Transcription
Transforming Dispatch and CrisisResponse Services: MeetingChallenges with InnovationPresented by:Ruth Simera, MEd, LSWPeggy Heil, LCSWAbigail Tucker, PsyDBen MelendrezRobert SmutsSimon PangMarch 2, 2021 2:00 - 3:30 pm ET
Welcome and IntroductionDr. Robin S. EngelPrincipal InvestigatorAcademic Training to Inform Police ResponsesUniversity of Cincinnati2
Opening RemarksCornelia SigworthAssociate Deputy DirectorBureau of Justice AssistanceOffice of Justice Programs3
Today’s ModeratorMike Hatch, MPASenior Project AssociateAcademic Training to Inform Police ResponsesPolicy Research Associates, Inc.4
DisclaimerThe preparation of this webinar was supported by Grant No. 2020-NT-BX-K001awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistanceis a component of the Department of Justice’s Office of Justice Programs,which also includes the Bureau of Justice Statistics, the National Institute ofJustice, the Office of Juvenile Justice and Delinquency Prevention, the Officefor Victims of Crime, and the SMART Office. Points of view or opinions in thisdocument are those of the authors and do not necessarily reflect the officialpositions or policies of the U.S. Department of Justice.5
Introducing Today’s PresentersRuth H. Simera, MEd, LSW Ruth is the Executive Director of the Coordinating Centers ofExcellence in the Department of Psychiatry at Northeast OhioMedical University. Ruth was previously the Director of the Ohio Criminal JusticeCoordinating Center of Excellence (CJ CCoE), and now oversees thethree centers of excellence, including the CJ CCoE, the BestPractices in Schizophrenia Treatment (BeST) Center, and the OhioProgram for Campus Safety and Mental Health. Under the CJ CCoE, Ruth oversaw the statewide CIT disseminationand technical assistance activities and the Ohio Sequential InterceptMapping initiative. Previously, Ruth worked 26 years in communitymental health, three years in juvenile justice, and ten years asinstructor in Applied Conflict Management at Kent State University.6
Introducing Today’s PresentersPeggy Heil, LCSW Margaret “Peggy” Heil works in the Office of Research andStatistics in the Colorado Division of Criminal Justice at theDepartment of Public Safety. She is a licensed clinical social worker with over 35 years ofexperience in criminal justice behavioral healthadministration, service delivery, and research. In her current position, she promotes effective interventionsfor justice-involved individuals with behavioral health needsby facilitating policy and research development through thecoordination of behavioral health-related grants andparticipation on multiple behavioral health-related boardsand committees.7
Introducing Today’s Presenters Abigail S. Tucker, PsyD is a licensed psychologist in Denver, Colorado. Dr. Tucker currently serves on the Colorado Commission Criminal andJuvenile Justice, Colorado Department of Youth Services CommunityBoard Northeast Region, and supports local and state taskforce effortson matters related to the nexus of justice system and behavioralhealth.Abigail Tucker, PsyD Dr. Tucker serves as Adjunct Faculty at Nova Southeastern University inboth their College of Psychology and for the Fischer College ofEducation and Criminal Justice. The focus of her ongoing research and practice includes emergencyresponder psychology, the intersection of behavioral health and socialjustice, and suicide prevention.8
Introducing Today’s PresentersBen Melendrez Ben has served with the Albuquerque PoliceDepartment (APD) since 2003 and is currentlyassigned as a detective in the Crisis Intervention Unit. He has spoken on the topic of mental health andofficer wellness at several national conferences andworks closely with the Behavioral Sciences unit atAPD. Before becoming a detective, he served for 14 years asa police officer. Prior to joining the police department, Ben served inthe U.S. military.9
Introducing Today’s PresentersRobert Smuts Robert Smuts is the Deputy Director of the SanFrancisco Department of Emergency Management,overseeing the city’s PSAP. He has held this positionfor seven years. Prior to this role, Robert was Chief AdministrativeOfficer for the City of New Haven, CT for seven years.10
Introducing Today’s Presenters Simon Pang is the Section Chief of CommunityParamedicine for the San Francisco Fire Department(SFFD). He has been in the fire service for 25 years as afirefighter, paramedic, and rescue captain.Simon Pang His interests are finding innovative, cross-boundary,collaborative solutions to fill gaps in the system ofcare.11
Training of CITDispatch TrainersRuth H. Simera, MEd, LSWExecutive DirectorCoordinating Centers of ExcellenceNortheast Ohio Medical University
Coordinating Centers of Excellence (CCOE)13
Ohio History TimelinesMemphis CITorientationand trainingTraining inAkronTraining inToledoCriminalJustice CCOE1999May 2000June 2000May 200114ACMIC @SupremeCourt of OhioJune 2001Ohio CITConsensusDocumentFirst NationalCITConferencein Columbus,Ohio20042005
Key Criminal Justice CCoE Partners National Alliance on Mental Illness of Ohio Ohio Department of Mental Health and Addiction Services Law Enforcement Liaison – CIT Coordinator Ohio Department of Public Safety - Office of Criminal Justice Services andOSHP Ohio Department of Rehabilitation and Correction Stepping Up Ohio Peg’s Foundation15
Key Criminal Justice CCoE Partners (cont’d) Retired Ohio Supreme Court Justice Evelyn Stratton CIT Coordinators Group Ohio Chapter of the Association of Public Safety Communications Officials(APCO) Ohio Office of the Attorney General & OPOTA Crisis Intervention training block (24 hours) Task Force on Criminal Justice & Mental Illness16
CIT Organization in Ohio17
Historic Crisis Intervention Team Training Information09/01/2020Full-time Ohio Peace Officers OnlyEquivalence of OfficersTrained since 200021% 16% - 20%11% - 15%6% - 10%1% - 5%0%PR18Peer Review
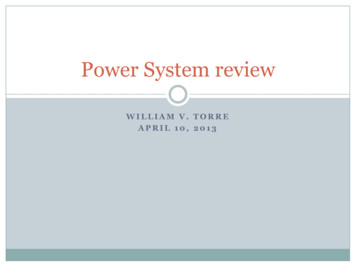
CIT in Ohio by Law Enforcement AgenciesMay 2000 - August 2020100%20 Counties75% - 99% 29 Counties50% - 74% 28 Counties20% - 49% 11 Counties19
Ohio 2015 Strategic Plan – 4 Key Strategies#3 - Prioritize training for 911 call-takers and dispatchers in all Ohio communities20
Training of CIT Dispatch Trainers1. Many models exist for CIT dispatch/call-taker training – we model an 8-hour version2. Training must meet local needs3. Participants should be experienced in the local CIT program: coordinators, trainers, CITofficers, mental health providers, etc.4. Focus on the content and provide resources – model some of the presentations5. Discuss specific needs of 911 workers6. Express goal for participants to implement training in their community21
Agenda1. Welcome and Introductions Presented by CJ CCoE Introduction to CIT Big Sky Video Manual Overview22
Agenda (cont’d)2. What does an officer need? Presented by Officer (Futo) Identifying CIT Calls Collecting and Sharing Information23
Agenda (cont’d)3. PTSD, TBIs and Trauma 24Presented by Officer KnolesPast dispatch experienceBrain developmentDefining traumaEffects of traumaPersonal experience
Agenda (cont’d)4. Mental Illness, IntellectualDisabilities, Substance Use Disordersand Medications Overview Presented by Psychiatrist Adult and Youth5. De-escalating & Active Listening Skills Presented by Officer (Futo)25
Agenda (cont’d)6. Consumer Perspective Presented by a community memberwith lived experience7. Suicidal Callers Presented by a mental healthprovider or community mentalhealth board representative Facts vs. Myths Prevalence Goals of call-taker Intervention strategies26
Agenda (cont’d)8. Scenario-based Training Co-facilitated by law enforcementand mental health trainers Alternative approaches to skilldevelopment and practice9. Self-care and Resources Presented by Officer Knoles Trained Peer Support27
Dispatcher/Call-Taker Training of CIT Trainers2017-201882 participants37 counties28
Thank You!Ruth H. Simera, MEd, iha9bq5jnuu56/AACiweKrxhi HMfRFc3Q073ya?dl 0
Colorado Justice Mental HealthCollaboration Program:Dispatch/Crisis ServicesCollaborationPeggy Heil, LCSWBehavioral Health SpecialistColorado Division of Criminal JusticeAbigail S. Tucker, PsyDSHE Consulting, LLC
Sequential Intercept ModelSelected area of focus: Intercept 0 & 1 Greatest potential to prevent criminal justice involvement 911 is more likely to be called than the state crisis line 2020 Policy Research Associates, Inc.31
Lean Process Mapping – Public Safety Answering PointAdministrators (911 Dispatch)Goal: Decrease the number of individuals withmental health disorders who end up in jail by default32
Colorado's Statewide Crisis Services andCrisis Support Line Colorado developed crisis servicesincluding a statewide crisis line inresponse to the Aurora theatershooting in July, 2012 The state is divided into 7 crisis servicesregions that align with the state’sMedicaid regions33
Expanding Stakeholders on a Shared Vision Add behavioral health response as fourth category along with lawenforcement, fire, and emergency medical services post-911 Integrate behavioral health services as part of emergency response Finish with a connection (intentionally broad to include behavioralhealth, physical health, case management, family/faith-based supports,housing, peer support services, crisis services, etc.)34
Expanding Stakeholders on a Shared Vision (cont’d)New stakeholders added: Advocacy groups Individuals with lived experience Regional accountable entities Colorado Consortium for Prescription Drug Abuse Prevention Colorado Office of Behavioral Health Co-Responder Program35
Where are we now?CommittedStaying true to the aim of aStatewide Justice &Behavioral HealthCollaboration36AdvancingHolding strong to the shared visionto shift the culture and addBehavioral Health as 4th category ofEmergency Response, integratebehavioral health services inemergency response and finish witha connectionDevelopingDeveloping a Process Map &Menu: Cultivating Colorado InformedJustice & Behavioral Health Practices forcommunities to select, pilot, duplicateand share
Pilot ModelDevelop Model Process to select mostappropriate Best Practice Model911 Call involving Emotional Distress(Track: Nature Code, # to Crisis, # back to 911)Standardize data for needs assessment &program evaluationDetermineGeneral Law Enforcement OfficerGeneral EMSEMS ClinicianCADCo-Responder Team (LE MH)Disposition CodeCIT – Crisis Intervention Team (LE)Psychiatric Emergency TechnicianCrisis Mobile Unit37Crisis Line dataCrisis Line call only (hot & warm line)Number of Agencies the ECC SupportLocally Available Intervention ResourcesExplore OptionsStaffing mental health provider or peersupport person in ECCFirst Responder asks if there is a PsychiatricAdvance Directive – Who do they want tohave it?App for First Responder to help individualobtain support servicesDrop off facility options
Process Mapping & Concept Development:Powered by Stakeholder Feedback SIM Intercept 0 Continue to support Colorado crisis system Expand behavioral health care access Fight stigma with awareness & trainings38
Process Mapping & Concept Development:Powered by Stakeholder Feedback (cont’d) SIM Intercept 0 & 139 Opi-rescue Treatment Mapping PSAP/Public Safety Telecommunicators (PST) standards and training Develop PSAP/PST Codes/Workflow Integration behavioral health at PSAP
Process Mapping & Concept Development:Powered by Stakeholder Feedback (cont’d) SIM Intercept 1 Opi-Rescue treatment engagement push notification Psychiatric Advanced Directives accessible to emergency health &behavioral health care providers Current pilot: PST triage to crisis line/98840
Next Steps Peer visit to Houston (virtually) Monitor pilot of 911 dispatch to Colorado crisis support line Support development of PSAP codes that support policy evaluation andresource need identification Explore options to increase treatment mapping and treatment engagementat Intercept 0 & 1as well as post-crisis Create and propose to stakeholders a Colorado Informed Practices ProcessMap & Menu for Justice & Behavioral Health Collaboration41
Thank You!Abigail S. TuckerTucker.Abigail@gmail.comPeggy HeilPeggy.Heil@state.co.us
Albuquerque PoliceDepartment’s Intellectual andDevelopmental DisabilityTraining for TelecommunicatorsBen MelendrezDetectiveAlbuquerque Police Department
Telecommunicator IDD Training BreakdownA. State law mandates 20 hours mental health training1. Eight hours of Mental Health First Aid (MHFA)2. Eight hours of APD-created curriculuma. Includes 1 hour of IDD/Autism spectrum instructionb. NAMI peer panel with individuals with lived experience3. Four hours of scenario-based traininga. One scenario includes a caller living with Autism Spectrum Disorder44
Telecommunicator 1-hour IDD class Define IDD and provide examples Prevalence and etymology of IDD Communication difficulties strategies with scenario reinforcement Destigmatize the population (meeting people with IDD)45
Albuquerque Police Department’s View on IDDCurriculum Identified a need for IDD specific training Department works closely with local IDD providers The need and implementation of IDD curriculum has been supported bythe top tiers of APD leadership Implemented in all phases of officers/telecommunicators career fromacademy to annual training46
Thank You!Detective Ben Melendrez
Transitioning 911 Response:San Francisco’sStreet Crisis Response Team (SCRT)Pilot ProgramRobert SmutsDeputy DirectorSan Francisco Department of Emergency ManagementSimon PangSection Chief of Community ParamedicineSan Francisco Fire Department
San Francisco (SF) Background SF is the second densest major US city, with 880,000 people in 47 square miles SF is unified City/County, and SF Department of Emergency Management (DEM) PSAPhandles Police, Fire, Sheriff and EMSo All operators are cross trained for call-taking and all dispatch roles Annually, SF PSAP handles 1.2m incoming calls; and dispatches 415,000 police,125,000 EMS and 32,000 Fire incidents (not counting “On View” incidents from units inthe field) SFFD handles 80% of EMS incidents requiring a transport unit, with the remaining20% handled by two private ambulance companies49
Program Background Mental Health SF legislation (late 2019)o Includes “street crisis response team” Mayor London Breed’s commitment to police reform (Summer 2020)o Includes call for behavioral health experts to respond to non-violent incidents onthe street Community Planning Processes for Police Reformo Several parallel planning tracks engaging related issues Street Crisis Response Team jointly planned by SF Department of Public Health and SFFire Department, with significant support by SF Department of EmergencyManagement (which runs SF’s PSAP)50
Key Elements of Crisis Systems51Someone tocallSomeone torespondMust be wellpublicized andeasy to useWell trained,trauma-informedand culturallycompetentA place to goTrue “no wrongdoor” servicesthat arewelcomingLinkage toongoing careStaff to supportwarm handoffs tostabilizingservices
Street Crisis Response Team Goal and StrategiesGoal: Provide rapid, trauma-informed response to calls for service to peopleexperiencing crisis in public spaces in order to reduce law enforcement encounters andunnecessary emergency room use.1. Identify 9-1-1 calls that will receive behavioral health and medical response ratherthan law enforcement response.2. Deliver therapeutic de-escalation and medically appropriate response to person incrisis through multi-disciplinary team (paramedic behavioral health clinician peer).3. Provide appropriate linkages and follow up care for people in crisis, includingmental health care, substance use treatment, and social services.52
Program Details Team Staffingo Community paramedic (on rig)o Behavioral health clinician (on rig)o Peer health worker (on rig)o Multi-disciplinary team dedicated to linkages and follow up care coordination With a paramedic, the team operates within the EMS system. SCRT responds to anarrower incident definition than crisis assistance programs in some othercommunities (CAHOOTS, for example) San Francisco is exploring other alternative response teams with a focus on lessacute incidents53
Street Crisis Response Team Deployment and LinkageEmergency, identified by self orconcerned bystanderDept of Emergency Management9-1-1 call triageNon-behavioral healthissueBehavioral health incident,violent (e.g. weaponinvolved)Behavioral health incident in publicsetting*, nonviolent – ADULT only*SFPD or SFFD/EMSSFPD/CITStreet Crisis Response Team***Phase 1**During active shift and available for new calls in specifiedcatchment area54Resolve crisis in thecommunityLinkage to crisisfacility or socialserviceFollow up supportto link to care
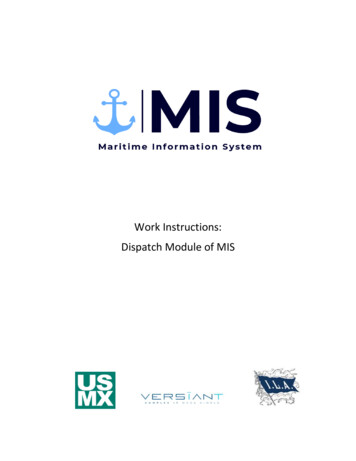
Phase 1 Dispatch WorkflowNote: Call-takers will no longercreate 800-B’s, which will all bereplaced by 800ST. 800-B willresult on channel, so PD units willnot see a change.Initial Questioning DeterminesCall Fits 800 Definition –“Mentally Disturbed Individual”Is the person a threat tothemselves or others; is there aweapon?NYGetting from Point A to Point B:25-A-0 is canceled; PDdispatched on 800-BCall interrogated using policekey questions; entered as800ST tied-call800-BN25-A-0Call sent for dispatch800-A – Police dispatchedYCall dispatched as normal unless SCRTcancels 800-B before unit on sceneSCRT Dispatched; 800-B ischanged by HS to 800-I, whichis rebroadcast by PD channelYHS has SCRT review – is calleligible?N55Is this during hours ofoperation?25-A-0 canceled; 800-Bdispatched; entry made in25-0-A with reason for 22Is SCRT available?YSCRT AvailableNCall pendsPolice arrive on scene whilepending and cancel 25-A-0when they clear the run The incidents SCRT is focusing on used tobe police calls coded “800” with a B-levelpriority. As the SCRT phases in, dispatch jointlycreates a medical call for them and apolice call. One agency will respond, anddispatch will cancel the other. Call is processed using police dispatchprotocols. SCRT unit reviews text of therun to determine if it qualifies. Instead of retraining 200 dispatch stafffor tweaks, SCRT staff can makeadjustments in dispatch eligibility forPhase 1.
Phasing Up Phase 1 launched 11/30/20, starting with one team business hours M-Fand gradually adding hours, weekends and a second team Phase 2 planned for 3/31/21o Switch from using police call-taking protocol to Emergency MedicalDispatch protocol using ProQA from Priority Dispatch No longer send up a police incident SCRT and/or EMS response to all callso Six teams, operating 24/7 on or soon after Phase 2 date56
Challenges and Initial Experience Challengeso Data baselineo Implementation bumpso Flexibility v Clarity Initial outcomes and impressions Planning for Phase 2 (and beyond)57
Looking Ahead Partnership development Community input, including people with lived experience of a behavioralhealth crisis Target implementation timelineFirst team live byNovember 30, 2020Two teams live byJanuary 31, 2021 Continuous process improvement58Six total teams live byMarch 31st, 2021Future expansionspending pilot evaluation
Thank You!Robert SmutsSimon PangSpecial thanks to Angelica Almeida, PhD; and Lauren Brunner, MPH, for programvisualization slides, as well as their leadership planning and implementing the StreetCrisis Response Team program.
Downloadable ResourceDownload the 911 DistressedCaller Diversion Program inBroome County, New York –Webinar Supporting Document!60
Thank you forattending!Learn more about the Academic Training to Inform Police Responses ng-to-inform-police-responses
Transforming Dispatch and Crisis Response Services: Meeting Challenges with Innovation. March 2, 2021 2:00 - 3:30 pm ET. Presented by: 2 . Document. ACMIC @ Supreme Court of Ohio. Criminal Justice CCOE. Training in Toledo. Training in Akron. Memphis CIT orientation and training. 1999. May 2000.