Transcription
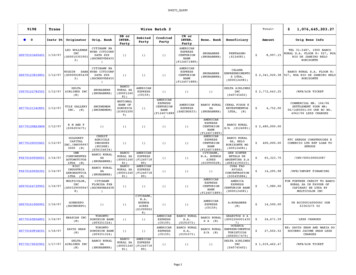
2010 Summary of BenefitsHumana Prescription Drug PlanHumana Standard S5884-076 (PDP)Humana Enhanced S5884-016 (PDP)Humana Complete S5884-046 (PDP)Missouri1S5884 SB PDP 10 FINAL 18 KC0809S5884NAV18SB10 0925
5Section I – Introduction to the Summary of BenefitsJanuary 1, 2010 - December 31, 2010Thank you for your interest in Humana Prescription Drug Plan. Our plan is offered by Humana Insurance Company, aMedicare Prescription Drug Plan that contracts with the Federal government. This Summary of Benefits tells you somefeatures of our plan. It doesn't list every drug we cover, every limitation, or exclusion. To get a complete list of ourbenefits, please call Humana Prescription Drug Plan and ask for the "Evidence of Coverage".You Have Choices in Your Medicare Prescription Drug CoverageAs a Medicare beneficiary, you can choose from different Medicare prescription drug coverage options. One option is toget prescription drug coverage through a Medicare Prescription Drug Plan, like Humana Prescription Drug Plan. Anotheroption is to get your prescription drug coverage through a Medicare Advantage Plan that offers prescription drugcoverage. You make the choice.How Can I Compare My Options?The charts in this booklet list some important drug benefits. You can use this Summary of Benefits to compare thebenefits offered by Humana Prescription Drug Plan to the benefits offered by other Medicare Prescription Drug Plans orMedicare Advantage Plans with prescription drug coverage.Where Is Humana Prescription Drug Plan Available?The service area for this plan includes: Missouri. You must live in this area to join the plan.There is more than one plan listed in this Summary of Benefits. If you are enrolled in one plan and wish to switch toanother plan, you may do so during certain times of the year. Please call Customer Service for more information.Who Is Eligible To Join?You can join this plan if you are entitled to Medicare Part A and/or enrolled in Medicare Part B and live in the service area.If you are enrolled in an MA coordinated care (HMO or PPO) plan or an MA PFFS plan that includes Medicare prescriptiondrugs, you may not enroll in a PDP unless you disenroll from the HMO, PPO or MA PFFS plan.Enrollees in a private fee-for-service plan (PFFS) that does not provide Medicare prescription drug coverage or an MAMedical Savings Account (MSA) plan may enroll in a PDP. Enrollees in an 1876 Cost plan may enroll in a PDP.You cannot enroll in this plan if your current or former employer or union (or your spouse’s current or former employer orunion) helps pay for your drugs.Does My Plan Cover Medicare Part B or Part D Drugs?Humana Prescription Drug Plan does not cover drugs that are covered under Medicare Part B as prescribed and dispensed.Generally, we only cover drugs, vaccines, biological products and medical supplies that are covered under the MedicarePrescription Drug Benefit (Part D) and that are on our formulary.2 – SUMMARY OF BENEFITS
9Section I (continued)Where Can I Get My Prescriptions?Humana Prescription Drug Plan has formed a network of pharmacies. You must use a network pharmacy to receive planbenefits. We will not pay for your prescriptions if you use an out-of-network pharmacy, except in certain cases.Humana Prescription Drug Plan has a list of preferred pharmacies. At these pharmacies, you may get your drugs at a lowercopayment or coinsurance. A non-preferred pharmacy is still a network pharmacy, but you may have to pay more for yourprescription drugs.The pharmacies in our network can change at any time. You can ask for a Pharmacy Directory or visit us atwww.humana.com/members/tools/prescription tools/medicare drug list.asp. Our customer service number is listed at theend of this introduction.What Is A Prescription Drug Formulary?Humana Prescription Drug Plan uses a formulary. A formulary is a list of drugs covered by your plan to meet patientneeds. We may periodically add, remove, or make changes to coverage limitations on certain drugs or change how muchyou pay for a drug. If we make any formulary change that limits our members’ ability to fill their prescriptions, we willnotify the affected enrollees before the change is made. We will send a formulary to you and you can see our completeformulary on our Web site at www.humana.com/members/tools/prescription tools/medicare drug list.asp.If you are currently taking a drug that is not on our formulary or subject to additional requirements or limits, you may beable to get a temporary supply of the drug. You can contact us to request an exception or switch to an alternative druglisted on our formulary with your physician’s help. Call us to see if you can get a temporary supply of the drug or for moredetails about our drug transition policy.What Should I Do If I Have Other Insurance In Addition To Medicare?If you have a Medigap (Medicare Supplement Insurance) policy that includes prescription drug coverage, you must contactyour Medigap Issuer to let them know that you have joined a Medicare Prescription Drug Plan. If you decide to keep yourcurrent Medigap policy, your Medigap Issuer will remove the prescription drug coverage portion from your Medigap policy.This will occur as of the effective date of your Medicare Prescription Drug Plan coverage. Your Issuer will adjust yourpremium. Call your Medigap Issuer for details.If you or your spouse has, or is able to get, employer group coverage, you should talk to your employer to find out howyour benefits will be affected if you join Humana Prescription Drug Plan. Get this information before you decide to enroll inthis plan.How Can I Get Extra Help With My Prescription Drug Plan Costs?If you qualify for extra help with your Medicare prescription drug plan costs, your premium and costs at the pharmacy willbe lower. When you join Humana Prescription Drug Plan, Medicare will tell us how much extra help you are getting. Thenwe will let you know the amount you will pay. If you are not getting this extra help you can see if you qualify by calling1-800-MEDICARE (1-800-633-4227). TTY/TDD users should call 1-877-486-2048.SUMMARY OF BENEFITS – 3
9Section I (continued)What Are My Protections In This Plan?All Medicare Prescription Drug Plans agree to stay in the program for a full year at a time. Each year, the plans decidewhether to continue for another year. Even if a Medicare Prescription Drug Plan leaves the program, you will not loseMedicare coverage. If a plan decides not to continue, it must send you a letter at least 60 days before your coverage willend. The letter will explain your options for Medicare prescription drug coverage in your area.As a member of Humana Prescription Drug Plan, you have the right to request a coverage determination, which includesthe right to request an exception, the right to file an appeal if we deny coverage for a prescription drug, and the right tofile a grievance. You have the right to request a coverage determination if you want us to cover a Part D drug that youbelieve should be covered. An exception is a type of coverage determination. You may ask us for an exception if youbelieve you need a drug that is not on our list of covered drugs or believe you should get a non-preferred drug at a lowerout-of-pocket cost. You can also ask for an exception to cost utilization rules, such as a limit on the quantity of a drug. Ifyou think you need an exception, you should contact us before you try to fill your prescription at a pharmacy. Your doctormust provide a statement to support your exception request. If we deny coverage for your prescription drug(s), you havethe right to appeal and ask us to review our decision. Finally, you have the right to file a grievance if you have any type ofproblem with us or one of our network pharmacies that does not involve coverage for a prescription drug. If your probleminvolves quality of care, you also have the right to file a grievance with the Quality Improvement Organization (QIO) foryour state, Primaris 1-800-347-1016 (toll free).What Is A Medication Therapy Management (MTM) Program?A Medication Therapy Management (MTM) Program is a free service we may offer. You may be invited to participate in aprogram designed for your specific health and pharmacy needs. You may decide not to participate but it is recommendedthat you take full advantage of this covered service if you are selected. Contact Humana Prescription Drug Plan for moredetails.Plan RatingsThe Medicare program rates how well plans perform in different categories (for example, detecting and preventing illness,ratings from patients and customer service). If you have access to the web, you may use the web tools onwww.medicare.gov and select “Compare Medicare Prescription Drug Plans” or “Compare Health Plans and MedigapPolicies in Your Area” to compare the plan ratings for Medicare plans in your area. You can also call us directly at (800)281-6918 to obtain a copy of the plan ratings for this plan. TTY users call (800) 833-3301.4 – SUMMARY OF BENEFITS
5Please call Humana Insurance Company for more information about the Humana Prescription Drug Plan.Visit us at www.humana-medicare.com or, call us:Customer Service Hours: Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, 8 a.m. - 8 p.m.Current members should call toll-free (800) 281-6918.(TTY/TDD (800) 833-3301)Prospective members should call toll-free (800) 706-0872.(TTY/TDD (877) 833-4486)For more information about Medicare, please call Medicare at 1-800-MEDICARE (1-800-633-4227). TTY users should call1-877-486-2048. You can call 24 hours a day, 7 days a week. Or, visit www.medicare.gov on the web.If you have special needs, this document may be available in other formats.SUMMARY OF BENEFITS – 5
4If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREPrescription Most drugs areDrugsnot coveredunder OriginalMedicare. Youcan addprescriptiondrug coverageto OriginalMedicare byjoining aMedicarePrescriptionDrug Plan, oryou can get allyour Medicarecoverage,includingprescriptiondrug coverage,by joining aMedicareAdvantage Planor a MedicareCost Plan thatoffersprescriptiondrug coverage.HUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Drugs covered under Medicare Part D (General) This plan uses a formulary. The plan will send you the formulary. You can also see theformulary athttp://www.humana.com/members/tools/prescription tools/medicare drug list.asp on theweb. Different out-of-pocket costs may apply for people who– have limited incomes,– live in long term care facilities, or– have access to Indian/Tribal/Urban (Indian Health Service). 48.30 monthly premium. 42.00 monthly premium. 104.00 monthly premium. The plan offers national in-network prescription coverage (i.e., this would include 50states, Puerto Rico and D.C.). This means that you will pay the same cost-sharing amountfor your prescription drugs if you get them at an in-network pharmacy outside of the plan’sservice area (for instance when you travel). Total yearly drug costs are the total drug costs paid by both you and the plan. The plan may require you to first try one drug to treat your condition before it will coveranother drug for that condition. Some drugs have quantity limits. Your provider must get prior authorization from Humana Prescription Drug Plan for certaindrugs. You must go to certain pharmacies for a very limited number of drugs, due to the specialhandling, provider coordination, or patient education requirements for these drugs thatcannot be met by most pharmacies in your network. These drugs are listed on the plan’swebsite, formulary, and printed materials, as well as on the Medicare Prescription DrugPlan Finder on Medicare.gov. If the actual cost of a drugis less than the normalcost-sharing amount forthat drug, you will pay theactual cost, not the highercost-sharing amount. If the actual cost of a drugis less than the normalcost-sharing amount forthat drug, you will pay theactual cost, not the highercost-sharing amount. If the actual cost of a drugis less than the normalcost-sharing amount forthat drug, you will pay theactual cost, not the highercost-sharing amount.(Continued Next page)6 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) If you request a formularyexception for a drug andHumana Prescription DrugPlan approves theexception, you will payNon-Preferred Brandcost-sharing for that drug. If you request a formularyexception for a drug andHumana Prescription DrugPlan approves theexception, you will payNon-Preferred Brandcost-sharing for that drug. If you request a formularyexception for a drug andHumana Prescription DrugPlan approves theexception, you will payNon-Preferred Brandcost-sharing for that drug.IN-NETWORK 310 yearly deductibleIN-NETWORK 0 deductibleIN-NETWORK 0 deductibleInitial Coverage After you pay your yearlydeductible, you pay thefollowing until total yearlydrug costs reach 2,830.Initial CoverageInitial Coverage You pay the following until You pay the following untiltotal yearly drug costs reach total yearly drug costs reach 2,770. 2,790.(Continued Next page)SUMMARY OF BENEFITS – 7
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Retail PharmacyRetail PharmacyRetail Pharmacy Preferred Generic Preferred Generic Preferred Generic– 15% coinsurance for a– 7 copayment for a– 7 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferredfrom a preferredfrom a preferredpharmacypharmacypharmacy– 15% coinsurance for a– 21 copayment for a– 21 copayment for athree-month (90-day)three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferredfrom a preferred pharmacyfrom a preferredpharmacypharmacy– 12 copayment for a– 20% coinsurance for aone-month (30-day)– 12 copayment for aone-month (30-day)supply of drugs in this tierone-month (30-day)supply of drugs in this tierfrom a non-preferredsupply of drugs in this tierfrom a non-preferredpharmacyfrom a non-preferredpharmacypharmacy– 36 copayment for a– 20% coinsurance for athree-month (90-day)– 36 copayment for athree-month (90-day)supply of drugs in this tierthree-month (90-day)supply of drugs in this tierfrom a non-preferredsupply of drugs in this tierfrom a non-preferredpharmacyfrom a non-preferredpharmacypharmacy(Continued Next page)8 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Non-Preferred Non-Preferred Non-PreferredGenerics/Preferred BrandGeneric/Preferred BrandGenerics/Preferred Brand– 25% coinsurance for a– 45 copayment for a– 45 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred pharmacyfrom a preferred pharmacyfrom a preferredpharmacy– 25% coinsurance for a– 135 copayment for athree-month (90-day)three-month (90-day)– 135 copayment for asupply of drugs in this tiersupply of drugs in this tierthree-month (90-day)from a preferred pharmacyfrom a preferred pharmacysupply of drugs in this tierfrom a preferred– 30% coinsurance for a– 50 copayment for apharmacyone-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tier– 50 copayment for afrom a non-preferredfrom a non-preferredone-month (30-day)pharmacypharmacysupply of drugs in this tierfrom a non-preferred– 30% coinsurance for a– 150 copayment for apharmacythree-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tier– 150 copayment for afrom a non-preferredfrom a non-preferredthree-month (90-day)pharmacypharmacysupply of drugs in this tierfrom a non-preferredpharmacy(Continued Next page)SUMMARY OF BENEFITS – 9
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Non-Preferred Brand Non-Preferred Brand Non-Preferred Brand– 44% coinsurance for a– 75 copayment for a– 75 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred pharmacyfrom a preferred pharmacyfrom a preferredpharmacy– 44% coinsurance for a– 225 copayment for athree-month (90-day)three-month (90-day)– 225 copayment for asupply of drugs in this tiersupply of drugs in this tierthree-month (90-day)from a preferred pharmacyfrom a preferred pharmacysupply of drugs in this tierfrom a preferred– 49% coinsurance for a– 80 copayment for apharmacyone-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tier– 80 copayment for afrom a non-preferredfrom a non-preferredone-month (30-day)pharmacypharmacysupply of drugs in this tierfrom a non-preferred– 49% coinsurance for a– 240 copayment for apharmacythree-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tier– 240 copayment for afrom a non-preferredfrom a non-preferredthree-month (90-day)pharmacypharmacysupply of drugs in this tierfrom a non-preferred– Not all drugs on this tier– Not all drugs on this tierpharmacyare available at thisare available at thisextended day supply.extended day supply.– Not all drugs on this tierPlease contact the plan forPlease contact the planare available at thismore information.for more information.extended day supply.Please contact the plan formore information.(Continued Next page)10 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Specialty Specialty– 33% coinsurance for a– 33% coinsurance for aone-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tierfrom a preferredfrom a preferred pharmacypharmacy– 33% coinsurance for a– 33% coinsurance for aone-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tierfrom a non-preferredfrom a non-preferredpharmacypharmacyLong Term CareLong Term CareLong Term CarePharmacyPharmacyPharmacy Preferred Generic Preferred Generic Preferred Generic– 15% coinsurance for a– 7 copayment for a– 7 copayment for aone-month (34-day)one-month (34- day)one-month (34- day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tier Non-Preferred Non-Preferred Non-PreferredGenerics/Preferred BrandGeneric/Preferred BrandGenerics/Preferred Brand– 25% coinsurance for a– 45 copayment for a– 45 copayment for aone-month (34-day)one-month (34-day)one-month (34-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tier Non-Preferred Brand Non-Preferred Brand Non-Preferred Brand– 44% coinsurance for a– 75 copayment for a– 75 copayment for aone-month (34-day)one-month (34-day)one-month (34-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tier Specialty Specialty– 33% coinsurance for a– 33% coinsurance for aone-month (34-day)one-month (34-day)supply of drugs in this tiersupply of drugs in this tier(Continued Next page)SUMMARY OF BENEFITS – 11
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Mail OrderMail OrderMail Order Preferred Generic Preferred Generic Preferred Generic– 0% coinsurance for a– 0 copayment for a– 0 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mailorder pharmacyorder pharmacyorder pharmacy– 0% coinsurance for a– 0 copayment for a– 0 copayment for athree-month (90-day)three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mailorder pharmacyorder pharmacyorder pharmacy– 15% coinsurance for a– 7 copayment for a– 7 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy– 15% coinsurance for a– 21 copayment for a– 21 copayment for athree-month (90-day)three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy(Continued Next page)12 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Non-Preferred Non-Preferred Non-PreferredGenerics/Preferred BrandGeneric/Preferred BrandGenerics/Preferred Brand– 25% coinsurance for a– 45 copayment for a– 45 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mailorder pharmacyorder pharmacyorder pharmacy– 25% coinsurance for a– 112.50 copayment for a – 112.50 copayment for athree-month (90-day)three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mailorder pharmacyorder pharmacyorder pharmacy– 25% coinsurance for a– 45 copayment for a– 45 copayment for aone-month (30-day)one-month (30-day)one-month (30- day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy– 25% coinsurance for a– 135 copayment for a– 135 copayment for athree-month (90-day)three-month (90-day)three-month (90- day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy(Continued Next page)SUMMARY OF BENEFITS – 13
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Non-Preferred Brand Non-Preferred Brand Non-Preferred Brand– 44% coinsurance for a– 75 copayment for a– 75 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mailorder pharmacyorder pharmacyorder pharmacy– 44% coinsurance for a– 187.50 copayment for– 187.50 copayment for athree-month (90-day)a three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mailfrom a preferred mail orderorder pharmacyorder pharmacypharmacy– 44% coinsurance for a– 75 copayment for a– 75 copayment for aone-month (30-day)one-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy– 44% coinsurance for a– 225 copayment for a– 225 copayment for athree-month (90-day)three-month (90-day)three-month (90-day)supply of drugs in this tiersupply of drugs in this tiersupply of drugs in this tierfrom a non-preferred mailfrom a non-preferred mailfrom a non-preferred mailorder pharmacyorder pharmacyorder pharmacy– Not all drugs on this tier– Not all drugs on this tier– Not all drugs on this tierare available at thisare available at thisare available at thisextended day supply.extended day supply.extended day supply.Please contact the planPlease contact the planPlease contact the planfor more information.for more information.for more information.(Continued Next page)14 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP) Specialty Specialty– 33% coinsurance for a– 33% coinsurance for aone-month (30-day)one-month (30-day)supply of drugs in this tiersupply of drugs in this tierfrom a preferred mailfrom a preferred mail orderorder pharmacypharmacy– 33% coinsurance for a– 33% coinsurance for aone-month (30-day)one-month (30-day) supplysupply of drugs in this tierof drugs in this tier from afrom a non-preferred mailnon-preferred mail orderorder pharmacypharmacy Coverage Gap Coverage Gap Coverage Gap– After your total yearly– After your total yearly– The plan covers manygenerics (65%-99% ofdrug costs reach 2,830,drug costs reach 2,770,formulary generic drugs)you pay 100% until youryou pay 100% until yourthrough the coverageyearly out-of-pocket drugyearly out-of-pocket druggap.costs reach 4,550.costs reach 4,550.– You pay the following:(Continued Next page)SUMMARY OF BENEFITS – 15
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Retail Pharmacy Preferred Generic– 7 copayment for aone-month (30-day)supply of all drugscovered in this tier from apreferred pharmacy– 21 copayment for athree-month (90-day)supply of all drugs coveredin this tier from apreferred pharmacy– 12 copayment for aone-month (30-day)supply of all drugs coveredin this tier from anon-preferred pharmacy– 36 copayment for athree-month (90-day)supply of all drugs coveredin this tier from anon-preferred pharmacyLong Term CarePharmacy Preferred Generic– 7 copayment for aone-month (34-day)supply of all drugs coveredin this tier(Continued Next page)16 – SUMMARY OF BENEFITS
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Mail Order Preferred Generic– 0 copayment for aone-month (30-day)supply of all drugs coveredin this tier from apreferred mail orderpharmacy– 0 copayment for athree-month (90-day)supply of all drugs coveredin this tier from a preferredmail order pharmacy– 7 copayment for aone-month (30-day)supply of all drugs coveredin this tier from anon-preferred mail orderpharmacy– 21 copayment for athree-month (90-day)supply of all drugs coveredin this tier from anon-preferred mail orderpharmacy– For all other covereddrugs, after your totalyearly drug costs reach 2,790, you pay 100%until your yearlyout-of-pocket drug costsreach 4,550.(Continued Next page)SUMMARY OF BENEFITS – 17
26If you have any questions about this plan's benefits or costs, please contact Humana Insurance Company for details.Section II - Summary of BenefitsHUMANA PRESCRIPTION DRUG PLANBENEFITORIGINALMEDICAREHUMANA STANDARDS5884-076 (PDP)HUMANA ENHANCEDS5884-016 (PDP)HUMANA COMPLETES5884-046 (PDP)Catastrophic Coverage After your yearlyout-of-pocket drug costsreach 4,550, you pay thegreater of:– A 2.50 copayment forgeneric (including branddrugs treated as generic)and a 6.30 copaymentfor all other drugs, or– 5% coinsurance.Catastrophic Coverage After your yearlyout-of-pocket drug costsreach 4,550, you pay thegreater of:– A 2.50 copayment forgeneric (including branddrugs treated as generic)and a 6.30 copaymentfor all other drugs, or– 5% coinsurance.Catastrophic Coverage After your yearlyout-of-pocket drug costsreach 4,550, you pay thegreater of:– A 2.50 copayment forgeneric (including branddrugs treated as generic)and a 6.30 copaymentfor all other drugs, or– 5% coinsurance.OUT-OF-NETWORKOUT-
It doesn't list every drug we cover, every limitation, or exclusion. To get a complete list of our benefits, please call Humana Prescription Drug Plan and ask for the "Evidence of Coverage". You Have Choices in YourMedicare Prescription Drug Coverage As a Medicare beneficiary, you can choose from different Medicare prescription drug coverage .