6 18 framework.The four Medicaid managed care life cycle phases described below highlight the key elements presentduring the managed care procurement life cycle process and include identified areas of potentialcollaboration.7
Phase 1: Developing and Releasing the Request for ProposalsS/THAs can be especially instrumental during three components of the first phase of the managed carelife cycle: educating Medicaid about valuable public health priorities and resources, incorporating publichealth priorities as managed care contract goals and metrics, and improving rate setting and riskadjustment with population-level data.Educating Medicaid about Valuable Public Health Priorities and ResourcesDepending on a state’s legislative and administrative procedures, the managed care planning processmay begin prior to the RFP release. However, much of the planning often occurs simultaneously todeveloping and releasing the RFP. The RFP is the basis of the future contract that will be executedbetween the state and the health plans. Subsequently, S/THAs can have the biggest influence on aMedicaid managed care program by engaging with state Medicaid agencies while they are stilldeveloping their RFPs, either when they are initiating the programs or amending or renewing existingcontracts. Engaging early in the process will provide S/THAs with the best opportunity to advocate forincluding population health interventions in the managed care delivery system, especially in managedcare contracts.During the managed care planning process, state Medicaid agencies often use data from a variety ofsources outside of health insurance claims to inform their RFPs. S/THAs can identify and presentrelevant data (e.g., vital statistics, health opportunity indices, and disease surveillance statistics) and canalso analyze specific populations’ health needs and report their results toe Medicaid leadership. Sharingsuch data can shape Medicaid contracting decisions that ultimately support specific public healthinitiatives or at-risk populations.S/THAs can also identify effective interventions and services that are relevant to Medicaid programs andare already provided through public health programs and/or community-based public health serviceproviders.A S/THA should prepare the following information in anticipation of meeting with the state Medicaidagency about managed care procurement: The three most prevalent disease states or health conditions in the state.Evidence-based public health services and interventions that are already deployed in the stateto address the above priorities.The relative efficacy of the intervention(s) in preventing or mitigating the specific healthcondition and any cost reductions associated with that efficacy.Where and how those services or interventions are currently available for the at-risk population.Information about how residents (especially existing Medicaid members, if known) currentlyutilize those services.Table C below discusses further how S/THAs can support strategic planning efforts in these early stages.By providing this information, S/THAs can encourage Medicaid agencies to include performancerequirements in their RFPs and contract directing MCOs to target existing state health improvementpriorities and to use existing public health assets and providers to meet contract goals and targets. For8
example, Michigan’s 2015 Medicaid managed care RFP required MCOs to offer CHW services toenrollees with significant behavioral health issues and complex comorbidities. Michigan also requiredMCOs to maintain a CHW-to-enrollee ratio of at least one CHW for every 20,000 Medicaid enrollees.8Incorporating Public Health Priorities as Managed Care Goals and MetricsThe next opportunity for incorporating public health priorities into the Medicaid managed care space isfor S/THAs to work with state Medicaid agencies to isolate a finite number of shared priorities (brieflyexplored above) and incorporate them as goals and with metrics into RFPs. After laying out the businesscase for public health interventions, S/THOs can work with Medicaid agencies to review differentmeasure sets (described in greater detail later in this document) to choose appropriate metrics thatboth align with population health needs and would be feasible for health plans to collect. These metricscan be used to measure health plans’ progress toward meeting its stated goals and requirements.Improving Rate Setting and Risk Adjustment with Population-Level DataAt some stage of developing the RFP, states will offer proposed capitated rates to be paid to the healthplan for each member (a per person per month flat payment). These rates may be based on categoriesas broad as services to be provided together with the Medicaid members’ gender, age, or eligibilitygroup. Population-level data about health outcomes and social determinants of health (SDoH), whichMedicaid normally doesn’t collect, may help Medicaid agencies set those rates and perform riskadjustment.9,10 Such data include vital records (i.e., births, deaths, and infant mortality); registry data(e.g., from cancer registries); data regarding reportable diseases and conditions (e.g., STDs andHIV/AIDS); immunization data; data from WIC offices, family planning clinics, and reproductive healthclinics; newborn screening data; environmental health data; electronic reportable laboratory results;and population-based surveys.Social indices like the Social Vulnerability Index, the Health Opportunity Index, or other informatics toolsthat compile data on income, education, housing, and other SDoH may be better aligned with Medicaidmembers’ depth of need than traditional capitation rates based on broad demographic categories. Formore information on using population-level data to adjust payment, the report, Medicaid and SocialDeterminants of Health: Adjusting Payment and Measuring Health Outcomes, includes best practicesand state examples of SDoH data collection and risk adjustment in Medicaid programs. S/THAs can helpto identify any assets that exist in this space and can collect the disparate data sets to help inform therisk adjustment process.Table C: Engagement During the RFP Development PhaseState Medicaid Agency Engagement IdeasIdentify and provide data on: The top 3-5 areas identified for improvement in SHIP. Statewide disease surveillance data and registries. Statewide natality, morbidity, and mortality. Provider shortage designation areas. SDoH and the health indices of communities Medicaid serves.Identify evidence-based chronic and infectious disease programs that target needs identified in the SHIP.Identify existing public health services and providers that Medicaid should require MCOs to contract with to serve Medicaidparticipants, such as:11 CHWs Ryan White HIV/AIDS providers9
Immunization clinics Housing assistance and home modification programs Lead poisoning prevention and abatement programs Tobacco cessation and prevention programs Diabetes participation prevention programs Hypertension prevention programs. Unintended pregnancy prevention programs Telehealth programsIdentify areas for Medicaid cost savings and/or outcome improvements. Possible activities include: Identifying opportunities to utilize CHWs and other community-based health and social service providers. Identifying low-cost, high-impact health interventions, such as the 6 18 interventions. Using information from disease surveillance data to help identify and target health interventions for Medicaid-servingpopulations. Working with local stakeholders to identify key community health needs and successful community health interventionstrategies. Providing data highlighting provider shortage areas. Identifying evidence-based care coordination programs, outreach language, and materials that promote positive healthybehaviors.Propose goals and metrics to be in the contract that require the health plans to address: Reducing and preventing the 3-5 top priority conditions in the state health improvement plan. Emerging health issues, such as STD outbreaks and cancer clusters. SDoH. Requiring public health providers to be in all MCO networks.Provide Medicaid with population-level data on SDoH to refine rate setting and risk adjustment.Phase 2: Selecting Plans and Preparing for LaunchOnce state Medicaid agencies selects their health plans, they enter into contracts and begin preparing tolaunch the programs. For health plans that are new to the state Medicaid program, this process mayinclude readiness reviews of health plans’ procedures and operations. Sometimes these reviews findgaps in the current plan capacity (e.g., no preparedness plan or insufficient consumer supportcapacities). At this juncture, S/THAs can share best practices and respond to the identified gaps in careusing the suggestions listed in Table D.Table D: Engagement During the Review and Launch PhaseState Medicaid Agency Engagement Ideas Review health plan RFPs for service gaps and/or quality improvement strategy gaps.Help health plans draft their own disaster preparedness plan or emergency communications tools to meet disasterpreparedness and response requirements.Evaluate health plan proposals to address top state health improvement priorities, address SDoH, care forvulnerable/at-risk populations, establish cultural competency, and account for language needs. Verify sufficient datacollection, monitoring, and quality improvement plans.Help health plans develop a needs assessment that includes SDoH.Phase 3: Ongoing Plan Oversight and Care ImprovementContracts with managed care plans typically last two to five years. Each year, the state may identify newquality improvement initiatives (e.g., performance improvement plans [PIPs]), quality metrics, or othermodifications that health plans need to be address. They may also adjust reimbursement rates, which10
may change during ongoing plan operations due to delivery system reforms, quality performance, andcost controls.Many states are developing dashboards and other tools for hot-spotting problems and identifying areasneeding focus or improvement. Often, Medicaid agencies will identify an area of concern and pull planstogether to address and ameliorate the problems. For example, Medicaid agencies may assess claimsdata to identify opioid over-prescribing or high-cost populations’ service utilization patterns indicating alack of meaningful coordination or access to support services.Collaboration opportunities during this period vary widely. Some S/THAs can work with health plans andMedicaid agency leadership to identify performance or quality improvement opportunities. Other publichealth programs work with Medicaid agencies to survey MCOs on how they reimburse for and deliverevidence-based interventions—such as long-acting reversible contraception or asthma medications ordevices—in order to better understand barriers to uptake and opportunities for improvement. Forexample, for people living with HIV, the Ryan White HIV/AIDS Program can help Medicaid create viralload suppression performance measures and set benchmarks for performance improvement projects.(Table E demonstrates opportunities to engage with state Medicaid agencies during the contractmanagement phase.)Table E: Engagement During the Contract Management PhaseState Medicaid Agency Engagement IdeasMonitor and support health plan progress in reaching contract goals and targets focusing on: SDoH metrics.
3 Part I: Medicaid Managed Care Context Medicaid is a federal-state partnership that provides jointly-funded health insurance coverage to approximately 73 million low-income people in the United States.i Medicaid primarily serves low-income people who meet specific criteria in the following categories: children, senior citizens, people living with