Transcription
SEALED BIDREQUEST FOR PROPOSAL FORVermont Health Care Innovation ProjectState-led EvaluationExpected RFP Schedule Summary:DATE ISSUEDQUESTIONS DUEWRITTEN RESPONSES TO QUESTIONSBIDDERS’ CONFERENCE CALLPROPOSALS DUEDATE AND TIME OF BID OPENINGLOCATION OF BID OPENINGSELECTION NOTIFICATIONWORK START DATE11-17-201511-25-2015 by 1:00 pm12-1-201511-30-2015 at 10:00 amRevised 12-11-2015 by 1:00pmRevised 12-11-2015 at 2:00pmGreen Mountain Care Board89 Main StreetCity Center, 2nd FloorMontpelier VT05620Revised 12-15-2015Revised 1-22-2016PLEASE BE ADVISED THAT ALL NOTIFICATIONS, RELEASES, AND AMENDMENTSASSOCIATED WITH THIS RFP WILL BE POSTED .vermont.gov/RFPCONTACT AGENT:MAILING ADDRESS:Janet RichardGreen Mountain Care Board89 Main StreetMontpelier, VT 05620TELEPHONE:E-MAIL:(802) 828-1971Janet.Richard@vermont.gov1
SEALED BID INSTRUCTIONSAll bids must be sealed and must be addressed to the Green Mountain Care Board, 89 Main Street,Montpelier, Vermont 05620. BID ENVELOPES MUST BE CLEARLY MARKED ‘SEALED BID’AND SHOW THE REQUISITION NUMBER AND/OR BID TITLE, OPENING DATE AND NAMEOF BIDDER. ALL BID SUBMISSIONS MUST CONTAIN AN ORIGINAL AND FIVE (5)COMPLETE COPIES and one electronic copy, which may be submitted on a CD or to thefollowing email address: Janet.Richard@vermont.govAll bidders are hereby notified that sealed bids must be in the office of the Green Mountain Care Board(GMCB) by the bid due date and time. Bidders are cautioned that it is their responsibility to originate thesending of bids in sufficient time to insure receipt by the GMCB on or before the bid due date. Handcarried bids shall be delivered to a representative of the GMCB on or before the bid due date and stampedin by the GMCB representative to indicate the date and time of receipt. Bids not in possession of theGMCB by the due date and time will not be considered.The GMCB may change the date and/or time of bid openings. If a change is made, the GMCB will makea reasonable effort to inform all bidders.All bids will be opened publicly. Any interested party may attend bid openings. Bid results may berequested in writing and are available once an award has been made.From the issue date of this RFP until a Contractor is selected and the selection is announced, bidders areprohibited from communicating with any GMCB staff regarding this procurement, except with JanetRichard, Administrative Support Coordinator.The GMCB shall reserve the right to reject the proposal if this provision is violated.FAXED BIDS: FAXED bids will NOT be accepted.ELECTRONIC BIDS: ELECTRONIC bids are required in addition to the hard copies.2
Table of Contents1.Overview and General Information . 5Overview of the Vermont Health Care Innovation Project. 5VHCIP Evaluation Overview . 62.Schedule of Events . 7Questions and Answers . 7Bidder’s Conference . 73.Scope of Work. 7State-led Evaluation Study . 7Research Questions. 7Methodology . 10Site Visits . 10Provider Surveys. 16Reporting. 18Tasks & Deliverables . 20Evaluation Findings . 20Learning Dissemination Plan . 21Diffusion Products . 22Audiences for Diffusion . 22Contract Management . 23Failure to Comply with Contractual Requirements . 24Evaluation Criteria. 24Evaluation Factors . 24Procedural Instructions: . 244.Instructions for Bid Preparation .25General Instructions. 25Bid Submission Delivery Methods . 25Specific RFP Response . 255.Bid Submission .27DUE DATE . 27Bid Confidentiality. 27Submission Checklist . 27Attachments. 276.General Terms and Conditions .28Statement of Rights . 28Non-Disclosure Agreement . 28Contract Terms. 28Acknowledgment of Terms . 28Cancelation . 28Work Product . 29Confidentiality of State Information . 29Performance Measures. 30Taxes . 30Amendments. 303
Non-Collusion. 30Insurance. 30Business Registration . 30Contract Negotiation . 30Price Guarantee . 31ATTACHMENT C: STANDARD STATE PROVISIONS. 31CERTIFICATE OF COMPLIANCE . 34WORKERS’ COMPENSATION; STATE CONTRACTS COMPLIANCE REQUIREMENT. 36Offshore Outsourcing Questionnaire. 384
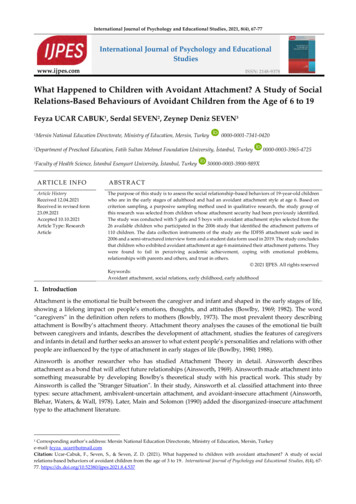
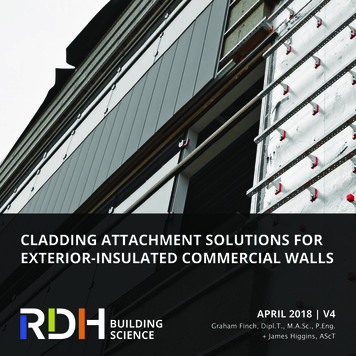
1.Overview and General InformationOverview of the Vermont Health Care Innovation ProjectVermont’s State Improvement Model (SIM) grant project, referred to as the Vermont Health CareInnovation Project (VHCIP), is expending 45 million in SIM grant funds to promote the “Triple Aim”objectives through the transformation of the State’s volume-driven delivery system to one that is valuedriven. The overarching goal of the SIM Initiative is to test whether new payment and service deliverymodels will produce superior results when implemented in the context of a state-sponsored health careinnovation plan. SIM Initiatives are comprised of two complementary components: State Innovation Models. Comprehensive approaches to transforming the health system of a statethat include new payment and delivery models as well as a broad array of other strategies to improvepopulation health. Payment and delivery models. Specific models, such as accountable care organizations (ACOs),patient-centered medical homes (PCMHs), or other integrated care models, that when combinedwith new payment methodologies can reward the provision of better care and health improvementsat lower cost.The SIM Initiative was created by the Patient Protection and Affordable Care Act (ACA) and isadministered by the Center for Medicare & Medicaid Innovation (CMMI). It is based on the premise thatGovernor-sponsored, multi-payer payment and delivery models that have broad stakeholder input andengagement, and set in the context of broader state innovation, will achieve sustainable delivery systemtransformation that significantly improves health system performance.VHCIP strives to increase provider-level accountability for cost and quality, monitoring and assessmentof cost and quality, sharing of health information across settings, and management of population health.To achieve these outcomes, VHCIP is supporting the design, implementation, and evaluation of a varietyof activities that build upon the State’s health insurance reforms and experiences gained as an earlyadopter of innovative delivery and payment models.Overall, VHCIP seeks to use SIM funds tostrive towards better care, better health andlower costs. In Vermont’s SIMimplementation, the Triple Aim is advancedthrough a series of tasks that fall under fivemajor focus areas: Payment Model Design andImplementation: Supporting creationand implementation of value-basedpayments for providers in Vermontacross all payers.Practice Transformation: Enablingprovider readiness and encouraging5
practice transformation to support creation of a more integrated system of care management andcare coordination for Vermonters.Health Data Infrastructure: Supporting provider, payer, and State readiness to participate inalternative payment models by building an interoperable system that allows for sharing of healthinformation to support optimal care delivery and population health management.Evaluation: Assessing whether program goals are being met.Program Management and Reporting: Ensuring an organized project.For detailed information about the Vermont Health Care Innovation project, please visit the followinglink: www.healthcareinnovation.vermont.govPlease see the VHCIP Year 3 Operational Plan for the most current information on project es/hcinnovation/files/Resources/Vermont Year 3 OperationalPlan 11.02.2015.pdfIn particular, bidders should review pages 59 – 61 in the Year 3 Operational Plan which shows a detailedlogic model for the project. All bids should reflect an understanding of the major VHCIP projectstrategies with the associated milestones and metrics as depicted in the logic model.VHCIP Evaluation OverviewTerms of the federal SIM grant require two evaluations: one conducted by the federal government and astate-led evaluation conducted by the state. The federal evaluation is longitudinal, summative andcomparative across states. The SIM federal evaluation baseline annual report can be downloaded /SIM-Round1-ModelTest-FirstAnnualRpt 5 6 15.pdfVHCIP State-led Evaluation is focused on activities that facilitate continuous improvement andevaluation of Vermont-specific pilots and innovations. The evaluation has two primary goals:1. Provide timely feedback to inform corrections in the implementation and operation of VHCIPsponsored-initiatives, and2. Generate actionable recommendations to guide Vermont state-leadership’s decisions to scale-upand diffuse VHCIP-supported initiatives.Vermont monitors its progress towards project goals and does rigorous continuous improvement by sharinginformation through a diverse set of vehicles including VCHIP work groups, multi-community learningcollaboratives, stakeholder symposiums, public presentations, and regional community collaboratives. VHCIPcontinuous improvement activities help to inform SIM programmatic decision-making, facilitate sharedlearning across the project, and directly support quality improvement efforts at the regional, community, andorganizational levels.A primary source for SIM continuous improvement information is metrics results – the SIM Core measure set,the Shared Savings Program measure sets, a select sub-set of PCMH measures, and the RTI federal evaluationmeasure set. Other important sources include risk assessments, subject matter experts, surveys, and internalpayer data analytics. Via the above varied means, continuous improvement information is regularly shared6
with administrators, ACOs, providers, payers, advocates, community leaders, and consumers. This helps keepSIM on track to achieve project goals and milestones, and informs any course corrections as needed.The three major areas of work outlined in this RFP will enhance Vermont’s existing State-led Evaluationactivities and actively support State-led evaluation goals. The key areas of work are:(1) Conduct a State-led Evaluation Study. Implementation of a mixed-methods, cross-sectionalstudy collecting primary data on three stakeholder-identified focus areas: care integration, use ofclinical and economic data for performance improvement and payment reform incentives.(2) Provide Evaluation Findings. Collection of secondary data from across VHCIP including metricresults, survey results, pilot evaluation results, and results from the State-led Evaluation Studyand analyzing/integrating them into clear, cogent and cohesive reporting that provides actionablerecommendations to State leadership on whether and what VCHIP-supported initiatives, and/orbest practices within initiatives, should be scaled-up and diffused.(3) Create and Assist in Implementing a Learning Dissemination Plan. The Plan should includedissemination of findings from the State-led Evaluation Study and overall State-led Evaluationresults. The contractor will work collaboratively with Vermont on implementation of the plan.2.Schedule of EventsQuestions and AnswersAny Vendor requiring clarification of any section of this RFP or wishing to comment or take exception to anyrequirements or other portion of this RFP must submit specific questions in writing no later than November 25,2015 by 1:00 pm. Questions may be e-mailed to or sent through the mail to: Janet Richard, Green MountainCare Board, 89 Main Street, Montpelier, VT 05620. At the close of the question period a copy of all questionsor comments and the State's responses will be posted on the State’s web site http://gmcboard.vermont.gov/RFP.Every effort will be made to have these available as soon after the question period ends, contingent on the numberand complexity of the questions.Bidder’s ConferenceThere will be a bidders’ conference call on November 30, 2015 at 10:00am. The conference callnumber is: 1-877-273-4202 and the participant number is: 2252454.Any change to the interpretation of the bid documents resulting from conference will be posted on the State’swebsite http://gmcboard.vermont.gov/RFP3.Scope of WorkState-led Evaluation StudyResearch Questions7
The following research questions will guide the VHCIP State-led Evaluation Study. The questions areorganized into three themes identified as high priority by VHCIP and GMCB leaders: Care Integration,Use of Clinical and Economic Data to Promote Value-Based Care, and Payment Reform.Care Integration. Integrated care is a key feature of many SIM activities, and a major activitycontributing to the goals of improving patient experience, improving population health, and reducing theper capita cost of health care. The majority of health spending is driven by patients with multipleconditions, multiple providers, and complex care needs. Nationally, there is a growing literature thatdefines frameworks for care integration and coordination, and recommends measures for assessing itseffectiveness. The focus on care integration is meant to be broad to capture patient-focused, careintegration/coordination activities performed by clinical and psychosocial providers.Across Vermont, care integration and coordination supported by the SIM grant takes a variety of forms,including, for example, identifying, reaching out to, and offering enhanced services to vulnerablepopulations at risk of admission to a nursing home; coordinating care for patients with particular diseasesacross a spectrum of social service and medical providers; improving care transitions to avoid hospitalreadmissions; and building on activities of existing community care teams. These models vary, butunderstanding the features of each that are most effective is critical to guide scaling up of care integrationand coordination.The following research questions will inform Vermont in directing SIM activities in this area: What are key examples of care integration approaches being tested/implemented across the state?What are the key characteristics of each approach in the sites that are studied, and how do theyvary in evidence base, design, setting, focus, resource utilization, and cost, and in comparison tonational care models?What evidence is available to demonstrate effectiveness of each approach? How solid is theevidence? What are the key lessons learned from each?What environmental and organizational features enhance care integration approaches? Whatfeatures result in barriers?Based on resources, cost, and perceived success, which appear to be most suitable for scaling up?What information do health care providers (physicians, nurses, care coordinators, social workers,others) need from other provider/care settings in order to provide high quality, coordinated andintegrated care? How available, timely and high of quality is this information? How are sharedclinical plan data used and shared?Work on the Care Integration theme should incorporate perspectives from the field on how integrated caremodels are building from services, programs and models that already exist in local communities, as wellas partnerships between clinical and non-clinical providers.Use of Clinical and Economic Data to Promote Value-Based Care. Data play a pivotal role inVermont’s efforts to transform its health system through VHCIP. Various project activities use clinicaland cost data in different ways: to inform providers, for internal and external monitoring of populationhealth data, for quality improvement, for payment, and to identify opportunities for efficiency. Clinical8
and cost data are shared with various audiences and come from a variety of sources including VHCURES,automated extracts from EMRs, and manual abstraction of medical records. This data-basedcommunication occurs in an environment that places numerous competing demands on providers,including tracking an ever-changing regulatory environment, running a business, providingcompassionate, coordinated care and complying with a long list of reporting requirements. Examples ofsuch data include: regular reports sent to providers with information to identify high cost conditions andtarget outreach and education; cost information regarding hospitalizations and hospital readmissions;services where utilization and spending vary across regions or providers, thus identifying opportunitiesfor gaining efficiency; and quality metrics that inform clinical care.However, data is not always perceived by providers as interpretable or actionable. The way in whichproviders interpret, trust, and use data is important to know in order to provide necessary content in auser-friendly format. For this theme, the contractor will visit practices to examine the process ofproducing, communicating and sharing data in support of transformation, as well as how these data arereceived, understood and applied by providers. The research questions outlined below will guide theevaluation for this theme: What data are being communicated, by whom, how are they being communicated (and throughwhat intermediary structures) and for what purposes are they being communicated? What assistance or support is provided to those intended to use data? How are data being received, understood and applied? Are the right data being communicated? What do providers perceive as most and least useful about the processes and data shared? Whatelements are most and least useful to improve patient care and practice efficiency? Do the datacontain information that providers want and think they can make use of? Are data serving HSAlevel local needs? How could the content or communication mode of the data be modified to make it coincide moreclosely with provider needs and allow effective provider responses? What data-related burdens or redundancies do providers/practices cite?Work on this theme will incorporate inquiry into how providers monitored value and performance prior toSIM, whether/how health outcomes data at the community level impacts practice patterns, and the processby which providers learn and respond to results from measures communicated to them.Payment Reform and Financial Incentive Structures. In the early phases of VHCIP implementation,physicians are operating in a system which simultaneously employs multiple—and likely intersecting—payment models and financial incentive structures. These models may include capitated, fee-for serviceand/or shared savings payments. As VHCIP accelerates Vermont’s health system transformation, thevariety of payment models and incentives confronting providers is likely to become yet more complex,adding additional models and incentives even while fee-for-service payment remains in place for somecare. For this theme, the following research questions will guide the project:9
Under what financial and non-financial incentive structure(s) do providers practice in Vermont?Are providers aware of the incentive structure under which they practice? If so, how do providersview the current incentive structure(s) under which they practice? Why? What changes, if any, have taken place in the way providers practice as a result of these incentivestructures? How does payment reform impact care integration, coordination, and providercollaboration?How do attitudes toward incentives and changes providers have made in practice (if any) differacross provider types (primary care, specialty care), practice sizes (solo, small and large group),and ownership (hospital-owned vs independent)?Are there non-financial provider incentives that influence patient care, quality, and providercollaboration?What further adaptations at the practice and provider level do providers anticipate in the transitionto next generation payment models, such as shared savings with downside risk, episode-of-carebased payment, and global budgeting? What additional support or technical assistance doproviders anticipate needing in making this transition? Work on this focus area will incorporate inquiry into whether and how payment reform impacts thepractice of preventive medicine, and whether and how payment models are driving care integration.MethodologyThe State-led Evaluation Study design will be mixed-methods and cross-sectional. Primary tasks includequalitative site visits at strategically selected sites and two quantitative provider surveys.Site VisitsSites will be selected according to methods outlined below, and will also include a clear description of10
how each site visit is intended to inform VHCIP initiative scalability recommendations.The contractor will complete 20 in-person site visits in early 2016. Each trip will involve from three tofive visits to different sites (e.g., a physician practice, Community Health Team office, ACOadministrative office, Unified Community Collaborative meeting) identified as relevant to the state-ledevaluation. Site visits will be supplemented by 10 additional hour-long phone conferences with moderatepriority sites or sites the contractor are not able to schedule for in-person visits.The specific sites to be visited or scheduled for phone conferences will be identified through the followingthree-step process:Environmental Scan. The contractor will collect and review Vermont-specific information related to eachof the three research themes. For the care coordination/integration theme, for example, the contractormight identify, collect and review materials from the published and grey literature that are related in anyway to care integration in Vermont. Conversations with VHCIP leaders or other individuals with expertiserelated to any of the three research themes will be combined with review of relevant documents.Example Activities for Environmental Scan by Theme11
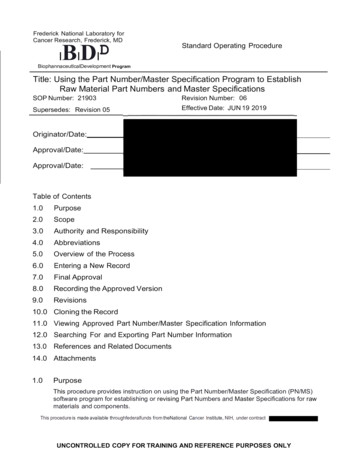
FocusUse of Data ThemeCare Integration/CoordinationPayment ReformDocumentReviewGMCB WebsiteGMCB WebsiteGMCB WebsiteVHCIP Quality andPerformance MeasuresWorkgroup materialsVHCIP Care Models and CareManagement websiteVHCIP Payment ReformWorkgroup materialsInterim reports from sub granteesACO meeting notescollected by the contractorand documents distributed atACO meetingsPubMed/Google searches forpublished/gray literaturePubMed/Google searches forpublished/gray literaturePubMed/Google searchesfor published/gray literaturePossibleKeyInformantsVermont MedicalAssociationPat JonesRichard SluskyAmy Cooper, HealthfirstMary Kate Mohlman/Blueprint CHTleadersVermont Association of Hospitalsand Health SystemsPat JonesBistate Primary Care AssociationACO leadersACO leadersVCCI/DVHAVermont Care Network/Vermont CarePartnersDevelop a preliminary list of sites. Based on interviews with VHCIP leaders and the environmental scan,the contractor will develop a preliminary list of sites to consider. Where there is doubt as toappropriateness of a site the contractor will err on the side of inclusion and formally assess its suitabilitylater, as summarized below. The preliminary site visit list will be shared with VHCIP leaders in order toassess if any essential sites have been omitted or whether any sites known to be unsuitable have beenincluded.Identify a final set of sites to be visited. The contractor will review the preliminary list of sites and selecta final set of candidate sites based on the following criteria: Relevance to multiple research themes: The contractor will favor sites where the contractor canconduct discussions that are relevant to more than one research theme. For example, the contractorwould favor a primary care practice that has an innovative care management mo
BIDDERS' CONFERENCE CALL 11-30-2015 at 10:00 am PROPOSALS DUE Revised 12-11-2015 by 1:00 pm DATE AND TIME OF BID OPENING Revised 12-11-2015 at 2:00 pm LOCATION OF BID OPENING Green Mountain Care Board 89 Main Street City Center, 2nd Floor Montpelier VT 05620 SELECTION NOTIFICATION Revised 12-15-2015 WORK START DATE Revised 1-22-2016