Transcription
OLAOFFICE OF THE LEGISLATIVE AUDITORSTATE OF MINNESOTAEVALUATION REPORTSubstance AbuseTreatmentFEBRUARY 2006PROGRAM EVALUATION DIVISIONCentennial Building – Suite 140658 Cedar Street – St. Paul, MN 55155Telephone: 651-296-4708 Fax: 651-296-4712E-mail: auditor@state.mn.us Web site: http://www.auditor.leg.state.mn.us
Program Evaluation DivisionEvaluation StaffThe Program Evaluation Division was createdwithin the Office of the Legislative Auditor (OLA)in 1975. The division’s mission, as set forth in law,is to determine the degree to which state agenciesand programs are accomplishing their goals andobjectives and utilizing resources efficiently.James Nobles, Legislative AuditorTopics for evaluation are approved by theLegislative Audit Commission (LAC), a16-member joint, bipartisan commission. Thedivision’s reports, however, are solely theresponsibility of OLA. Findings, conclusions, andrecommendations do not necessarily reflect theviews of the LAC or any of its members.A list of recent evaluations is on the last page ofthis report. A more complete list is available atOLA's website (www.auditor.leg.state.mn.us), asare copies of evaluation reports.The Office of the Legislative Auditor also includesa Financial Audit Division, which annuallyconducts an audit of the state’s financial statements,an audit of federal funds administered by the state,and approximately 40 audits of individual stateagencies, boards, and commissions. The divisionalso investigates allegations of improper actions bystate officials and employees.Joel AlterValerie BombachDavid CheinJody HauerAdrienne HowardDaniel JacobsonDeborah JunodCarrie MeyerhoffJohn PattersonJudith RandallJan SandbergJo VosJohn YunkerThis document can be made available in alternativeformats, such as large print, Braille, or audio tape,by calling 651-296-8976 Voice, or the MinnesotaRelay Service at 651-297-5353 or 1-800-627-3529.E-mail: auditor@state.mn.usReports of the Office of the Legislative Auditorare available at our web site:http://www.auditor.leg.state.mn.usPrinted on Recycled Paper.Photo Credits:The photographs on the Substance Abuse Treatment report cover were provided courtesy of PDPhoto.org, flickr.com,OHS Health and Safety Services, Inc., and St. Anthony’s Health Center.
OLAOFFICE OF THE LEGISLATIVE AUDITORState of Minnesota James Nobles, Legislative AuditorFebruary 2006MembersLegislative Audit CommissionSubstance abuse does great harm to individuals, families, and society. While some types oftreatment may mitigate the harm, research shows that not all treatment is effective.Our evaluation found that Minnesota needs stronger leadership to help ensure that effectivetreatments are more widely available. The Department of Human Services should foster thedevelopment of effective treatment options, particularly in parts of the state that areunderserved. In addition, the department should more closely monitor local decisions thatplace people in publicly-funded treatment to better ensure that appropriate services are beingused.We found that many chemically dependent prisoners have not received any treatment duringor after their time in prison. Thus, we recommend that the Department of Corrections workwith the Legislature to develop more treatment opportunities for prisoners. We alsorecommend that the department work with local corrections agencies to more effectivelyplan for inmates’ post-prison treatment needs.This report was researched and written by Joel Alter (project manager), Valerie Bombach,and Kelly Lehr. During our evaluation, we received full cooperation from the Departmentof Human Services, Department of Corrections, Department of Public Safety, SentencingGuidelines Commission, and county human services and corrections agencies.Sincerely,James NoblesLegislative AuditorRoom 140 Centennial Building, 658 Cedar Street, St. Paul, Minnesota 55155-1603 Tel: 651/296-4708 Fax: 651/296-4712E-mail: auditor@state.mn.us TDD Relay: 651/297-5353 Website: www.auditor.leg.state.mn.us
Table of ContentsPageSUMMARYixINTRODUCTION11.BACKGROUNDKey TermsCommunity-Based Treatment in MinnesotaPrison-Based Treatment in Minnesota337112.PREVIOUS RESEARCH ON TREATMENT EFFECTIVENESSGeneral ObservationsResearch on Community-Based TreatmentResearch on Prison-Based Treatment171719313COMMUNITY-BASED TREATMENT: USE ANDAVAILABILITYDepartment of Human Services’ RoleCounties’ Use of Substance Abuse TreatmentChemical Use AssessmentsAvailability of Substance Abuse Treatment3536374154COMMUNITY-BASED TREATMENT: OUTCOMES ANDPROGRAM OVERSIGHTAddressing Individual NeedsLength of TreatmentProgram Completion RatesReadmissions to TreatmentExternal Reviews of Treatment Programs7171737778815.TREATMENT FOR PRISONERS: USE AND AVAILABILITYAssessment PracticesParticipation in Treatment While in PrisonParticipation in Treatment After Release From Prison858588936.TREATMENT FOR PRISONERS: OUTCOMESProgram Completion RatesCriminal Recidivism Following TreatmentRelapse Rates Following Release From Prison9797100108LIST OF RECOMMENDATIONS111AGENCY RESPONSES113RECENT PROGRAM EVALUATIONS1174
List of Tables and nitions of Chemical Abuse and Dependency in Minnesota Rules4American Psychiatric Association Criteria for Substance Dependence5Services in Community-Based Treatment Programs7“Levels of Care” in Community-Based Substance Abuse Treatment11Characteristics of Persons Admitted to Community-Based Treatment,1995 and 200412Chemical Dependency Programs in Department of CorrectionsInstitutions, January 200614National Institute on Drug Abuse’s “Principles of Effective Treatment” 23Utilization of Publicly-Funded Treatment, 2003-0438Select Counties’ Treatment Referral Practices for Consolidated ChemicalDependency Fund Clients, 2003-0440Required Topics for Consideration in Rule 25 Assessments44Local Corrections Directors’ Perceptions of Rule 25 Assessments45Examples of Differences in Counties’ Substance Abuse AssessmentInstruments47Assessment Results of Clients Authorized for Publicly-FundedTreatment, Select Counties, 2003-0449Client “Dimensions” that Substance Abuse Treatment ProvidersMust Assess50Licensed Substance Abuse Treatment Programs, 2000-0554Local Corrections Directors’ Views Regarding Treatment Availability,by Level of Care56Local Corrections Directors’ Views Regarding Treatment Availabilityfor Certain Offender Groups57Local Corrections Directors’ Views on the Availability of TreatmentRelated Services60Number of Counties with All Treatment Admissions Provided Outsideof Clients’ Counties of Residence, by Level of Care61Consolidated Chemical Dependency Treatment Fund Eligibility63Local Corrections Directors’ Preferences for Greater or Lesser Useof Certain Treatment Approaches73Average Duration of Publicly-Funded Treatment for Treatment“Completers,” 200474Local Corrections Directors’ Preferences for Changes in TreatmentProgram Duration76Projected Length of Prison Time for Persons Entering Prison, 200490Client Completion Rates for Prison-Based Substance Abuse Programs,200499
viiiSUBSTANCE ABUSE TREATMENT6.26.36.4Reoffense Rates of Chemically Dependent Prisoners Released in 2002by Program Participation104Reoffense Rates of Chemically Dependent Prisoners Released in 2002,by Gender and Age107Relapse Rates of Prisoners and Others Who Completed SubstanceAbuse Programs in 2002110Figures3.13.24.14.24.36.1State Appropriations (in Millions) for Consolidated ChemicalDependency Treatment Fund, FY 2000-06Financial Responsibility for Publicly-Funded Substance AbuseTreatmentAverage Length (in Days) of Completed Treatment per Admission,2000-04Number of Prior Treatment Episodes for Persons Who CompletedCommunity-Based Treatment in 2004Average Number of Violations per Licensed Program Reviewed,2003-05Recidivism Rates of Chemically Dependent Prisoners Released in20026465758084102
SummaryMajor Findings: Stronger stateleadership andoversight areneeded toimprove theavailability andeffectiveness ofsubstance abusetreatment inMinnesota.Broad claims—positive ornegative—about the effectiveness ofsubstance abuse treatment aremisleading. Research has producedmixed evidence, with some studiesshowing that certain types oftreatment can achieve positive clientoutcomes, while others have littleevidence of effectiveness. (pp. 1821) The Department of Human Serviceshas not provided enough oversight ofcounty practices to ensure that clientsare placed in appropriate treatment,nor has it done enough to foster thedevelopment of sufficient treatmentoptions to effectively meet clients’needs statewide. (pp. 36, 46, 55-62) Despite uniform placement criteria,there is wide variation in counties’use of publicly-funded substanceabuse treatment for low incomepersons, and the treatment clientsreceive depends partly on where theylive. (pp. 37-41) Inmates who complete substanceabuse treatment programs in prisonhave lower overall arrest andconviction rates following releasethan (1) inmates who complete shorteducation programs, and (2)untreated inmates. However,Minnesota prisons do not haveenough capacity in their substanceabuse treatment programs to serve allof the inmates who need treatment.(pp. 92, 103-105) Few inmates deemed chemicallydependent by prison staff enroll intreatment upon release from prison,which partly reflects inadequateplanning by state and localcorrections officials to addressinmates’ post-prison treatment needs.(pp. 93-94)Key Recommendations: The Department of Human Servicesshould (1) strengthen its oversight oflocal assessment and referralpractices; (2) develop strategies toincrease the availability of effectivetreatment options; (3) improveplacement decisions by providingcounties with more information ontreatment program outcomes andquality; and (4) assess options forimproving the equity of state lawsgoverning county obligations to payfor treatment costs. (pp. 50, 68, 69,82) The Department of Correctionsshould (1) develop a strategy forimproving the post-release outcomesof chemically dependent inmateswho do not complete treatment inprison; (2) present the Legislaturewith a plan for ensuring that moreoffenders receive the treatment theyneed during and after prison, and (3)work with local agencies to improvepost-release substance abuse plansfor individual inmates. (pp. 95, 96,108)
xSUBSTANCE ABUSE TREATMENTReport SummaryState policysupports the useof substanceabuse treatment,although evidenceabout treatmentoutcomes islimited.State policy supports the use oftreatment for individuals withsubstance abuse problems. Forexample, state law says that “theinterests of society are best served byproviding persons who are dependentupon alcohol or drugs with acomprehensive range of rehabilitativeand social services.”1There were nearly 42,000 admissionsof Minnesota residents to substanceabuse treatment in 2004, and 55 percentwere publicly-funded. The main sourceof public funding was the ConsolidatedChemical Dependency Treatment Fund.State appropriations for this fund haveincreased in recent years (reaching 63million in fiscal year 2006), but the2003 Legislature discontinued fundingfor persons with household incomesabove the federal poverty line.Effectiveness Studies Show MixedResults, And Information OnMinnesota’s Community ProgramsIs LimitedBroad claims that treatment is effectiveor ineffective are misleading. There aremany forms of substance abusetreatment, of various lengths andintensities, provided to persons withdifferent needs, and implemented withvarious degrees of skill. Nationalresearch has produced a mix of positiveand negative findings regarding theeffectiveness of substance abusetreatment. A limited number of studieshave isolated the impact of treatmenton clients, apart from other variables.Studies have demonstrated the potentialfor certain counseling-based programsto reduce clients’ chemical use andimprove their social functioning, basedon comparisons to persons who did notundergo treatment or persons in othertypes of programs. Also, there havebeen favorable outcomes for some1Minnesota Statutes 2005, 254A.01.other approaches, such as maintainingheroin addicts on methadone for aperiod of time and having primary careprofessionals conduct briefinterventions with problem drinkers.But there is still much to learn aboutwhich treatments work best in variouscircumstances. There are also certainsubgroups of clients, such asadolescents and methamphetamineusers, for whom there has been alimited amount of rigorous research.The Department of Human Servicesshould develop an inventory of theapproaches used in Minnesota’streatment programs so that it can ensurethat there are appropriate, effectiveplacement options for clientsthroughout the state.In general, research has shown thatpersons who complete their treatmentprograms or remain in programs forlonger periods tend to have betteroutcomes. In Minnesota, 60 percent ofpersons who entered publicly-fundedtreatment in 2004 “completed” theirprograms, while 31 percent left“without staff approval.” The NationalInstitute on Drug Abuse has suggestedthat treatment should generally last forat least 90 days, and there is a growingconsensus that many chemicallydependent persons need extendedperiods of services, even if some areprovided at low levels of intensity.However, the duration of manytreatment episodes in Minnesota isshorter than 90 days, and the averagelength of treatment has been declining.State regulations have variousprovisions that are intended to ensurethat clients receive individualizedtreatment, but many local correctionsand human services officials told usthat programs need to be moreeffectively tailored to meet individualclients’ needs. For example, 96 percentof the directors of community-basedcorrections agencies favored strongeremphasis by substance abuse treatmentprograms on addressing clients’ mentalhealth needs.
SUMMARYCounties are the“gatekeepers” ofMinnesota’spublicly-fundedchemical healthprogram, and theDepartment ofHuman Servicesshould moreclosely monitortheir assessmentand referralpractices.xiLegislators have expressed someconcern about repeated placements ofclients into community-basedtreatment. We found that, amongpersons over age 30 who weredischarged from publicly-fundedtreatment in 2004, 37 percent had noprior episodes of treatment inMinnesota since 1995 and 22 percenthad only one episode, while 20 percenthad at least four prior episodes. Thus,some clients experience frequentreadmissions, but this is not the norm.Existing data do not conclusively showwhether Minnesota’s treatmentprograms are effective. However, theDepartment of Human Services shouldprovide counties and tribes with betterinformation to help them judgeprogram outcomes and quality,including information on programs’client completion rates, clientreadmission rates, compliance withstate regulations, and peer reviews.Use Of Community-BasedTreatment Reflects SignificantVariation In Program AvailabilityAnd Local Referral PracticesPublic funding pays for the substanceabuse treatment of persons who meetstate-prescribed financial and clinicaleligibility criteria. Despite uniformcriteria, there are wide variations in thecounties’ use of publicly-fundedtreatment for low income persons, andthe treatment clients receive dependspartly on where they live. For example,the average number of adult admissionsin 2003-04 to publicly-fundedtreatment per 1,000 adult residents inpoverty ranged from 22 in KittsonCounty to 168 in Mahnomen County.The range among counties in the TwinCities area was from 53 in DakotaCounty to 129 in Anoka County. Inaddition, some counties made most oftheir placements to outpatienttreatment, while other counties reliedmuch more on other types of care.To some extent, these differencesreflect variations in assessmentpractices. Counties and AmericanIndian tribes are “gatekeepers” inMinnesota’s chemical health system,assessing residents and makingreferrals to publicly-funded treatment.Some counties are much more likelythan others to find the clients theyassess to be chemically “dependent”(rather than the less serious diagnosisof chemically “abusive”), and the typesof programs to which clients can bereferred depends partly on thisdetermination. Also, local agencies usea variety of assessment instruments,which differ in how thoroughly theydocument clients’ underlying problems.The Minnesota Department of HumanServices is required by law to monitor“the conduct of [substance abuse]diagnosis and referral services,” but ithas not done in-depth reviews of localpractices for several years. Thedepartment should (1) provide localagencies with information on “bestpractices” in substance abuseassessment, including model protocolsfor assessment of adults andadolescents, and (2) initiate ongoingcompliance monitoring of localassessment and referral practices.Variations in treatment referrals alsoreflect the uneven availability oftreatment programs around the state,and the department should develop astrategy for addressing gaps intreatment services. About 51 percent ofpublicly-funded admissions totreatment in 2004 were at programsoutside of the client’s home county.Local corrections and human servicesofficials expressed concerns about theavailability of treatment in halfwayhouse and “extended care” settings, aswell as treatment and related servicesfor adolescents, persons with dualdiagnoses of mental illness andchemical dependency, persons withcognitive limitations, andmethamphetamine users.In addition, local corrections officialstold us that criminal offenders’
xiiSUBSTANCE ABUSE TREATMENTfinancial eligibility for publicly-funded,community-based treatment hasaffected whether these offenders enrollin treatment. Ineligibility for publicfunding could be one reason whynearly half of the offenders sentencedto probation in 2003 for felony-levelsubstance use or possession did notenter community-based treatment priorto sentencing or during the periodimmediately following their sentencingdate or release from jail.Prisons Need More TreatmentBeds And Better Planning ForServices Following ReleaseMost chemicallydependentinmates do notcompletetreatment inprison or whenthey are released.Persons imprisoned for drug-relatedoffenses now comprise 25 percent ofMinnesota’s prison population, up from9 percent in 1990. In addition, a highpercentage of other types of offendersin Minnesota’s prisons have histories ofsubstance abuse. All but two ofMinnesota’s prisons have programs forinmates with substance-relatedproblems. Some are treatmentprograms, lasting 6 to 12 months andproviding a variety of group andindividual counseling, while others aresubstance abuse education programs,lasting three months or less andoffering no individual counseling.Among chemically dependent inmatesreleased from prison in early 2004, only25 percent participated in substanceabuse treatment prior to release (17percent completed a program andanother 9 percent started a program butdid not complete it). Another 30percent participated only in short-termeducation programs prior to release.Many inmates do not serve enoughtime in prison to complete a treatmentprogram, but there is also a shortage oftreatment beds to meet the needs ofinmates with substance use problems.Among chemically dependent inmatesreleased from prison in 2002, amajority had arrests or convictions fornew offenses within three years(including 36 percent with arrests orconvictions for drug or alcohol crimes).Prisoners who completed the ChallengeIncarceration Program (a boot campwith a chemical dependency treatmentcomponent) and other prison-basedtreatment programs generally had lowerpost-release recidivism rates than thosewho failed treatment or completedshort-term education programs. It isunclear whether the lower recidivismrates for treatment completers wereattributable to treatment rather thanother factors, such as the offenders’motivation to change.When inmates near their dates ofrelease from prison to correctionalsupervision in the community, theDepartment of Corrections andsupervising agency develop plans forhelping the offenders succeed in thecommunity. But prison “release plans”have contained little direction regardingpost-release chemical use assessmentsand programming. In addition, lessthan 10 percent of chemicallydependent inmates released from prisonto community supervision in 2004entered community-based treatment inthe six months following their release.The Department of Corrections shoulddevelop a strategy for improving theavailability of treatment in prisons andensuring that chemically dependentoffenders receive the treatment theyneed following release.
IntroductionAbuse of alcohol and other drugs has widespread impacts. It often leads toreduced personal productivity, harmful health effects, and damaged personalrelationships. In addition, substance abuse can have broader social impacts,contributing to child abuse, welfare dependence, and criminal activity. Thus,interventions that reduce substance abuse may serve important public purposes.Accordingly, Minnesota law declares that it is the state’s policy to providechemically dependent people with rehabilitative services.1But policy makers have asked many questions about substance abuse treatment inrecent years. In April 2005, the Legislative Audit Commission directed ouroffice to evaluate substance abuse treatment in Minnesota communities and stateprisons. Our evaluation addressed the following questions: Are substance abuse treatment programs effective? Is there adequate treatment for chemically dependent criminaloffenders sentenced to prison and probation? To what extent do counties vary in how they assess and referindividuals to community-based substance abuse treatment, andshould policy makers be concerned about these variations? Do public agencies use reasonable methods to determine individuals’needs for substance abuse treatment?We used existing data from the departments of Human Services, Corrections, andPublic Safety to assess outcomes for persons who entered treatment programs.For example, we examined the extent to which chemically dependent inmateswho participated in prison-based treatment programs were arrested and convictedof new crimes following release from prison. For community-based treatment,we examined measures such as program completion rates and rates ofreadmission to treatment following treatment discharge. We recognize thatfactors other than treatment may have contributed to the outcomes we observed,so we also examined findings from previous studies of substance abusetreatment.2We looked at treatment use and availability in Minnesota, including variationamong counties. Local human services agencies play a key role in treatment12Minnesota Statutes 2004, 254A.01.We did not conduct “experimental” research, in which persons are randomly assigned to variousprograms or to no treatment at all. Such studies provide more definitive evidence of treatment’simpacts.
2SUBSTANCE ABUSE TREATMENTplacement decisions, and we conducted site visits to eight counties and contactedsome others by phone.3 Publicly-funded treatment for low-income personsaccounts for more than half of Minnesota’s substance abuse treatmentadmissions, so we gave particular attention to its use. We looked at variationamong counties in the share of treatment costs they bear, but we did not conductan in-depth evaluation of the formula used to allocate state treatment funds tocounties.Because of the close association between substance use and crime, we alsolooked at treatment availability and use among Minnesota’s criminal offenders.Specifically, we examined the extent to which chemically dependent offendersenrolled in treatment programs in prison, after prison, and during probation.Community-based corrections agencies supervise many offenders with substanceabuse problems, so we conducted a statewide survey of the directors of theseagencies to better understand their perceptions about treatment availability andadequacy.4Chapter 1 provides background information on substance abuse treatmentservices in Minnesota communities and prisons. Chapter 2 reviews previousresearch on treatment effectiveness. The next two chapters examine communitybased treatment in Minnesota, including client placements (Chapter 3) andcertain treatment outcomes (Chapter 4). The final two chapters examine prisonbased treatment, including availability (Chapter 5) and rates of post-prisonrecidivism and relapse (Chapter 6).Finally, we often use the terms “substance abuse” and “chemical dependency”interchangeably in this report. Chapter 1 notes the diagnostic distinctionsbetween “abuse” and “dependency,” and Chapter 3 examines differences amongcounties in their diagnoses, but elsewhere in the report we do not differentiatebetween “substances” and “chemicals” or between “abuse” and “dependency.”3We did not review individual clients’ case files during our site visits, such as assessment reportsor treatment plans.4To provide probation services, each Minnesota county (1) participates in the state’s CommunityCorrections Act (CCA) and receives state funds for this purpose, (2) receives “county probationofficer” (CPO) funding from the state, or (3) obtains services from the Minnesota Department ofCorrections (DOC). We surveyed and received responses from all of the 54 directors of CCAagencies, CPO agencies, and DOC’s district offices and supervised release offices.
1BackgroundSUMMARYMinnesota law supports treatment and other rehabilitative services forpeople with substance abuse problems. The state has provided significantfunding for community-based treatment for low income persons, as well asfunding for substance abuse programs in most of the state-operatedprisons. Current state rules that define chemical “dependency” do notreflect diagnostic criteria commonly used by mental health professionals,although changes to the outdated definition are scheduled forimplementation in 2007. Alcohol remains the predominant substanceabused by people entering treatment in Minnesota, but the number ofpeople entering treatment for methamphetamine use grew dramaticallyduring the past decade.Avariety of factors contribute to chemical dependency, including socialinfluences, genetic predispositions, the nature and availability of thesubstances abused, and underlying psychological disorders.1 Substance abuseinvolves voluntary behaviors, at least initially, but it may also evolve intocompulsions and loss of control. Substance abuse treatment takes many forms,and relapses are common. This chapter provides background information onsubstance abuse treatment, and it addresses the following questions: How are substance “abuse” and “dependency” defined? What types of treatment programs are offered in community-basedand prison-based settings? What roles do Minnesota’s state and local governments play inoverseeing substance abuse treatment programs, paying fortreatment, and helping individuals access treatment services? What are the primary substances abused by persons enteringtreatment, and how has this changed in recent years?KEY TERMSSubstance “Abuse” and “Dependency”Definitions of chemical “abuse” and “dependency” are important becauseMinnesota’s administrative rules prescribe the types of publicly-funded treatmentfor which persons are eligible, based partly on whether the person is determined1George E. Vaillant, “Natural History of Addiction and Pathways to Recovery,” in Principles ofAddiction Medicine, 2nd ed., ed. Allan W. Graham and Terry K. Schultz (Chevy Chase, MD:American Society of Addiction Medicine, 1998), 295-308.
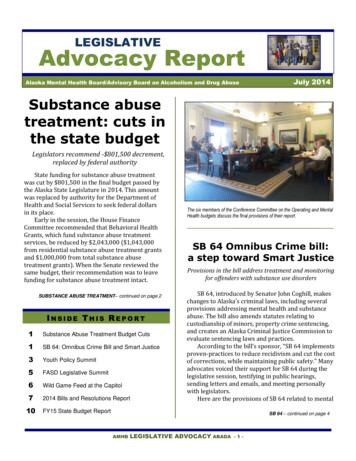
4SUBSTANCE ABUSE TREATMENTto be chemically dependent rather than chemically abusive.2 As shown in Table1.1, the rules define chemical abuse as less severe than chemical dependency.3We found that: Minnesota’s criteria for determining who is “chemically dependent”are not consistent with current professional criteria for diagnosingmental health disorders.The Minnesota rules that define “abuse” and “dependency” are based on the 1980edition of the American Psychiatric Association’s Diagnostic StatisticalManual.4 The rules require that dependency be based, in part, on evidence ofTable 1.1: Definitions of Chemical Abuse andDependency in Minnesota RulesStateadministrativerules definesubstance“abuse” and“dependency.”Chemical abuse is a pattern of inappropriate and harmful chemical use which exceedssocial or legal standards of acceptability, the outcome of which is characterized by threeor more of the following indicators: Weekly use to intoxication.Inability to function in a social setting without becoming intoxicated.Driving after consuming sufficient chemicals to be considered legally impaired,whether or not an arrest takes place.Excessive spending on chemicals that result in an inability to meet financialobligations.Loss of friends due to behavior while intoxicated.Chemical use that prohibits one from meeting work, school, family, or socialobligations.Continued use of chemicals by a woman after she has been informed that she ispregnant and that continued use may harm her unborn child.Chemical dependency is a pattern of pathological use accompanied by the physicalmanifestations of increased tolerance to the chemical or chemicals being used orwithdrawal syndrome following cessation of chemical use. “Pathological use” means thecompulsive use of a chemical characterized by three or more of the following indicators: Daily use required for adequate functioning.An inability to abstain from use.Repeated efforts to control or reduce excessive use.Binge use, such as remaining intoxicated throughout the day for at least two daysat a time.Amnesic periods for events occurring while intoxicated.Continuing use despite a serious physical disorder that the individual knows isexacerbated by continued use.Continued use of chemicals by a woman after she has been informed that she ispregnant and
3.5 Examples of Differences in Counties' Substance Abuse Assessment Instruments 47 3.6 Assessment Results of Clients Authorized for Publicly-Funded Treatment, Select Counties, 2003-04 49 3.7 Client "Dimensions" that Substance Abuse Treatment Providers Must Assess 50 3.8 Licensed Substance Abuse Treatment Programs, 2000-05 54