Transcription
New JerseySubstance Abuse Prevention and SynarSystem Review ReportAugust 4–6, 2009Fiscal Year 2009Substance Abuse and Mental Health Services AdministrationCenter for Substance Abuse Prevention
CONTENTSSYSTEM REVIEW SUMMARY .1Brief Background.2Summary of Prevention System.7Summary of Synar Program.16APPENDIX A: SUMMARY OF SYSTEM REVIEW FINDINGS.19APPENDIX B: CSAP NATIONAL OUTCOME MEASURES .32APPENDIX C: PARTICIPANT LIST FROM THE SYSTEM REVIEW .50APPENDIX D: SOURCES OF INFORMATION REVIEWED .53APPENDIX E: SUMMARY OF NEW JERSEY’S ESTIMATED FFY 2008 AND PLANNED FFY 2009SYNAR BUDGETS .58APPENDIX F: ABBREVIATIONS .60i
SYSTEM REVIEW SUMMARYThe Alcohol, Drug Abuse, and Mental Health Administration Reorganization Act (P.L. 102-321)enacted by Congress in July 1992 authorized the Substance Abuse Prevention and Treatment(SAPT) Block Grant administered by the Substance Abuse and Mental Health ServicesAdministration (SAMHSA). SAMHSA’s Center for Substance Abuse Prevention (CSAP) ischarged with providing policy and program guidance to help States 1 use and report on the20-percent primary prevention set-aside of the SAPT Block Grant. CSAP is committed toproviding support and guidance for advancing Single State Authority (SSA) substance abuseprevention systems through technical assistance (TA), expert panel meetings, national andregional conferences, training, videos, guidance documents, and other products.CSAP also supports States by conducting thorough substance abuse prevention system reviewsto examine how a State’s substance abuse prevention system is addressing State needs. Thisreport is a summary of the most recent CSAP system review for New Jersey.The system review conducted on August 4–6, 2009, examined the progress of the New Jerseysubstance abuse prevention system and Synar program in improving the substance abuseindicators and outcomes measured by SAMHSA’s National Outcome Measures (NOMs), as wellas other State-specific goals and objectives. The system review also involved detaileddiscussions with State participants concerning the State’s current capacity for using performancemanagement processes to achieve and sustain outcomes measured by the NOMs and other Statespecific outcomes. The System Review Report will help guide New Jersey in enhancing itsinfrastructure and State prevention system capacity to implement the five steps of the StrategicPrevention Framework (SPF) or other equivalent planning process and to achieve populationlevel reductions in the incidence and prevalence of substance abuse and related problems andconsequences.The review included the creation of the New Jersey “System Review Analysis” tables (appendixA), which present findings on the current strengths and challenges specific to the State’sprevention system and Synar program. The findings also identify potential areas of capacity andinfrastructure development that could further enhance the New Jersey prevention system andSynar program, either through State-supported efforts or through TA requested from CSAP.In addition to appendix A, which details New Jersey’s successes and challenges and maps outnext steps, the System Review Report contains: The State’s NOMs baseline and, where possible, data from previous years and changes inthe baseline data (appendix B) A list of participants from the system review (appendix C) A list of New Jersey’s prevention and Synar documents that were consulted inpreparation for the system review (appendix D)1In this document, the word State refers to the 50 States and the District of Columbia and to the Territories, Pacificjurisdictions, and North American tribe that receive SAPT Block Grant funds.1
System Review Summary A summary of the State’s estimated Federal fiscal year (FFY) 2008 and planned FFY2009 Synar budgets (appendix E) The abbreviations used in the System Review Report (appendix F).Brief BackgroundPrevention System Development and OrganizationThe New Jersey Division of Addiction Services (DAS) is one of eight major divisions within theDepartment of Human Services (DHS) and one of two administrative offices that handlelicensing and contract services that span the department. DHS is recognized as the social servicesauthority for the State, and DAS is recognized as the SSA for substance abuse. As such, DHS isresponsible for administration of the social services block grant; alcohol, drug, and mental healthblock grants; and other federally assisted State programs or plans. DAS plans, licenses, regulates,and monitors more than 14 million of SAPT Block Grant and State funds to contracted provideragencies that offer prevention education and early intervention services to residents in all 21counties of New Jersey. The division is also responsible for the statewide Intoxicated DrivingProgram.The director of DAS is one of three division directors who report to a Deputy Commissioner ofDHS. DAS comprises the Office of the Director; Office of Quality Assurance; Office ofTreatment; Office of Prevention and Early Intervention; Office of Research, Planning,Evaluation, and Information Systems/Technology; Office of Policy and Special Initiatives; andOffice of Administrative Services.Prevention services are provided through the Prevention and Early Intervention Services Unitwithin the Office of Quality Assurance. This unit includes six full-time staff members and ismanaged by the National Prevention Network representative. Both the SSA director and theNational Prevention Network representative are new to the SSA since the last CSAP preventionand Synar system review in April 2006.DAS contracts with the New Jersey Prevention Network (NJPN) to manage prevention resourcescenters in all 21 counties. DAS also funds statewide substance abuse services delivered by localprevention providers and a variety of agencies. These providers conduct the StrengtheningFamilies Program and evidence-based curricula, as well as other statewide special projects, suchas outreach and services to members of the military and their families.The Governor’s Council on Alcoholism and Drug Abuse (GCADA), established by thelegislature as an independent body, is responsible for reviewing and coordinating New Jersey’sefforts regarding substance abuse prevention, treatment, research, education, and evaluation.GCADA funds the Municipal Alliances to prevent alcoholism, a network of 540 communities inNew Jersey dedicated to a comprehensive and coordinated effort against alcoholism and drugabuse.The Alliances implement policies to reduce alcoholism and drug abuse at the municipal level andallocate funding, including moneys from mandatory penalties on drug offenders, to the CountyAlliances. These funds are funneled through the County Alliances to the member municipalitiesto support appropriate county and municipal alcohol and drug abuse education and public2
System Review Summaryawareness activities. Each county is charged with establishing a Local County AdvisoryCommittee responsible for identifying local needs; developing, planning, and funding prioritiesfor the county; and providing rehabilitation services for abusers of alcohol and drugs.Additional multiagency councils responsible for substance abuse prevention in New Jerseyinclude the Prevention Coordinating Council (a subcommittee of the Governor’s OversightCommittee for Safe Streets and Neighborhoods) and the Strategic Prevention Framework-StateIncentive Grant (SPF SIG) Advisory Council.Although DAS coordinates and collaborates with a variety of organizations at the municipal,county, and State levels to carry out its policies, programs, and practices, most of theserelationships are State-level partnerships and appear to focus primarily on those partners withinDHS and the State Epidemiological Outcomes Workgroup (SEOW). The SEOW membershipincludes not only State partners but also representatives from the counties, colleges, andcommunity agencies. It is not clear how these groups interact and whether there is some overlapin role and function of the groups. Although State agencies and local partners may share somegoals, they do not appear to share a universal vision or mission statement for providingprevention services, and each convening venue has its own set of guiding principles andoverarching themes. While these principles are not necessarily in conflict with one another, theyalso are not uniform or constant across the various collaborations.For example, there is little coordination with the Enforcing Underage Drinking Laws and Safeand Drug-Free Schools grants, which DAS does not monitor or oversee. DAS could enhance itsleadership by strengthening relationships with State agency partners beyond those engaged in theSEOW and DHS, such as the agency that is responsible for the Enforcing Underage DrinkingLaws grants.Historically, GCADA, DAS, and the County Authorities have collaborated to carry outPrevention Unification as a comprehensive, integrated, and cohesive planning strategy forcommunity-based prevention services. The roles of GCADA, the Municipal Alliances, thePrevention Coordinating Council, the SPF-SIG Advisory Council, and the SSA are overlapping,and coordination is not maximized. The New Jersey prevention system would be strengthened ifDAS and GCADA worked more closely together to coordinate resources and provide strong,cohesive leadership to the prevention system.Other State- and local-level collaborative efforts include the Department of Education’s SchoolSurvey Workgroup, the Governor’s Blueprint for Safe Streets and Neighborhoods, the City ofTrenton Department of Health and Human Services, the City of Newark Anti-Gang Task Force,and the Center for Healthy Schools and Families.DAS is responsible for the prevention and treatment of substance abuse, and supports therecovery of individuals affected by the chronic disease of addiction. The vision and missionstatements for DAS embrace the full continuum of prevention, early intervention, treatment, andrecovery support services. Addiction services are considered a component of a public healthparadigm, where early detection and assessment protocols begin with client engagement; promptand effective treatment is provided, meeting a standard of care; all substance abuse and mentalhealth programs are competent to screen, assess, and address co-occurring mental health and3
System Review Summarysubstance abuse disorders; prevention measures are employed throughout the life cycle andcontinuum; consumers are active, informed, and educated participants in their own recovery;collaboration occurs regularly with mental health and primary health care systems; the use ofbest practices is widespread, including the latest pharmacotherapeutic responses; and thefinancing system promotes client outcomes.DAS promotes a risk and protective factor model and data-driven collaborative planningprocesses as the foundation for Prevention Unification within DAS prevention efforts.Unification establishes funding priorities based on a comprehensive, integrated, and cohesiveplanning strategy for community-based prevention services.DAS is exploring opportunities to better integrate prevention, treatment, and recovery in acontinuum of care, while at the same time ensuring that the 20-percent set-aside for prevention isused to fund primary prevention services. DAS is encouraged to consider how to transition froma current focus of using SAPT Block Grant funds for indicated populations, to a strategy thatsupports more universal or environmental primary prevention strategies, policies, and programsthat are designed to impact population-level change.DAS recently began targeting prevention services to at-risk populations that have not historicallybeen served, including lesbian/gay/bisexual/transgender/questioning youth and militarypersonnel and their families. The division has worked toward strengthening culturally competentprogramming by allocating funds to provide technical assistance and training in this area to allDAS-funded prevention providers.Despite the many new and stable prevention initiatives that DAS has undertaken in recent years,the Governor and State legislators may be forced to consider program cuts, hiring freezes, joblayoffs, tax increases, and using funding heretofore dedicated to substance abuse to shore upNew Jersey’s anticipated budget deficit. New Jersey’s economy, like that of many States, isexperiencing a significant downturn, and the Governor’s Office anticipates State budget deficitsof 6.1 billion for 2009 and 8.8 billion (29.9 percent of the budget) for 2010.Although New Jersey is the fifth-smallest State in the Nation, it is also one of the most ethnicallydiverse. In 2000, Caucasians made up 72.6 percent of the population, 13.6 percent of thepopulation was African-American, 5.7 percent was Asian, 0.2 percent was Native American, andthose of mixed heritage or not reporting race made up 7.9 percent of the population. Hispanics,who may be of any race, were 13.3 percent of the population and were primarily of Puerto Ricanor Cuban origin. There are no federally recognized tribes within New Jersey.New Jersey lies between New York City and Philadelphia, in the heart of a highly urbanizedarea, and it is the second most urbanized State, behind only California. It is the most denselypopulated State, with an average population density of 1,176 per square mile in 2000. NewJersey is the only State in which all 21 counties are officially classified as “metropolitan” by thecensus. New Jersey has ready access to the markets and a dense system of highways, railroads,tunnels, and bridges that connect it with New York City and Philadelphia. All of these factorsinfluence substance abuse patterns and transportation.4
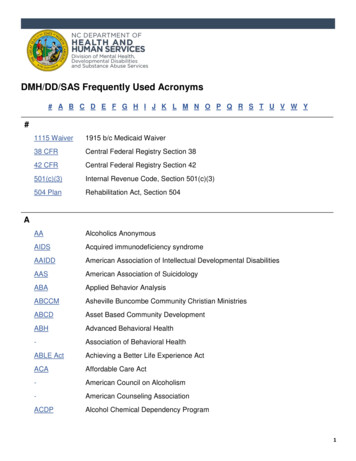
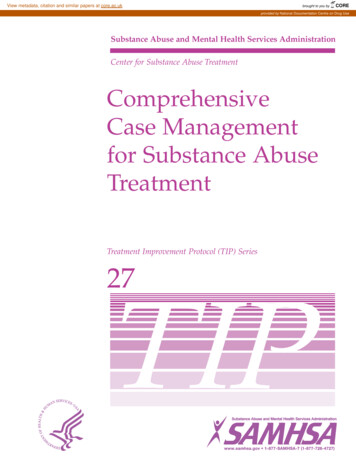
System Review SummaryThe New York–New Jersey region is the Northeast United States’ center for narcotics trafficking, both a gateway and a marketplace. The area is ideal for importation of drugs through twomajor international airports and several domestic airports; two major railroad complexes and thehundreds of miles of subway tracks; extensive waterfront with various points-of-entry, includingthe Port of New York, the third-largest port in the country; and a complex network of highways,bridges, and tunnels bringing more than a billion people into New York City each year.The metropolitan area offers numerous opportunities and avenues to convert illicit funds into aform unidentifiable by the banking system and more readily acceptable in world trade. Inaddition, the area’s multicultural population allows ethnic-based drug organizations to operatewithin widely recognized ethnic enclaves without arousing suspicion. Despite the fact that crimein New York City and New Jersey has decreased dramatically, much of the remaining crime isdirectly attributable to the drug trade.The importance of tourism—epitomized by Atlantic City, which in 1978 became the site of thecountry’s first gambling casino in modern years outside of Nevada—provides another potentialsource of substance abuse and consequences.State Substance Abuse TrendsAccording to the 2006 National Survey on Drug Use and Health (NSDUH), New Jerseyexperiences higher rates of 30-day alcohol use, compared with national rates, across all agegroups. Compared to the national average, 30-day alcohol use among youth ages 12–17 in NewJersey is more than 3 percentage points higher, use among 18- to 25-year-olds is more than 5percentage points higher, and use among those ages 26 and older is 5.5 percentage points higher.Despite State rates being higher than the national averages, New Jersey’s 30-day alcohol useamong those 26 and older declined 1.9 percentage points to 59.8 percent between 2002 and 2006(see figure on the next page). Rates for those younger than 26, however, have recently increased.For those 18–25 years of age, 30-day alcohol use increased by 4.2 percentage points to 66.6percent from 2005 to 2006. In the same time period, 30-day alcohol use increased for 12- to 17year-olds by 0.9 percentage points to 19.7 percent.NSDUH data also show that the 30-day use rates of marijuana and other illicit drugs for each ofthe age groups are slightly less than the national rates. The percentage of adults smokingcigarettes declined 3.8 percentage points to 21.3 percent, much lower than the national averageof 26.7 percent, and the percentage of alcohol-related traffic fatalities increased 8 percentagepoints to 44 percent. Attitudinal measures for risk related to binge drinking and marijuanasmoking are also close to the national averages for both youth and adults.With current prescription drug use rates close to the national rates, DAS is seeking to partnerwith the Drug Utilization Review Board to proactively monitor prescription drug use in an effortto prevent the prescription drug use trends that are appearing in other States.5
System Review SummaryOutcome Measure: Percentage who reported having used alcoholduring the past 30 days by 8%2003‐20042004‐200518‐2519.7%2005‐200626 and olderData collected by NSDUH, as well as data collected by the SEOW, indicate that alcohol is by farthe primary drug of choice for all age groups in the State, with marijuana and other illicit drugsclose behind. These data also reflect four major trends in the State: increased rates of alcohol useamong those ages 12–17 and 18–25, increased treatment admissions, and increased drug-relatedarrests for those 18 and older.Heroin is the most prevalent illicit drug of abuse in the New Jersey area. Data provided by DASreveal that the percentage of 18- to 25-year-olds in the State using heroin is more than twice thenational average.Cocaine also continues to be a popular drug in New Jersey. Crack, which remains readilyavailable throughout the State, is particularly prevalent in lower income communities throughoutthe State.Mexican drug-trafficking organizations are increasingly transporting larger quantities ofMexican methamphetamine to parts of the New York/New Jersey High Intensity DrugTrafficking Area, using their established transportation networks. This area also continues to bethe most significant heroin destination and distribution center in the country. In addition toDominican and Colombian drug-trafficking organizations, Mexican drug-traffickingorganizations and street gangs, Asian criminal enterprises, and Jamaican drug-traffickingorganizations, which control crack and marijuana distribution in certain areas, operate in theregion. Drug distribution, street-level sales, transport, and attendant violence remain high.Although DAS identified alcohol and drug use among 18- to 25-year-olds as the priority problemfor the SPF SIG, it has not yet set this as a priority for State- and local-level prevention efforts.DAS is urged to use available data to review statewide substance abuse trends and develop Statelevel prevention priorities that are based on data and that will affect population-level change.Synar Program Development and OrganizationA Memorandum of Understanding exists between DAS and the New Jersey Tobacco Age-ofSale Enforcement (TASE) program to implement the State’s Synar program. TASE is a program6
System Review Summaryof the Comprehensive Tobacco Control Program (CTCP) at the Division of Family HealthServices of the Department of Health and Senior Services, which is responsible for tobaccoprevention and control programming across the State. While DAS is ultimately responsible forSynar, TASE takes the lead in implementation.DAS and TASE partner to draw the Synar sample. TASE tobacco inspectors then conduct therandom, unannounced inspections and file summonses in the municipalities in response to anyviolations that occur. This is the first year TASE has conducted inspections without the supportof local health departments. Because of funding reductions, TASE was required to consolidate itsfunding and use staff to conduct inspections rather than contract with local health departmentsfor this task. The Memorandum of Understanding between TASE and DAS has not been updatedto include the coverage study requirement, and TASE does not have the funding for this work.Since the last system review in 2006, TASE has seen significant funding reductions, and inresponse, the agency has been restructured. CTCP was funded through 30 million in MasterSettlement Agreement funds, but in FFY 2004, these funds were redirected and the agency’sbudget was cut to 11 million in tobacco tax revenue. Reduction in funds continued throughoutthe years, and for the upcoming FFY, CTCP has a budget of 7.5 million. Just as contracts withlocal health departments for inspections have been eliminated, funding for merchant educationand media campaigns also has been eliminated.Description of Trends in the State’s Retailer Violation RateNew Jersey reported a baseline retailer violation rate (RVR) of 44.4 percent in FFY 1997 (table).Since that time, the State has not been found out of compliance with the Synar requirements. InFFY 2003, the State achieved a rate below the 20-percent target (15.9 percent), and the rate hasremained between 15 and 11 percent ever since.Retailer Violation Rates for Federal Fiscal Years 1997–2009 (in percent)1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009Target–35.0 28.0 26.0 25.0 24.020202020202020Reported 44.4 27.0 26.5 23.2 24.6 22.1 15.9 13.0 12.6 15.6 11.2 12.2 11.9Summary of Prevention SystemPrevention System Compliance and Compliance SupportNew Jersey is in compliance with the Federal requirement that a minimum of 20 percent ofSAPT Block Grant funds be allocated to primary prevention. In its FFY 2009 SAPT Block Grantapplication, the SSA reported intended prevention expenditures of 24.8 percent of its total BlockGrant allocation of 46,941,463 and intended expenditures of 4.1 million from State generalfunds.DAS also leverages funds from a number of other sources, including the SPF SIG, Drug-FreeCommunities grants, and alcohol beverage taxes. As New Jersey explores options to more fullyintegrate prevention, treatment, and recovery in a continuum of care, it will be necessary forDAS to continue to employ effective allocation and reporting tools to ensure that funding7
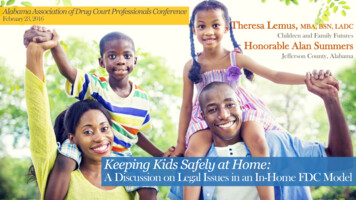
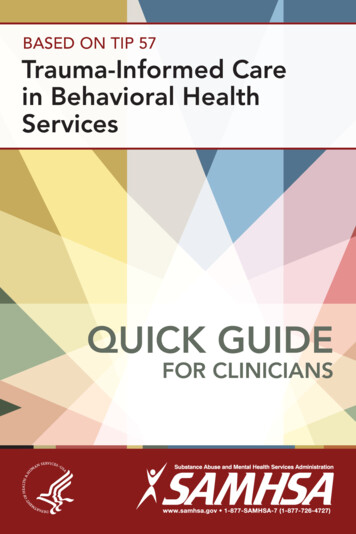
System Review Summarystreams are used as required, specifically in relation to the 20-percent set-aside for primaryprevention.As reported in the FFY 2009SAPT Block Grant application, actual expenditures inEnvironmentalFFY 2006 were distributed20.0%4.0% 6.0%Community Based Processacross all six CSAP core10.0%10.0%strategies (figure). In 2006,Alternativeshowever, similar to earlierEducationyears, more than 50 percentof funding was allocated toInformation Disseminationprevention educationProblem Identification &processes that aimed toReferral50.0%increase individual andcommunity knowledge aboutsubstance abuse prevention or to problem identification and referral strategies for youth. Inaddition, only 6 percent of SAPT Block Grant expenditures in 2006 targeted environmentalprevention strategies.FFY 2006 New Jersey SAPT Block Grant Expenditures bySix StrategiesAs reflected in the State’s NOMs data, almost 50 percent of persons receiving preventionservices through SAPT Block Grant funds are 25–64 years of age; approximately 33 percent ofprevention services are provided to school-age children. A breakdown of expenditures for 2006shows that almost 70 percent of funded strategies are selected or indicated prevention strategies.These are primarily program-focused or individually focused prevention services, includingresources for the Strengthening Families Program, which targets the adult at-risk population inneed of parenting skills. This allocation leaves approximately 30 percent of funding available foruniversal strategies.Many current environmental and universal prevention strategies are funded though State generalfunds and the SPF SIG. This situation raises concerns about sustainability. Given the currenteconomic downturn, State general funds are in jeopardy, and strategies funded by the SPF SIGmay be threatened when that program ends if alternative sources of funding are not found.The SSA also reported that 100 percent of its programs employed evidence-based practices inboth 2005 and 2006 and that all programs were within cost bands in 2005 and 2006.The New Jersey data system, the Prevention Outcomes Management System (POMS), currentlyis not able to collect data related to environmental strategies, only program-level data. Therefore,NOMs data reported for numbers of persons served by individual-based strategies and thoseserved by population-based strategies are identical. DAS requests TA to develop a process thatwill allow New Jersey prevention providers to more accurately report data relating to thedevelopment and delivery of environmental strategies.8
System Review SummaryPrevention System Infrastructure and OperationsStrategic PlanAlthough New Jersey does not have a single comprehensive strategic prevention plan thatincludes all substance abuse prevention-related funds and stakeholders, it does have a number ofdisparate State prevention plans that could be used to advance a single statewide plan. Theseplans include: New Jersey Comprehensive Statewide Master Plan for Alcoholism, Tobacco and OtherDrug Abuse, December 2008—developed by GCADA and including program objectivesand funding amounts that could be aligned with data to inform development of acomprehensive strategic plan New Jersey State Strategic Plan for Substance Abuse Prevention—developed for the SPFSIG, based on the SEOW report State of New Jersey Executive Summary: A Strategy for Safe Streets andNeighborhoods—a three-tiered approach to reducing crime, juvenile delinquency, andgang involvement that does not specifically address substance abuse issues, but targetsfor prevention activities some risk and protective factors for selected and indicatedpopulations that are also relevant to substance abuse prevention.It is not clear how the Comprehensive Statewide Master Plan and the State Strategic Plan arelinked and whether Block Grant-funded prevention efforts are included in either plan.Additionally, it is not clear whether the SSA participated in the development of the plans orwhether the plans are used to develop subrecipient resource allocation and contract requirements.There are no goals, objectives, or outcomes in the Statewide Master Plan.DAS is strongly encouraged to provide leadership to develop a unified strategic plan for itsprevention system based on needs assessment data across the lifespan. The statewide strategicplan could be used to guide the development of local strategic plans, which include statewidepriorities as well as priorities identified from local data. The needs of culturally disparatepopulations, such as Native American, Hispanic, and Asian populations, should be addressed inthe strategic prevention plan. This plan should include the agency’s prevention vision, mission,priorities, goals, objectives (risk and protective factors influencing the behavior), baseline data,and outcomes to more effectively focus prevention resources. This approach would incorporate alogic model planning process, such as SPF, and provide a foundation and direction for workforcedevelopment training and TA needs, data system development, and evaluation systemdevelopment.Prevention FundsNew Jersey is committed to funding substance abuse prevention as demonstrated by thesubstantial allocation of State general funds, alcoholic beverage tax funds, and dedicated fundsfrom the Governor’ budget. The SSA reported in its FFY 2009 SAPT Block Grant applicationthat the percentage of total expenditures for prevention intended for 2009 is a 7.6-percentincrease over FFY 2006 expenditures. Prevention funding increased from 24 percent in 2005 to28.3 percent in 2006, even with a reduction in overall Block Grant funding from 47,251,367 in2005 to 46,768,909 in 2006.9
System Review SummaryDAS reports that New Jersey currently receives more than 46 million for substance abuseprevention as follows: Division of Addiction Serviceso Block Grant: 11,645,976o Other Federal: 4,186,000 (SPF SIG, other)o State: 4,060,000Department of Education––Federal: 9,776,639 (Safe and Drug-Free Schools funds)(This funding has been cut from the President’s budget for the coming year.)Department of Health and Senior Services (not including CTCP)––State and Federal: 3,066,555 (Master Settlement Agreement funds)Law and Public Safety––State and Federal: 5,746,863Military and Veterans Affairs––Federal: 350,500Governor’s Council on Alcoholism and Drug Abuse––State: 10,400,000 (fines andpenalties to drug offenders)Drug Free Communities Support Programs (nine)––Federal: 1,125,000STOP Grants (three)––Federal: 150,000.In October 2006, New Jersey was awarded 10,465,000 in SPF-SIG funding. Administered byDAS, the funding is intended to be used over a 5-year period to promote and provide outcomebased prevention services to the citizens of New Jersey. The grant is designed to build p
The Alcohol, Drug Abuse, and Mental Health Administration Reorganization Act (P.L. 102-321) enacted by Congress in July 1992 authorized the Substance Abuse Prevention and Treatment (SAPT) Block Grant administered by the Substance Abuse and Mental Health Services Administration (SAMHSA). SAMHSA's Center for Substance Abuse Prevention (CSAP) is