Transcription
NewsBriefsLAM EFFECTIVE AT12 MONTHSway to use breastfeeding.toachieve contraception,.called the lactational amenorrhea method (LAM), appears tobe highly effective for 12 monthsafter delivery among women whoremain amenorrheic.Arecent study found apregnancy rate ofless than 3percentamong women using LAM for 12months. This compares favorablywith such methods as oral contraceptives, which are also about 97percent effective during a yearof use.Experts have recommendedLAM as a reliable contraceptiveapproach for six months followingdelivery anlong amenorrheicwomen who are fully or nearlyfully breastfeeding. When any ofthese conditions changes, awoman should begin using another contraceptive method toprevent unplanned pregnancy.The findings indicate thatwomen who breastfeed intensively and remain amenorrheiccan rely on lactational amenorrhea to prevent pregnancy,explains Cynthia Visness ofFHI, one of the study authors."They need to make an informed choice, though, andunderstand the degree of risk ofpregnancy," she says. "Forwomen who remain amenorrheicup'to a year, this approach givesthem more time and flexibilityin starting another method."The study followed 485women, in the Philippines.About one-third of the womenremained amenorrheic 12months after delivery. Becausemany breastfeeding women doA2NETWORKnot remain amenorrheic for aequal chance of becoming infected by their partners: Twoful year, new mothers cannotthirds of m le partners ofcount on LAM protectionlastinfected females and two-thirdsingfor that long, Visness says."The most important marker of of female partners of infectedreturn to fertility is the return of· males' contracted chlamydia.nlenses," she says "WheneverChief researcher Dr.'that occurs, a woman needs toThomas Quinn, ofNIAID'sLaboratory ofJmmunostart using another methodregulation and Johns Hopkinsimmediately."Published in the Oct. 12,University School ofMedicine,1996 issue of the British Medicalsays the equal transmission ratesJournal, the study was conducted were determined by using a new,by the Comprehensive Familysensitive urine assay to screenfor the infection. TraditionalPlanning Center, Jose FabellaMemorial Hospital in Manilacell culture tests, which wereand FHI. An earlier study, conalso given, showed higher ratesducted by the National Research among women.Institute for Fertility Control in"The old standard aboutKarachi, Pakistan, and FHI,men being resistant to chlamyfound a pregnancy rate of only 1 dia isn't true," says Dr. Quinn.percent at one-year postpartum"They should be screened just asamong those women who remuch as women. If they're posimained amenorrheic.tive, you can treat them and thatwill lower the infection ratesoverall. In the long-run, thatCHLAMYDIA RISKwill reduce the complications inwomen." Chlamydial infectionEQUAL FOR MEN,in women can lead to more seriWOMENous problems, including pelvicinflammatory disease (PID).recent study concludes thatThe study also concluded\ women and men are atthat young women are threeequal risk ofinfection fromtimes more likely to acquirechlamydia through sexual con,chlamydia than 'older women.tact. Previous studies indicated"Age is the single most imporwomen were more susceptible totant demographic variable," Dr.infection.Quinn says. Results of the studyThe study, sponsored bywere published in the Dec. 4,the U.S. National Institute of1996 issue of the Journal oftheAllergy and Infectious DiseasesAmerican Medical Association.(NIAID), examined 958 peopleover four years. Clients whovisited a clinic in Baltimore,MD, USA, and their partners,were tested for chlamydial infection using a variety of diagnostictechniques. Researchers foundthat men andwornen had an . Winter1997Since chlamydia is morelikely to be detected using thenew urine test, NIAID is recommending that the test be usedmore widely. Two versions of thetest are already available in manypartsof the world.PPFA CLINICSDROP PRE-TESTlanned pare.nthOOd Federa-.tion ofAmerica (PPFA), an.organization with family ,planning clinic affiliates throughout the United States, has eliminated its requirement for medicaltesting prior to insertion ofan intrauterine device (IUD).The National MedicalCominittee ofPPFAagreed tochange language in theorganization's guidelines from"must" to "as indicated" forblood tests and laboratory diagnosis for chlamydia and gonorrhea before an IUD is inserted,effective January 1.IUDs can now be insertedwithout any testing ifa client's,medical and personal histories'are appropriate. The change isconsistent with 1994 U.S.Agency for International'Development guidelines for developing countries, which say a routinepre-exam (a separate visit) shouldnot be required, since two visitsmay be a'barrier to IUD use-andmay expose a woman to unintended -pregnancy between thevisits. , WContinued on page 7
o0000.0.FAMII ,YHEALTH INTERNATIONAL, VOL. 17 NO.2, WINTER 1997. IN THIS ISSUEFAMILY. PLANNING AND AIDS PREVENTION. OPIN'IONOUNCE OFPREV NTION WORTHA. MILLION LlyES. ;: ' 4"REPRODUCTIVE HEALTH·RESOURCES ';.'.RISK ASSESSMENTS .SEEKTo.IMPROVE SCREENING . . 8EMERGENCY CONTRACEPTIONAS A BACKUP METHOD . EXPERIMEN ALHI". DRUGSMAYIMP' OVE PREVENTION· . 'COMMON REPRODUCT'IVE,TRACK INFECTIONS '.12.141 .·,6.SERVING CLIEN'T GROUPSSERVING YOUNG 'ADULTS REQUIRES CREATIVITY. 20. S.TDS PREGNANCIES AFFEcT 'WOMEN'S H.EALTH 24'REDUCINGTHEHIV RISK FROM .MOTHER TO INFANT ' 29DEPARTMENTS'NEWS BRIEFS· . RESO'URCES : ·2' . . 32Cover photo by'the United Natio s 'Children 'sFund (UNICEF1585OlVilas) shows a typicalfamilyin New Delhi, India. Ways to maximizereproductive health resources include the combinationoffamily planning services with appropriateSTDIHIVprevention activities.NETWORKWinter19973
Ounue of PreventionWortba Million LivesBy Peter Lamptey,MD, DrPHPHI Senior Vice President, AIDS ProgramsWillard Cates, ]r., MD, MPHPHI Senior Vice President, Biomedical Affairsince the XIth International AIDSConferencein Vancouver lastJuly,news of continued important treatment breakthroughs has raisedhopes and expectations. Researchershave reported that the new protease inhibitors, taken in combination with other AIDSdrugs such as AZT, ddC and 3TC, can reduce the amount ofHIV in infected peopleto undetectable levels. Some scientists evenspeak - cautiously - about the possibilityof eradicating HIV from infected people. Astestimony to the optimism, the popular U.S.magazine Time proclaimed Dr. David Da-iHo ofAaron Diamond Research Institute inNew York as its 1996 "Man of the Year" forhis scientific leadership in these treatmentefforts.The results from trials of a new generation of anti-HIV drugs are indeed encouraging. But the excitement over these findingshas obscured what is - and will continue tobe - our most potent weapon against thevirus: prevention. Worse still, it may undermine prevention efforts by encouraging themistaken impression that scientists havefound a "cure" for AIDS.Anyone who works in any area of reproductive health must remember the urgent and global need for effective HIVprevention strategies, and that this need willbe with us for many years to come. For thosewho work primarily with family planning,seeking creative ways to incorporate appropriate, cost-effective STDIHIV preventionactivities into their programs must continueto be a priority.l Promoting' condom useamong clients at risk of a sexually transmit7'ted disease is just one example ofhow. familyplanning providers in many countries arealready making an important contribution toHN prevention.NoREPLACEMENTAlthough powerful antiviral drug combinations will make it possible to improveand extend life for many who are infectedwith HIV, drug treatment will never replaceprevention. These therapies are alreadyproving unaffordable for poor andunderinsured North Atnelicans. The cost at least U.S. 10,000 per patient per yearguarantees that they will not be accessible tomost people with HIV/AIDS in developingcountries, where 90 percent ofall HIV infections occur.Even for those who can afford them;the drug "cocktails" are not a cure. Wedonot know how long they can keep the virusin check, and the drugs do not work for everybody. Moreover, compliance is difficult:the three drugs must b taken several times aday with more than a liter ofwater, Soine onan empty stomach and others with a high-fatmeal.
The cost and complexity of the threeveloping countries. Methods under studypaigns give people the knowledge, skills andsupport they need to prevent HN transmisdrug regimen and the remarkable ability ofinclude vaccines, microbicides, new apHN to mutate more rapidly than any otherproaches to counseling, and prophylacticsion. In Uganda, for example, the "ABC"message (abstinence, behavior change orperinatal drugs.known virus raises the specter of multiplecondoms) is reaching young people throughdrug resistance. If paPREVENTION WORKSschools, community outreach and the media,tients do not take theFHIClearly, universaland a 35 percent decrease in HN prevalencedrugs correctly, or ifaccesstoeffective,affordamongyoung women attending antenataltreatment is interruptedable antiviral therapy is abecause ofadverse sideclinics suggests a substantial reduction in newdistant goal. But the good HIV infections among 15- to 24-year-old girlseffects or a patient'snews-news that hasand women from 1990-93 to 1994-95.3inability to afford a newmade few headlines - isIn the United States, Australia andprescription, strains ofthat we can reduce theWestern Europe, HN incidence appears toHN will develop thatneed for treatment. Databe stabilizing, largely because of effectiveare resistant to many, ifshow that HN prevenprevention efforts within gay communities.not most, of the limitedtion works - and at anumber of drugs curEven while in the Rwandan refugee camps,fraction of the cost ofwhere the daily struggle for survival nladerently available. Thesedrug treatment. 2AIDS seem a distant threat, many have reresistant strains will beAs in basic and clini- sponded to prevention education by becomtransmitted to others,cal research on HN/ing more faithful to their partners.making the drug combiAIDS, years of painstakTreating sexually transmitted diseasesnations powerlessing research and practiceagainst HN even inhelps prevent HN transmission. 4 Thein prevention are begin-"people who have neverpresence of preventable STDs increases susning to pay off. For moretaken them.ceptibility to HN infection as much as ninethanadecade,publicFurther researchfold.Groundbreaking research in TanzaniaDR. PETER LAMPTEYhealth professionals andwill undoubtedly lead tohas confirmed that STD treatment can reeducators have been remore effective HN/duce HN transmission by more than 40fining effective approaches to slowing theAIDS treatments that are easier for patientspercent. This could make a big difference inspread ofHN.to take, and we must fight to make thesethe developing world, where most ofthe curWe have figured out which strategiestreatments accessible to all. One possibilityable sexually transmitted infections occur.work and how to make them culturally senis a two-tiered pricing system to make thePromoting condom use results in lowersitive, politically acceptable and econominew drug combinations affordable in develinfection rates. s In Thailand, aggressivecally feasible in sonle of the least developedoping countries. Companies that reap hugecondom promotion throughout the countryregions of the world.profits from HN/AIDS drugs in industrialand tough enforcement of condom use inWe have learned that some populations brothels led to reductions in transmission ofized countries have a moral obligation to- among them, womenwork with governments, nongovernmentalHN and other STDs.and young people - areorganizations (NGOs) and people livingSkyrocketing condomFHIparticularly vulnerablewith HN/AIDS to expand access to thesesales in countries whereand require special prolife-saving therapies.condoms could hardly begrams that address theirSupport for HN prevention researchgiven away just 10 yearsneeds. And we've foundcould pay even greater dividends. Throughago are another indicatorout how to work withof the success ofHNapplied research by HN/AIDS preventionprojects around the world, we know that the grass-roots organizationsprevention intervenwith strong communitythree main strategies ofFHI's AIDS Contions.trol and Prevention (AIDSCAP) project and ties to ensure that prevenSocial marketingtion efforts can bethe Joint United Nations Programme onprograms that makesustained.HIV/AIDS (UNAIDS) - communicationcondoms more accessibleHere is what we haveto change behavior, condom promotion andand attractive to potenimproved STD services - can reduce trans- discovered:tial users have increasedPrevention educamission of the virus. Studies sponsored bytion and communicationthe U.S. National Institutes of Healthcan reduce risky behavior.funded HIVNET (HNNetwork for EffiEducation, counselingcacy Trials) Consortium in nineand conlmunication canlinternational sites managed by FamilyDR. WILLARD CATES"Health International will identify new toolsto complement these three strategies in de-NETWORKWinter 19975
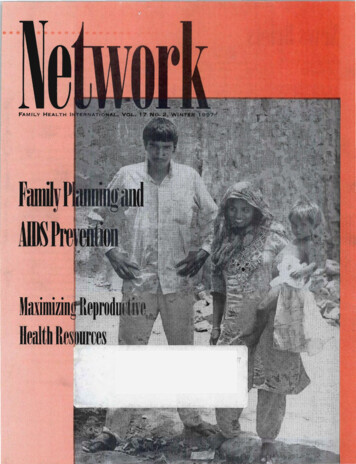
IMPACT VISUALSI GISELE WOLFSOHNHIV DRUG RESEARCH ISENCOURAGING, BUTPREVENTION REMAINS THEMOST POTENT WEAPONAGAINST THE VIRUS.PEOPLE READ LEAFLETSDURING A SOUTH AFRICANAIDS PREVEN"rION RALLY.condonl sales in countries from Haiti tounrest and an international trade enibargoBEST INVESTMENT'paralyzed Haiti, Haitian nongovernmentalEthiopia to Nepa!. In sub-Saharan Africa,Despite the success of these preventionorganizations 'valiantly continued the· preannual condom 'sales rose from less than 1strategies,and the continued elusiveness ofmillion in 1988 to more than 167 million in' ventiori effort. With support from FHI's6aneffectiveand affordable cure or vaccine,AIDSCAP Project, funded by the u.S.1995.onlyasmallpercentage of the funding for. Agency for International Developnlent,Encouraging national policy changeglobalHIV/AIDSefforts goes to preventionmakes HIVprevention possible. Adoptingthese small groups initiated effec ve prevenprograms.Yetevenwhen an effective vaction programs in workplaces, schools,policies that support rather than obstructcineagainstHIVbecomesavailable, irwillchurches a d community centers, reaching·prevention efforts is one of the most impornotbeperfect andwewillstillneed all thetant ways a government can protect its citiboth urban and rural pop lations. And inotherpreventionapproachesworkingtozens from HIV infection. In Brazil, condom .Tanzania, AIDSCAP has helped NGOsincombination.Thus,thesecombigethersales 'boomed after the government elimiabandon competition and collaborate onnation HIV prevention strategies in .prevention programs in the regions of thenated a 15 percent tariff on imported.populations are analogous to our need for.condoms. The Thai government's "100 Per- country most affected by HIV/AIDS.combination HIV treatment approaches inComprehensive HIV prevention procent Condom Policy," which Experienceconsistent condom use among sex workers,This need is now greater than ever. Ashas contributed to decreases in HIV andhas shown that combining these preventionmany as 40 milli n people will have beenSTD transmission, and has inspired similarapproaches multiplies their effectiveness,infected with HIV by the end of the decade;efforts in the Philippines and the Dominican creating a social and political environmentRepublic. Throughout the world, when gov- that supports sustained behavior change and . In some regions, entire generations will bedevastated by the disease; leaving behindernment leaders have spoken out aboutreduced risk. Just as conlbination HIVhundreds of th6usands of orphans AIDS prevention, their openness hasdent on charity and social services. As workininfectedindividuals,combinationHIVencouraged a more vigorous response to theprevention approaches have a greater impact ers in their most productive years succumbepidemic.on the virus in populations where it is preva- to AIDS and national health budgets areStrengthening indigenous AIDS prestretched thin by the rising cost of caring forlent. Family planning professionals have avention organizations is the best way tothe il , the economic fallout will strain thereach communities and sustain preventionvital role to play in this onlprehensiveapproach. .efforts. From 1991 to 1995, when political6NETWORK Winter 1997
struggling economies. of developing. .nations. These p(essures on fragile societiescan intensify political unrest and instability.If we failt() support HIV preventionwhile waiting for amedical" lagicbullet,"the consequences will be catastrophic. As weapplaud biomedical advancesinAID : re .search, we must not forget thatHrypreven-.tion remains one ofthebesti Ivestments wecan make in a healthier, more PT()ductiveand more stable world.' . ' .'Dr. Lamptey·directsUSAID'sAIDSCAP Project and Di·.Cates overseesFHI'sptl11:icipation in the NIHHIVNETp1-oject. This a11:icle'is adaptedfrom one by Dr.Lamptey and Dr. Cates that appe'aredinAIDScaptions, aperiodicalpublished by theAIDSCAP Project.4. Dallabetta G, Lagaft1, Lamptey p;.l.CatesW]r. Sexuallytransmitted disControl ofSexually Transmitted Diseases: A Handeas sand family planning: Strange or naturalbookfor the Design and Management ofPrograms.bedfellows, revisited. Sex Tl'a11SmDis'.'.' Arlington, VA: AIDSCAP/Family Health Inter,1993;20:174-78.SteinZ. Editorial: Family plan- ,.national, 1996; GrosskurthH, Mosha F, Todd],': 'et a1. Impact ofimproved treatment ofsexuallyning, sexuallytransmiheddiseases, and the pretransmitted diseases on Hrv infection in rural:velltionofAIDS - divided we fail? Am JPublicTanzania: Randominzed control trial. Lancet. REFERENCESHetllth 1996;86:783-84., i.'St Louis ME,Wasserheit]N, Gayle' . 1995;346:530-36; CommitteeoriPrevention and·.D··JAN·."d'ers.th'HIV.' demlC.'. H'ar- TRControlof.Sexually Transnlitted. Diseases,. EngH . . US. conSIepanB I .WT d 'T' h u'd'J E' J . C.d'.'.h.AIDS··.·.·.·.·,uter '1'1 ,e S. enlnessmg recent a. vances to en ancepre- . . :S'".' d lle11. ,pIll.emlc:h' on. . A J bf R. I h . . . ' CT.J'. ':." ont11lg .' exua. Iy Tl allS11t1tte DIseases. Was mgventlon. 'pm . u 1 11" eaFt ,mIPHrervss. oate . ,. ,:' ton: National Academy Press, 1996.Aggleton. , Q utzWl er ,et a.preventton. 5 Hberg RS R' . . h korn Windevelopirtgcountries'.Lancet 1996;348:1143-.K'I'P'"anen48. .' .' . '. " . unaso ,eta.l Impact 'foTJahnaiIPltd YHa0a an s IV-con-,. 3. The Status and Tl·ends 'ofthe Global HIV/trolprogramme as indicated by the decline of. AIDS Pa.lidemic.Svmnos.ium, Final Repolt.,sexuallytransmitted diseases. Lancet.I l'1994;334:243-45.(Arlington,VA:i\lDSCAP/F mily Health Inter 6 . Population Services International salesnational, Harvard School of Public Health and.'reports, unpublished. .UNAIDS, 199.6) 17."llfl'.I'p. '.Ne\V8 Brie Continuedfrom page 2In PPFA's U.S. clinics, nledical testing"seemed to be a barrier to IUD use in someinstances," says Kara Anderson, PPFA'snurse practitioner and consultant to themedical division. Clients who have a highrisk of seXually transmitted disease (STD)should still be tested routinely for commonSTDs, says Anderson, since IUD use in infected womenincreases the risk of pelvicinflammatory disease (PID).For all clients, PPFA providers continue to take careful medical and personalhistories, including looking for symptomsand asking questions that may lead tocontraindications. Providers are required tocheck for vaginal discharge, intermenstrualbleeding, vaginal inflammation and historyof seXual contact in order to determine if aclient is infected with an STD, Andersonsays.MIFEPRISTONE·TSAFETY, 'EFFICACYhe U.S. Food and DrugAdministra, tion (FDA) has determined that. clinical data demonstrate the safetyand effectiveness of an oral method of pregnancy termination, the use of the drugmifepristonein combination with·misoprostol under close medical supervision.Other issues, including manufacturingpractices and labeling,nlust be approved byFDA before the method is available in theUnited States. Mifepri tone for pregnancytermination is currently approved in France,the United Kingdom and Sweden.Also known as RU-486,mifepristoneconles in pill form and is taken' to' terminatepregnancy within the first seven weeks ofonset of a woman's last menstrual period.The regimen involves taking three tablets ofmifepristone (600 milligrams) followed two, days later by two tablets (400 micrograms)\pf oral·misoprostol.\"It can be offered by different kinds ofproviders and can be used earlier in a pregnancy (than surgical termination). It can beused as soon' as a pregnant woman missesher period," says Dr. Beverly Winikoff ofthe Population Council, a NewYork.;basedresearch organization seeking FDA approvalof mifepristone. 1The FDA's September ruling was'·based on clinical trials conducted in Franceshowing the approach was 95.5 percent effective in terminating pregnancy among2,480 women. Side effects, similar to·thoseof a natural miscarriage, included painfuluterine contractions, nausea, vomiting, diarrhea, pelvic pain and headaches, but medicalcomplications requiring hospital treatment·were few. Uterine bleeding requiring curettage or blood transfusion occurred inO. 3percent of the women.NOTE1. The U.S. Agency for InternationalDevelopment has not provided any financialassistance or other support in seeking theapproval.NETWORKWinter 19977
·Risk Assessments Seek.To Im,rove.Surelning.-,.:' '.-':,,',-;,.' - --. .While STD as essmel1tmodelsSh.gw mixed results,modifying for'local conditions imprbves usefulness.he only way to be certain someonehas a sexually transmitted disease·:(STD) is to identify the dis asecausing microbe .with laboratorytests, which are usually expensiveand often require a clientto return for results and treatment.Consequently, the World HealthOrganization (WHO) has developed an approach for diagnosing and treating STDswithout the use oflaboratory tests. CalledsYndromic management, this approach isbased only on a person's clinical signs andsymptoms. More recently, WHO and otherorganizations have begu developing a tool'called "risk assessment," which seeks to improve the accuracy ofSYfidromic screeningby including an evaluation of the client'sbehavior and other social circumstances thatare correlated with STD risks. Having multiple partners, for example, suggests agreater STD risk than beingin a monogamous relationship."STD risk assessments hold promise,but the,research is mixed on theirusefulnessat this point," says Dr. Willard CatesJr.,FHI senior vice presidentof biomedical affairs and an expert onSTDs. "What is clearis that any STD risk assessment has to bemodified to individualcountries and regionswithin countries, according to cultural issues, prevalence ofvarious STDs and otherfactors."Ide tifying infected clients by signs andsymptoms alone (sYndromic management)works well in some situations. For example,treating men with urethral discharge forgonorrhea and chlamydial infection is effective. However, id ntifying women withcervical infections, such as gonorrhea andchlamydial infection, has been less successfu1. 1 For many women infected with gonorrhea or chlamydia, there are no symptoms.While risk assessment models are beingstudied as ways to improve the accuracy ofdiagnosis for treatment, they can also playarolein STD prevention strategies. For example, risk assessments can be used effectively by nearly any family planningprogram for counseling on contraceptivechoices to improve STD prevention, saysLaurie Fox ofFHI, who studies STDservices and family planning programs.However, she.cautions, "Program managersshould not add STD risk assessment to theirroutine services without understanding itslimitations as a diagnostic tool."CHECKLIST OF QUESTIONSAn STD risk assessment is simply achecklist of questions on demographic, behavioral and related·factors. Questions coversuch issues as the number of sexual partnersa person has, the client's age, whether he orshe has had a new partner in recent months,has had·a previous STD infection, has symptoms such as a discharge or abdominal pain,
USA, who led the Haiti study.3whether his or her partner(To evaluate such models, rehas symptoms or othersearchers compare the results of asexual partners, andrisk assessment with laboratorywhether the partner travelstesting.)frequently.In 1993, WHO develA study among 964 womenoped a risk assessment toolattending a rural antenatal clinic inTanzania compared nine risk asto be used in conjunctionsessment models. As in Haiti, riskwith its sYlldromic manageassessments using localnlent approach (also knownsociodemographic factors imas syndromic algorithms)proved the performance of corfor vaginal discharge. 2 "Werectlydiagnosing women withsuggested that certain varigonorrhea and chlanlydial infecables would show an intions. One local risk assessmentcreased risk, such as beingcorrectlydiscovered 69 percent ofunder age 21, having asymptomatic partner orthe women who had the diseases,having a new partner in thebut incorrectly identified aboutseven uninfected wo en for treatlast three months," says Dr.Monir Islam, chief of thement for every one true infectionWHO's Family Planningit found.The local assessments askedand Population unit."But we should noteach woman (all were pregnant) ifhave been so specific, beshe was younger than 25, hermarital status, number of sexualcause the risks will be different in differentpartners over the last year,countries. Alot of countrieswhether she had any symptomtook this new list as definirelated to genital infection, hadpreviously given birth (indicatingtive," he says. For example,in some settings, womenthat sexual activity had not begunrecently) and, if so, whether hermay not know if their husbands have symptoms'.most recent birth had been moreBERYL GOLDBERGthan five years ago (indicating posCouples may always havesex in the dark, which maysible low fertility due to STD inSOME RISK ASSESSMENT MODELS INCORRECTLY IDENTIFY WOMEN ASfection). Answers had weightedmean that a woman wouldHAVING AN STD WHEN THEY DO NOT, LEADING TO UNNECESSARYnot observe her husband'sscores, with a certain total score orTREATMENT AND FAMILY DISCORD WHEN THEY INFORM HUSBANDS.genital ulcers or urethralhigher indicating treatment for gonorrhea and chlamydia. discharge.Among women withA study in Zaire among urbanA study among 996 women attendingpregnant women used the results of a leukovaginal discharge, STD risk assessmentsan antenatal clinic in Haiti found that a riskbased on local factors seem to improve thecyte esterase dipstick (LED) test on urine inassessnlent model based on local risk factorsidentification of those who have gonorrheaaddition to other factors, including age,correctly identified almost nine of every 10or chlamydial infection. Unfortunately,marital status, number of sexual partners andinfected women. However, the model alsothey also incorrectly identify many womensymptoms. The LED, a simple test that doesconcluded incorrectly that many uninfectedas having an STD when they do not, thusnot require laboratory facilities, predictswomen were also in need of treatment. Forleading to unnecessary treatments.possible infection using a color chart toevery five women designated by the modelTreating uninfected people who areshow an elevated white blood cell count.for treatment, only one was actually infected.led to believe they have an STD can beThis approach identified nearly three of evAmong symptonlatic women, risk asemotionally traumatic, especially when theyery four infected women. 5sessment can increase the sensitivity of cliniinform their partners. Hence, an uninfectedcal diagnosis among infected women,PARTNER'S BEHAVIORwife asking her uninfected husband to beconcludes Frieda Behets of the University oftreated can imply that he or she has beenIn a review of STD risk assessmentNorth Carolina (UNC) Medical School,unfaithful. Excessive treatment with antibistudies conducted in Africa, Susan Chen andotics can also result in STD organisms thather colleagues at FHI concluded that amongare resistant to the antibiotic.married, monogamous women, thehusband's behavior may be a better indicatorNETWORKWinter 19979
of the woman's riskthan is the woman'sbehavior. Ahusbandmay bring an infectionto his wife from extramarital sex. For thehusband's behavior tobe useful in the riskassessment, a womanmust be able to reporth r partner's behavioraccurately.6Research in Kenyaamong pregnantwomen at an urbanclinic found risk assessment generally performed poorly indetecting gonorrheaand chlamydial cervicitis. 7 "The women wereat risk primarily because of their partners'behavior, and it wasvery difficult to getaccurate information. about the partners,"explains Dr. StephenIMPACT VISUALS/ BRUCE PATONMoses of the FACTORS,INCLUDINGRECENTSEXUALtive research programof the University ofPARTNERS AND OTHER SOCIAL OR BEHAVIOR CIRCUMSTANCES THAT ARE CORRELATED WITH STD RISKS.Nairobi MedicalSchool and the University ofManitoba,i' CONTRACEPTIVE CHOICEBrasil (BEMFAM), the InternationalCanada, which conducted the study.Planned Parenthood Federation (IPPF) afWith the sharp increase ofHIV andArecent study at aJamaican familyfiliate in Brazil, then trained its staff in STDother STDs in developing countries, evaluplanning clinic also found that a risk assessprevention.ating the risk of STD infection among famment approach did not detect STDs accu"All women who come to the clinic arerately. The most predictive measure of STD ily planning clients i
DR. WILLARD CATES FHI PREVENTION WORKS Clearly, universal access to effective, afford able antiviral therapy is a distant goal. But the good news-newsthat has made few headlines - is that we can reduce the need for treatment. Data show that HNpreven tion works - and at a fraction ofthe cost of drug treatment.2 As in basic and clini cal .