Transcription
PolypharmacyManagementby 2030:a patient safetychallenge
PolypharmacyManagementby 2030:a patient safetychallenge2nd edition
Stimulating Innovation Management ofPolypharmacy and Adherence in The Elderly
PolypharmacyManagementby 2030:a patient safetychallenge2nd editionAlpana MairFernando Fernandez-LlimosAlbert AlonsoCathy HarrisonSimon HurdingThomas KempenMoira KinnearNils MichaelJennifer McIntoshMartin WilsonThe SIMPATHY consortium
Mair A, Fernandez-Llimos F, Alonso A, Harrison C, Hurding S, Kempen T,Kinnear M, Michael N, McIntosh J, Wilson M, The Simpathy consortium.Polypharmacy Management by 2030: a patient safety challenge,2nd edition. Coimbra: SIMPATHY Consortium; 2017.The SIMPATHY consortium was constituted by: Alpana Mair, VictoriaElliott, Simon B Hurding, Steve Kendrick, Moira Kinnear, Katie MacLure,Derek Mckenzie, Nils Michael, Derek Stewart, Neil Stewart, Martin Wilson[Scotland]; Astrid Forsström, Thomas Kempen, Ulrika Gillespie [Sweden];Albert Alonso, Carles Codina, Jennifer McIntosh [Catalonia]; GlendaFleming, Cathy Harrison, Michael Scott, Claire Scullin [Northern Ireland];Birgitt Wiese, Ulrike Junius Walker [Germany]; João O. Malva, MargaridaCastel-Branco, Fernando Fernandez-Llimos, Isabel V. Figueiredo, CarlosFontes Ribeiro, Manuel T. Veríssimo [Portugal]; Michele Arcopinto, AntonioCittadini, Maddalena Illario, Vincenzo de Luca, Enrica Menditto, SalvatoreRiegler, Guiseppe Simeone, [Italy]; Przemysław Kardas, Paweł Lewek[Poland]; Anastasia Balasopoulou, Mary Geitona, Dimitra Gennimata,Christos Kampolis, Theodore Vontetsianos [Greece].The SIMPATHY consortium would like to acknowledge the contribution ofMarty Linsky to the content of this document.1. Polypharmacy. 2. Patient Safety. 3. Deprescriptions. 4. InappropriatePrescribing. 5. Health Policy. 6. Health Plan Implementation. 7. Health CareEconomics and Organizations. 8. Leadership. 9. Interprofessional Relations.(NLM classification: WX 185) 2017 by The SIMPATHY Consortium.Published by the SIMPATHY consortium.Legal deposit: 429217/17ISBN: 978-989-20-7674-4Available at: www.simpathy.euThis document is distributed under a Creative Commons AttributionNonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0).Graphic: Simon HurdingDesign: FBA.Printed by: Organigráfica Artes Gráficas, Lda.This document is part of SIMPATHY project (663082),Co-funded bywhich has received funding from the European Union’sthe Health ProgrammeHealthProgrammeofthe EuropeanUnion (2014-2020)Disclaimer:The material contained in this document is provided for informationpurposes only. No warranty is given in relation to use that maybe made of it and neither the copyright owners or the EuropeanCommission accept any liability for loss or damage to a third partyarising from such use.The content of this document represents the views of the authorsonly and is his/her sole responsibility; it cannot be considered toreflect the views of the authors or editors’ Institutions, or EuropeanCommission and/or the Consumers, Health, Agriculture andFood Executive Agency, or any other body of the European Union.The European Commission and the Agency do not accept anyresponsibility for use that may be made of the information it contains.
Contents9111314Foreword17Chapter 1: The case for appropriatepolypharmacy management19192022Executive summaryIntroductionAbout this handbookComplex careQualityEconomicPolitics and policy27Chapter 2: Preparing for changein polypharmacy management2929323232Preparing for change in polypharmacySystems approach in health and careStrategies for change managementAccounting for culturePatient centered35Chapter 3: Approaches to implementpolypharmacy management at scale373838404040424245454848515151Change management frameworkGetting ready for change#1 Choosing a model#2 Sharing leadership#3 Assessing the scenario#4 BenchmarkingImplementing change#5 Setting the vision#6 Creating guidelines#7 Training the workforceSpreading change#8 Using dataSustaining change#9 Changing regulations#10 Evaluating the programme53Chapter 4: EU collaboration forglobal patient safety challenge54565656Summary of recommendations59ReferencesShort termMedium termLong term
AbbreviationsADR – Adverse drug reactionAGREE II-GRS – Appraisal of guidelines for researchand valuation II - global rating scaleEU – European UnionICT – Information and communications technologyNPT – Normalization process theoryPESTEL – Political, economic, social, technological,environmental, and legalSIMPATHY – Stimulating Innovation Management ofPolypharmacy and Adherence in The ElderlySWOT – Strengths, weaknesses, opportunities and threatsWHO – World Health Organization
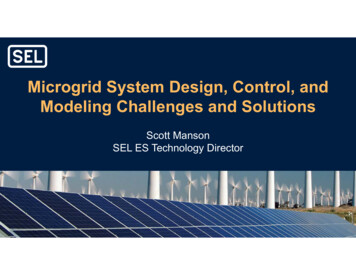
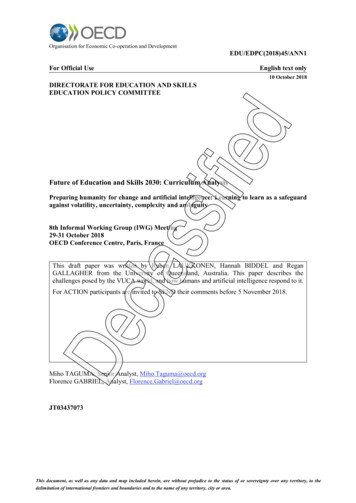
SIMPATHYForewordPopulations are aging, and many people over the age of 50 live with multiplelong-term conditions and take multiple medications. Medication is the singlemost common healthcare intervention and generates the third highest costof health expenditure. Up to 11% of all unplanned hospital admissions areattributable to medicines related harm.a The European Union has identifiedthe reduction of avoidable harm in healthcare as a key priority. Over the last 15years, in reports such as To Err is Human, countries have raised patient safetyas an opportunity to reduce harm. Building on this, both Choosing Wisely,Free from Harm and the Patient Safety 2030 report suggest that this couldbe approached by developing a holistic systematic approach that extendsacross the professional, cultural, technological and procedural boundaries.b,c,dThe SIMPATHY (Stimulating Innovation Management of Polypharmacyand Adherence in The Elderly) consortium have explored how healthcaremanagement programmes can be implemented to improve medication safetyand prevent patient harm by addressing the appropriate use of multiplemedications (polypharmacy). Fundamental to these programmes is theprinciple that providers work in partnership with patients to enable shareddecision making regarding medication, which improves patient adherenceand medicines related outcomes.This report sets out the case for prioritising working together now to addressinappropriate medication use over the next decade, to ensure the quality,economic and political systems are put in place to improve medication safetyfor patients. There are encouraging signs of the increasing recognition of thesechallenges, and the timeliness of this report. In March 2017, the World HealthOrganization (WHO) launched a global patient challenge to address medicationsafety, with polypharmacy as a flagship element. A special interest group waslaunched by the International Foundation on Integrated Care in May 2017.First and foremost, the priority for polypharmacy management has to beabout the quality and safety of patient care. It is essentially done within theeconomic resources available and enabled by political support.We commend the recommendations of this report to you and call for yoursupport in tackling together the important issues in delivering appropriatemanagement of polypharmacy.Liam J DonaldsonEdward T KelleyEnvoy for Patient SafetyWorld Health OrganizationGeneva, SwitzerlandDirector, Service Delivery and SafetyWorld Health OrganizationGeneva, Switzerlanda. Kongkaew C, Hann M, Mandal J, Williams SD, Metcalfe D, Noyce PR, Ashcroft DM. Risk factors for hospitaladmissions associated with adverse drug events. Pharmacotherapy. 2013;33(8):827-37. doi:10.1002/phar.1287b. Kohn LT, Corrigan JM, Donaldson MS, Eds. To err is human - building a safer health system. Washington, D.C.National Academy Press; 2000. ISBN: 0-309-06837-1c. Malhotra A, Maughan D, Ansell J, Lehman R, Henderson A, Gray M, Stephenson T, Bailey S. Choosing Wiselyin the UK: the Academy of Medical Royal Colleges’ initiative to reduce the harmsof too much medicine. BMJ. 2015;350:h2308. doi: 10.1136/bmj.h2308.d. Yu A, Flott K, Chainani N, Fontana G, Darzi A. Patient Safety 2030. London: NIHR Imperial Patient SafetyTranslational Research Centre; 2016.9
UNPLANNED HOSPITALADMISSIONS CAUSED BYADVERSE DRUG EVENTS8.6MILLIONADMISSIONSIN EUROPEEVERY YEAR50% OF HOSPITAL ADMISSIONSDUE TO ADVERSE DRUGEVENTS ARE PREVENTABLE70%OFTHESE AREIN PATIENTSOVER65YEARSOF AGEANDON5OR MOREMEDICINES
SIMPATHYExecutive SummaryAll of us have a role to play in leadership to drive changeto manage polypharmacy, regardless of the position wehold and whether we are patient organisations, government bodies, clinicians, managers or policymakers.Inappropriate polypharmacy and medicines adherencein the elderly is one of the most significant public healthchallenges of the current age. This burden is set toincrease as the population ages and more people sufferfrom multiple long-term conditions. There remains a lackof evidence-based solutions, as both medical researchand healthcare delivery models have focused on singledisease interventions. This challenge, and the limitedrange of solutions, have significant implications for howhealthcare resource is used to address inappropriatepolypharmacy. However, with up to 11% of unplannedhospital admissions being attributable to harm from medicines, and over 70% of these being due to elderly patientson multiple medicines there are significant opportunitiesto reduce this burden by timely and effective interventions.1The Institute of Medicine report, Responsible use of Medicines demonstrates that 0.3% of the global health budgetcould be saved by managing polypharmacy appropriately.2The report identifies key areas of focus which include usingrisk stratification to identify vulnerable patients and a morecollaborative role for pharmacists, physicians and patients.Facing the challenge of reducing patient harm, the European Union (EU) issued a public health call to identify, develop and implement innovative solutions that can be implemented at scale to address key problems. StimulatingInnovation Management of Polypharmacy and Adherencein the Elderly (SIMPATHY) is one of the funded projects todeliver tools to implement polypharmacy managementprogrammes throughout the EU in the context of quality,economic and political factors.The SIMPATHY case studies, benchmarking surveyand literature review demonstrate that there are someeffective polypharmacy management programmes inthe EU, but that they are too few in number. The projectalso demonstrates that patients believe inappropriatepolypharmacy is an important issue to address.This report calls for EU countries to work together in afocused way to manage and prevent inappropriatepolypharmacy, and improve medicines adherence,through the use of a change management approachthat is coordinated and collaborative in order to deliverbetter patient outcomes through the following six keyrecommendations:1. Use a systems approach that has multidisciplinaryclinical and policy leadership2. Nurture a culture that encourages and prioritisesthe safety and quality of prescribing3. Ensure that patients are integral to the decisionsmade about their medicines and are empoweredand supported to do so4. Use data to drive change5. Adopt an evidenced based approach with a biastowards action6. Utilise, develop and share tools to supportimplementationAdopting these recommendations will help prepare EUcountries for the WHO global patient safety challengeto improve medication safety, of which polypharmacyis an essential element.11
MORE PEOPLE HAVE MULTIMORBIDITYTHAN A SINGLE DISEASE65-84 YRS45-64 YRS30 %65% 85 YRS82 %PERCENTAGE OF PATIENTS PRESCRIBED TEN OR MORE MEDICINESBY AGE GROUP AND DEPRIVATION40%35%Percent of population30%25%20%15%10%5%0%50-541 (Most deprived)55-59260-643465-6970-74Patient age band5 (Lest deprived)75-7980-8485
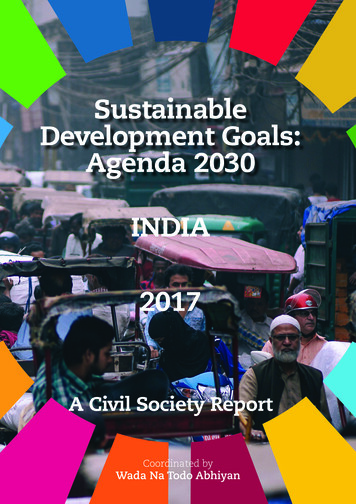
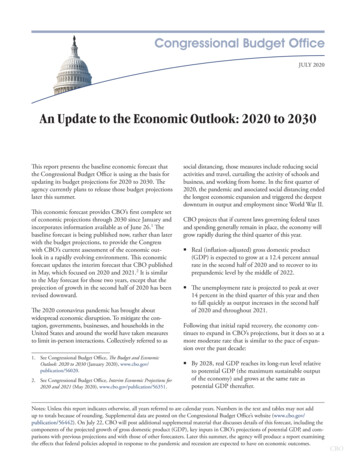
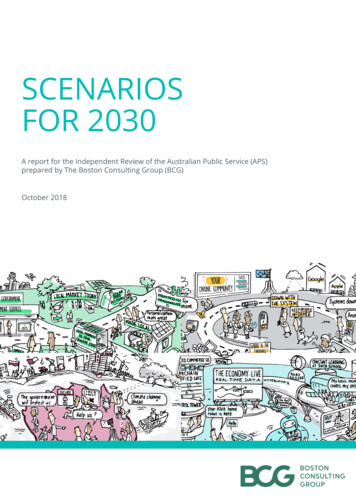
SIMPATHYIntroductionThe proportion of the global population over 65 years oldwill increase from 11% in 2010 to 22% in 2050. In Europe,advances in healthcare, education and socio-economiccircumstance mean that in most countries people cannow expect to live beyond the age of 80. However, evidence shows that the average healthy life years (HLY) forEU citizens is only 61 years meaning that many people areliving for around twenty years in sub-optimal health.Multimorbidity is defined by the World Health Organization as the co-occurrence of two or more chronic medicalconditions in one person.3 Patients with multimorbiditymay require medicines to treat each condition, whichcan lead to polypharmacy. Currently around 50 millionEU citizens are estimated to have multimorbidity. Most ofthem are 65 years and over, and this number is expectedto continue to increase.4Linking clinical and prescribing data, from a Europeancountry, has shown that 20.8% of people with two chronic conditions were taking between four and nine medicines daily. 10.1% were taking over ten medicines, andthose patients taking the most medicines are the oldest.5Data also shows that multimorbidity and polypharmacyaffects adults up to ten years earlier in deprived communities. The burden of multiple diseases can have a combined effect on physical health, the quality of day-to-dayliving and mental health.6The burden of multiple treatments can be just as problematic, causing frequent healthcare contacts and anincreasing likelihood of medicine side effects, adversedrug reactions and interactions.Non-adherence to prescribed medicines is a majorpublic health issue, intricately related to multimorbidityand polypharmacy. Research suggests that between50% and 80% of patients with chronic conditions maybe non-adherent, depending on the clinical conditionbeing studied. Non-adherence has been estimated to beresponsible for 48% of asthma deaths, an 80% increasedrisk of death in diabetes and a 3.8-fold increased risk ofdeath following a heart attack.7 It has been estimatedthat non-adherence to medicines costs the EuropeanUnion 125 billion euros annually.8PolypharmacyThere are a number of different definitions ofpolypharmacy but it is generally understood asthe concurrent use of multiple medicines by oneindividual. It can be therapeutically beneficial whenappropriate or inappropriate when not. Appropriate polypharmacy is defined asprescribing for an individual for complexconditions or for multiple conditions incircumstances where medicines use hasbeen optimised and where the medicinesare prescribed according to best evidence. Inappropriate polypharmacy is definedas the prescribing of multiple medicinesinappropriately, or where the intendedbenefit of the medication is not realised. Polypharmacy management is a wholesystems approach which optimises thecare of multimorbid patients throughmaximising benefit while reducing therisks of inappropriate polypharmacy.Non-adherenceThere are two overlapping categories ofnon-adherence to medicines. Intentional non-adherence, where theindividual decides not to follow the treatmentrecommendations perhaps because ofconcerns about the value or effectivenessof medicines, their side effects, and theinconvenience of taking the medicines at theprescribed times and frequency. Unintentional non-adherence, where theindividual wants to follow the treatmentrecommendations but is prevented fromdoing so by practical barriers which includecognitive problems, poor organisational skills,polypharmacy and difficulty accessing medicines.13
Effective Management of Polypharmacy by 203014The European Innovation Partnership on Active andHealthy Ageing has a target to increase the averagehealthy lifespan of citizens by two years by 2020.9The Partnership is seeking to identify and share goodpractice and drive research and innovation. One of thePartnership’s action groups, ‘Prescribing and Adherenceto Medical Plans’, includes a focus on multimorbidityand polypharmacy.About this handbookThe 2012 Institute for Healthcare Informatics report,Advancing the responsible use of medicines, identifiedseveral opportunities to save healthcare spendingthrough more responsible use of medicines worldwide.2Using multiple international datasets, it was estimatedthat inappropriate polypharmacy contributes to 4% ofthe avoidable costs due to suboptimal medicine use. Atotal of 0.3% of global total health expenditure, or 18 billionUS dollars worldwide, could be avoided by managingpolypharmacy correctly. Specific recommendations in thisreport were to: invest in medical audits targeting elderlypatients; develop the role of pharmacists to help patientsmanage their own medicines; support pharmacist collaboration with physicians for medication reviews; prepare atargeted medicines management plan and to encourageuse of risk stratification processes to identify patients.Focussing on change management, this handbook highlights the approaches that can help health systems todeliver effective polypharmacy management in order tohelp address the issues caused by multiple medicine usefor multiple medical conditions. Included are a range ofexamples of good practice and tools from local, regionaland national programmes.Many healthcare organisations have sought to addressthe problem of fragmented delivery of health and socialservices, through the more coordinated approach, ofintegrated care. Collaboration in this way is an essentialaspect of addressing inappropriate polypharmacy.Building on the benefits of integrated care there is nowan additional focus on population and public health inorder to minimise or prevent inappropriate polypharmacyin the first place.The SIMPATHY project was awarded funding on anEU public health call to support the use of innovative,coordinated and comprehensive community basedprevention to optimise the care of multimorbid patients.The project demonstrates the importance of a systemsapproach to developing polypharmacy managementthrough understanding the requirements of the individualpatient, carers and organisations, and the political andeconomic environment.Funded by the EU Health Programme (2014-2020) theSIMPATHY project’s goal is to stimulate and supportinnovation across the EU in the management of polypharmacy and adherence with specific focus on addressing inappropriate polypharmacy in the context of quality,economic and political factors.The content is informed by the findings of the SIMPATHYcase studies,10 analysis of SIMPATHY change managementtools,11 SIMPATHY literature review and benchmarkingsurvey,12 and SIMPATHY Delphi study.13SIMPATHY confirms the findings of Advancing theresponsible use of medicines,14 that there are currentlytoo few polypharmacy management programmes. Thereis a consensus among all stakeholder groups for the needto address the issue of inappropriate polypharmacy. Thereis a recognition of the quality of existing programmes, butsignificant concerns expressed regarding the challengeof how to initiate polypharmacy management in countries,where services do not exist, and how to expand whereservices are concentrated in a small area. The projectdemonstrates how change management can be usedas a successful approach to help initiate and implementeffective polypharmacy management at scale.
SIMPATHYCaseTHE SIMPATHY PROJECTCase StudiesIn depth studies to understandcurrent practices showcasingdifferent approaches topolypharmacy managementin the EU.StudiesManagegearkingchen mChanBBenchmarkingEurope wide regional andlocal benchmarking surveyidentifying strategies ofpolypharmacy and nonadherence management.chesoant ApprmeChange ManagementApproachesDevelopment of strategies andtools to support innovation inpolypharmacy and adherencemanagement.15QualityManagement of polypharmacyis an essential element of patientsafety in an integrated caresetting making a significantcontribution to well-beingEconomicPrevention of harm due tomedicines can reduce demandson the healthcare systemreducing threats to servicesustainability1. Use a systems approach that has multidisciplinaryclinical and policy leadership2. Nurture a culture that encourages and prioritisesthe safety and quality of prescribing3. Ensure that patients are integral to the decisionsmade about their medicines and are empoweredand supported to do soPoliticalDemographic changes aredriving up public awarenessof polypharmacy issues,demanding a response frompoliticians and policymakers4. Use data to drive change5. Adopt an evidence based approach with a biastowards action6. Utilise, develop and share tools to supportimplementation
Effective Management of Polypharmacy by 2030PERCENTAGE OF PEOPLE BY AGE GROUPON MULTIPLE MEDICINES100%90%Percent of MYE population80%70%60%50%40%30%20%10%0%00-04 05-09Num. medicines1610-1415-190120-24 25-29 30-34 35-39 40-44 45-4923456750-54 55-59 60-64 65-6989101170-7475-7980-8412131485 15 FRAILTY AND THE NUMBER OF MEDICINESMORE FRAILTYFRAILTY1.5 XOR MOREMEDICINES5MORE MEDICINESFRAILTY2.0 X10 OR MOREMEDICINES
The case for appropriatepolypharmacy management
Complex careEconomicThe shift in demographics to an aging population withincreasing multimorbidity leads to increasing complexityin care. Health inequalities can add to this complexity,where long-term illness can present 10-15 years earlierin the most deprived groups.Increasing demand on constrained health budgetscreates the need for change to ensure that medicinesand healthcare resources are used optimally.QualityMultimorbidity and polypharmacy are a widespreadand growing challenge, adversely affecting the qualityof life of EU citizens and increasing pressures on healthsystems. The solutions require political and policysupport for change and improvement.A growing population with multimorbidity using multiplemedicines (polypharmacy) for long periods of their livesare at increased risk of adverse events, error and harm.Politics and policy
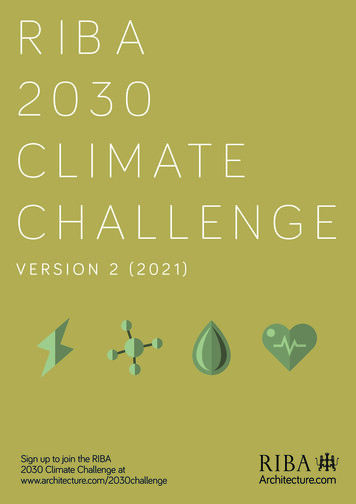
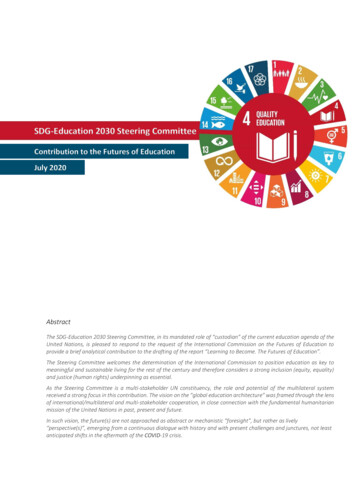
SIMPATHYComplex careThere are many factors that are creating favorablecircumstances to address the polypharmacy challenge.Resources are constrained and under increasing demandas people live longer with multiple morbidities. Thereis a focus on improving safety and quality of healthcareand avoiding harm. Workforce pressures mean thathealthcare professionals and policymakers are moreopen to multidisciplinary working.Polypharmacy is a growing problem as populationlongevity and the incidence of multimorbidity increase.Although not exclusive to the elderly, polypharmacy inolder people presents particular challenges. Physiological decline and frailty, combined with inappropriate polypharmacy, increases the potential for harm in older people. This is compounded by the risks of non-adherence tocomplex treatment regimens.15 These factors combine toincrease the likelihood of morbidity, unplanned admission,readmission and prolonged length of stay in hospital.Modern prescribing is largely based on single diseaseevidence-based guidance which does not generally takeaccount of multimorbidity, despite this being the norm inthose over 65 years.6 In contrast, polypharmacy management aims to optimise outcomes by ensuring that throughout life people are prescribed the safest and most effectivecombination of medicines to manage their multimorbidityand to maintain well-being for as long as possible.Caring for patients with multimorbidity treated withpolypharmacy is a widespread and increasingly commonglobal challenge. Polypharmacy management involvescomplex decision making and requires the combinedknowledge of physicians, pharmacists and nurses supported by informed patient interaction.Good communication and accurate sharing of information is essential, facilitated by information technologysystems that support cohesiveness and integrationacross health and care systems. Re-design of servicesto proactively cope with an increased clinical workloadrelated to polypharmacy can relieve pressures on services as a whole. Appropriate polypharmacy avoids unnecessary work for all health and care professionals andcarers at the same time as improving patient outcomes.Consequent improved adherence with medication canalso contribute to improve outcomes.Given this evidence, the case for effective polypharmacymanagement is quite clear, but in a complex healthcaresetting with many competing priorities it is useful tooutline the quality, economic and political reasons whythis should be prioritised within every EU country’s healthpolicies and plans for active and healthy aging.The SIMPATHY benchmarking study set out to identifythe status of polypharmacy management across the EU,gathering more than 1,000 responses from a spectrum ofstakeholders across 26 EU countries.12 Although responseswere mainly from clinical practitioners, 10% of responseswere from patients.Across the EU a lack of understanding was shownregarding the issue of polypharmacy, in terms of its definition, and any consistent framework against which tomeasure progress. This finding was not confined to anyone stakeholder group but applied equally to clinical andnon-clinical stakeholders, and patients.This survey sought to benchmark key indicators of performance relevant to effective polypharmacy management.The findings clearly illustrated that there is an absence ofknowledge and meaningful metrics across all countries andstakeholders. Of particular note was the almost completelack of awareness of the health economics related to appropriate medicines use. However, more than 60% of respondents thought that health economic data would be useful.The existence of programmes to manage polypharmacy,where more than 10% of the country respondents indicatedthis, were restricted to the UK, Sweden, Portugal, Spain,Germany and the Netherlands. The activities of the reportedprogrammes were: prescription reviews (83%); treatmentreviews (77%) and clinical medication reviews (71%).QualityPeople with multimorbidities, taking multiple medications(polypharmacy), are at increased risk of potentially avoidable medicine related issues. All medicines are associatedwith a level of risk and it is estimated that worldwide, 3-6%of all hospital admissions are attributed to medicines, andfigures ranging from 2-19% have been recorded in the USAwith studies in the UK reporting up to 11%.1,16-18Over half of medicines-related hospital admissions in theover 65s on multiple medications are preventable, with four19
Effective Management of Polypharmacy by 2030groups accounting for 50% of these (antiplatelets, diuretics,anticoagulants and non-steroidal anti-inflammatory drugs).1Prescribing errors are common in all healthcare settingsand another major cause of harm. The UK GeneralMedical Council in 2012 reported that one in 20 prescriptionsin primary care contained an error with a higher prevalenceassociated with prescriptions for the elderly and thosetaking 10 or more medicines.19 In hospital prescribing, errorsare also a common occurrence, affecting 50% of hospitaladmissions.20 When patients transfer between health andsocial care settings evidence shows that 30% to 70% ofpatients experience an error or unintentional change totheir medicines.21 Taking multiple medicines, long term,presents difficulties for individuals and carers managingcomplex medicine regimens with evidence that between30-50% of these medicines are not taken as prescribed.2220The SIMPATHY literature review confirmed that there isevidence to support the principle that medication reviewsreduce inappropriate polypharmacy.23 Recent researchhas also begun to show improvement in outcomes dueto polypharmacy management, including a reduction inhospital admissions.24 The SIMPATHY literature reviewidentified that there are guidance documents availablerelating to the management of polypharmacy in only 5 ofthe 28 EU countries, with only the guidance documentsfrom Scotland, the Netherlands and Germany scoring themaximum on the AGREE II-GRS criteria for quality.25There remains an evidence gap, whilst research catches upwith this fundamental shift in healthcare priority. Safety is amajor concern in modern healthcare and addressing issuesrelated to inappropriate polypharmacy should form part ofthis. The literature review supports the principle that it isimportant to adopt an evidence based approach, but with abias towards action where the evidence is limited. It shouldalso be recognised that there is further emerging evidenceto support polypharmacy management research, that is inprocess, and yet to publish.EconomicThe demand for health and social care is increasingglobally in response to demographic shift, pharmaceutical and technological advances. This creates budgetary pressure between the healthcare needs and theresources available in most EU countries. Constrainedbudgets call for the prudent use of resources to gainthe best possible outcomes from investment. Evidencebased approaches that deliver clinical and cost-effectivecare are of interest to all governments and this has beenincreasingly supported by policy documents.26Throughout Europe, 16% of total government expenditureis dedicated to healthcare, ranging from 6% in Cyprus to22% in Switzerland.4 After inpatient and outpatient care,pharmaceuticals represent the third largest expenditure inhealthcare and accounted for around a sixth of total healthexpenditure in 2014, not taking into account spending inhospitals.27 In 2014 the total pharmaceuticals bill across theEU was 200 billion euros and the average spend per head ofpopulation was 402 euros with wide variation between countries, from 201 euros in Denmark to 551 euros in Germany.Medicines are one of the highest costs in EU healthcaresystems and are consequently one of the most commonlytargeted areas for efficiency savings. Post financial crisis,between 2009 and 2014, expenditure on pharmaceuticalsdropped by 1.1% in real terms on average in the EU, mainlytriggered by cuts in public spending. However, there aresigns that spending is increasing again in some countriesdue to the steep growth in spending on high cost medicinesto treat, for example, hepatitis C or oncological conditions.27Effective polypharmacy management can deliver improved safety and health outcomes plus economic benefits. Avoiding harm from adverse drug events improvespatient outcomes in addition to delivering economicbenefit through f
To err is human - building a safer health system. Washington, D.C. National Academy Press; 2000. ISBN: -309-06837-1 c. Malhotra A, Maughan D, Ansell J, Lehman R, Henderson A, Gray M, Stephenson T, Bailey S. Choosing Wisely in the UK: the Academy of Medical Royal Colleges' initiative to reduce the harms