Transcription
Aortic AneurysmsHow Big is the Problem? Incidence is increasingCutting EdgeTechnology for AorticAneurysms UnityPoint Health Methodist, Peoria, ic AneurysmsHow Big is the Problem? 1 - 5 % of general population affectedAAA: 100,000 – 250,000 new cases eachyear in the U.S.TAA: approximately 15, 000 new cases eachyear43,000 – 47,000 deaths per year (CDC)Twice as many deaths from thoracic aorticdissection and rupture than abdominalNormal Size of Aorta10th – 18th leading cause of death inthe USA2/3 of patients who suffer a rupturedaneurysm will die before evenreaching the hospital.90% mortality with ruptured AAASource: Society of Thoracic SurgeonsSize in ingDiaphragmatic 2.43-2.69Source: J Vasc Surg 1991:13:452-8 and 2010 Guidelines TAD.Aortic Aneurysm (AA)Aortic Aneurysm (AA) Abnormal dilation of the aortic wallthat alters the vessel shape andblood flowThoracicTAAAbdominalAAA50% increase in the diameter of avessel in comparison of it’s expectednormal With gradual enlargement, the aortabecomes increasingly weakened,leading to possible dissection andrupture.1
Abdominal AneursymThoracic Type A AneurysmSmokingRisk Factors HypertensionIncreasing AgeSmokingCocaine or otherstimulant useWeight lifting or othervalsalva maneuverTraumaDeceleration ortorsional injury Family historyMarfan’s syndromeLoeys-Dietz SyndromeTurner SyndromePheochromocytomaCoarctation of theaortaBicuspid valveRisk Aortic aneurysm disease is rareunder the age of 50.Mean age of patient undergoingrepair is 70. Current smokers are seven timesmore likely to develop AAAthan non-smokers.Former smokers are three timesmore likely.Strongest modifiable risk factor fordevelopment of aneurym.Precipitating Events of onset ofacute aortic dissection Extreme exertionWeight lifters (Yale)Extreme elevation in BP Episode of severe emotional upset2
DissectionAortic Aneurysm Rupture A tear in the vessel wall near or atthe location of the ballooning of theweakened area of the aorta allowingblood to hemorrhage into the chestor peritoneal cavityRupture carries a 90% mortality Tear in the intimallayer of the aortic wallBlood passes into theaortic media throughthe tear separatingthe intima from thesurround mediaand/or adventitia,creating a falsechannel within theaortic wallDissection Acute DissectionDiagnosed within 14 days of the onsetof symptomsThe risk of death is greatest during thisacute period A Silent Disease Often discovered on a routine CXR orabdominal sonogram Chronic DissectionDiagnosis after two weeks of the onsetof symptoms S/S depend where the dissectionoccurs and what area is not gettingoxygenConfused with:Kidney stonesGallstonesParalysis -- think neuro diagnosisMyocardial infarctionOnly 5% of patients are symptomaticbefore an acute aortic event.The other 95%, the first symptom isoften deathAA Dissection Symptoms“The Great Imitator” 40% of individuals are asymptomaticat the time of diagnosisAA Symptoms Abrupt onset of excruciating pain inchest, back, or abdomenAscending DissectionRetrosternal pain that is not exertional innatureDescending DissectionInterscapsular chest painSevere flank painEpigastric pain Ripping, tearing, stabbing and orsharp quality of pain3
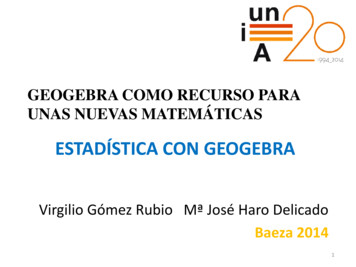
High Risk Examination Features Pulse deficitSystolic BP limb differential 20mm HgFocal neurologic deficitMurmur of aortic regurgitationHypotension or shock stateThoracic Dissection Symptoms Severe tearing pain of sudden onsetPain has a tendency to migrate fromits point of origin to other locationsfollowing the path of dissection2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines forthe Diagnosis and Management of Patientswith Thoracic Aortic DiseaseDeveloped in partnership with the American College of CardiologyFoundation/American Heart Association Task Force on PracticeGuidelines, American Association for Thoracic Surgery, AmericanCollege of Radiology, American Stroke Association, Society ofCardiovascular Anesthesiologists, Society for CardiovascularAngiography and Interventions, Society of InterventionalRadiology, Society of Thoracic Surgeons, and Society for VascularMedicine.Endorsed by the North American Society for CardiovascularImaging.Source: 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STA/SVM Guidelines for TAAYou suspect a dissecting/rupturinganeurysm .NowWhat?Source: 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STA/SVM Guidelines for TAA4
Rapid Triage & Treatments DiagnosticsAortic Center Aortic PathwayMethodist Hospital Houston. TX12 Lead EKG to r/o STEMIChest x-ray – not very helpful as noabnormalities notedCT scan Aortic Dissection Classification:DeBakey and Stanford ClassificationsDissections62% are Type AType B are typically older than Type AType A Immediate operation room interventionType B Medical managementNote: Figure 20 in full-text version of TAD Guidelines. Reprinted with permission from The Cleveland Clinic Foundation.Acute AoD Management PathwayAcute AoD Management PathwaySTEP 2: Initial management of aortic wall stressSTEP 2: Initial management of aortic wall stressIntravenous rate and pressure controlNoRate/Pressure Control1Intravenous beta blockadeor Labetalol(If contraindication to beta blockadesubstitute diltiazem or verapamil)Hypotensionor shock state?Anatomic based managementType A dissectionYes1Titrate to heart rate 60 Pain ControlIntravenous opiatesAnatomic based management22Urgent surgical consultation Arrange for expeditedoperative managementIntravenous fluid bolus Titrate to MAP of 70mm HGor Euvolemia(If still hypotensive beginintravenous vasopressor agents)Titrate to pain controlSystolic BP 120mm HG?Type B dissection1 Titrate to MAP of 70mm HGor Euvolemia(If still hypotensive beginintravenous vasopressor agents)2BP Control3Titrate to BP 120mm HG (Goal is lowest possibleBP that maintains adequate end organ perfusion)3Review imaging study for: Pericardial tamponade Contained rupture Severe aortic insufficiencyEvaluate etiology ofhypotension Review imaging study forevidence of contained rupture Consider TTE to evaluatecardiac functionSecondary pressure controlIntravenous vasodilatorIntravenous fluid bolus3Urgent surgical consultation5
Indications for AA repairAbdominalThoracic Indications for AA repairSymptomaticDiameter 5.5 - 6 cmDiameter 4.4 - 5 cm associated withgenetic disorder(Marfan’s syndrome)Symptoms suggesting expansion orcompression of surrounding structures Diameter 5 cmDiameter 4 cm needs regular follow upDiameter 4 – 5 cm, management iscontroversialSize --- It really does matter!Indications for AA repairAnnual Incidence of RuptureBoth: TAA & AAA Rapidly expanding aneurysms Symptomatic aneurysm regardless of sizegrowth rate 0.5 cm/year At 6 cm – aorta becomes a rigid tubeIt cannot stretch in systoleResults in high wall stress34% risk of ruptureTAA at 6 cmAAA at 7 cmRepair of AATraditional:Surgical Repair for AAAEvolving Trend: 50 years since first repairmortality 4% Significant short & long-term morbidity Causes of aneurysm related death welldefined AverageOpen surgicalrepairEndoluminalgrafting (ELG)6
Functional Outcome after Open Repairof Abdominal Aortic AneurysmOperative MortalityMean LOSICU LOSAmbulatory Post-opDecreased FunctionalityTime to RecoveryUnrecoveredAgain?Evolving Trend:AbdominalEndovascular Graft4% (154 pts.)10.7 days4.6 days64% (25 mos.)33%3.9 mos.33%18% - NoSynthetic, twopiece bifurcatedgraft, that lines theaorta and extendsfrom below therenal arteries intoboth the iliacarteriesWilliamson, et al – Portland, OregonJ Vasc Surg 2001;33:913-20Abdominal EndovascularGraft First implanted1997FDA approvedNovember 2002Gore ExcluderEndologix28 french7
AneurRxTalentEndurantMedtronicAneurysm Before & AfterEndograftingBranched Endografts Pre-attached limbsor cuffs targeted forthe aortic branches.Cuffs are deployedin the targetedbranchTAG Thoracic EndograftTEVAR: Thoracic Endovascular Aneurysm RepairINDICATIONS:Thoracic AneurysmsAcute and Chronic Thoracic DissectionTEVARThoracicTAA2003Starting treating TAAwith endografts inPeoria2005 FDA approved8
Morbidity of Open RepairGore TAGDeploys from the middle to the endThis prevents windsockWindsock can move graft 3 – 5 cmThoracicAortaAbdominalAortaApproved by the FDA on March 23, 2005.Medtronic TalentStent GraftPush pull method to openCan migrate during cardiaccycle while deploying.Use Adenosine to stop heartwhile deploying.Deploys proximal to distalHybrid Open/EndovascularAneurysm RepairDefinition of HybridAn offspring resulting from cross-breeding Hybrid approach: combinesstandard operative approaches andendografts and/or conduitcreation/de-branchingDe-branching: the transposition ofthe origin of critical branch vessels tofacilitate a seal zone9
Aortic DebranchingExtra-anatomical BypassCriado, EVToday Aortic Debranching: The transposition of the origin of thecritical branch vessels to facilitate a seal zone.Aortic Debranching is used to provide blood flow aroundthe arch arteries that become occluded when a TAG isplaced in the ascending aorta.Photos courtesy ofDr James Bertram Willliams A board-certified cardiothoracic andvascular surgeon Peoria, ILPrincipal investigator in a number ofU.S. clinical device trials forendovascular devices.Endovascular Therapies FellowshipTraining (ETFT) Program, a six-weekvisiting fellowship programwww.etft.orgTAG inserted covering the subclavian artery.Pre TAGPost TAG10
Aorto bi-carotid bypass:Y graft to the left & right common carotidsand the infrarenal abdominal aortaPre-opPost-opHybrid:Bentall’s Procedure with TAGPre TAG & BentallBentall Ring & TAGTAG prior to BentallBentall and TAG POD #2lateral Bentall & TAG11
Type A Dissection Acute Type B dissectionImmediate operating roominterventionFollow-up after 4 y.Kato N, et al. J Vasc Surg 2003;38:1130-1Acute, Uncomplicated Type BDissectionsAcute Type B Complicated Dissection Goal is to have the true lumen re-expandand the false lumen to resolveNeed to understand anatomy of thedissection to know what the true lumen vsfalse lumen is feedingPrefer to wait 8 - 9 days to treat as willhave less complicationsIf repair 3- 5 days after dissectionsignificant re – dissectionIf wait longer than 9 days, then the truelumen may not re-expand Medical management is currently themost appropriate treatmentAcute 14 daysChronic Type B DissectionAcute Type B DissectionPreCourtesy Rodney White, MD2d Post9 mos15 mos4-26-045-2-045-4-041 d post5-7-044 d post5-11-048 d postCourtesy Rodney White, MD12
Nursing CarePreop DiagnosticsPreoperative Care To measure length & diameter of the arteriesUsually AM admitHydrate with NS at 125 -150 ml/hourIf Creatinine 1.6 may giveMucomyst or Bicarbonate infusion (3amps Bicarb/1000ml D5W at 3 ml/hrx 6 hours --- start 1 hour preop)Permit to include possible resectionof aortic eliac axisSMA Duplex scanCT (without contrast)Aortogram(with calibrated catheter)Spiral CTIntravascular ultrasound3-D CT ReconstructionIntravascular UltrasoundProximal NeckCephaladneckKinkingIMALengthLumbarsIliac arteryInt. 3
TAAPre-proceduralAssessmentsPostop Nursing CarePostopertative Assessment,Complications & CareManagement TAG/ELG vs DebranchingTAG with debranchingTAG & ELG Hourly neurovascularchecks to extremitiesImmediate notification ifdecreased movement orsensation in legs-- mayneed to insert cerebralspinal catheterLactate levelsPulmonary Toilet Volume resuscitate. KeepCVP highIf hypotensive &hypovolemic, grafts canclot offTreat like a trauma or openabdominal surgery --- treatwith hypotentsion withfluids not inotropes untiltanked up.If Carotid arteriesbypassed, hourly neurochecks EndoleaksExtremity IschemiaUrinary RetentionRenal FailureBowel IschemiaAbdominal Compartment SyndromsSpinal Ischemia (TAA)StrokeMetabolic AcidosisRespiratory ComplicationsEndoleakType IAneursym sac remains pressurizedEndoleak SignificanceEndoleak Endopressure ProtectionPerigraft Flow/Endoleak:Definitions*Attachment leakType IIBranch flowType IIIDefect in graft ormodular disconnectionType IVFabric porosity* White et.al., Endoleak Classification,Journal of Endovascular Surgery, 1998;5:305-30914
Post-operative Detection ofEndoleakAssessment of aneurysm diameter & volume Abdominal four view xrays POD #1 CT with 3-D reconstruction Duplex Scan For severe endoleak hemodynamicinstabilityExtremity Ischemia Urinary Retention Due to enlarged prostateDiscontinue foley in OR orimmediately upon admission to unitto prevent urinary retentionDue to thombosis of graft or groinhematoma at insertion siteAssess pedal pulses, sensation, color, andtemperature of extremities every 15minutes x 4 and then hourly.Assess for pain in the hip(s) or leg(s)during walkingAnkle brachial indexes bilaterally POD #1Renal Failure Due to occlusion of renal arteries bygraftDue to atheroembolismDue to contrast induced nephropathy200 – 250 mg of contrast used perprocedure caseHYDRATE preoperativeBowel IschemiaRightRenalArteryLeft RenalArtery Due to occlusion or hypoperfusion ofmesenteric artery ischemiaDue to atheroembolismWill do bypass if think graft may covermesenteric teryMesenteric Artery ischemia Paralytic ileusGastric distentionRetroperitoneal bleedingMesenteric ischemiaDrugs (narcotics)15
Bowel Ischemia Assess for Loose stool or diarrheaBright red blood per rectum, bloodstreak stoolAbdominal pain out of proportion tophysical findings Mesenteric ischemiaDecompress bowel with nasogastrictube and keep NPO Early diagnosis and treatment areessential to lower mortalityMortality generally exceeds 50%When ischemia is prolonged,irreversible intestinal necrosis mayoccur within hoursEmergency abdominal exploration isindicated if bowel necrosis issuspectedSigns of Intra-abdominal hypertension (IAH)and Abdominal Compartment SyndromeIntra-abdominal hypertension (IAH) andAbdominal Compartment Syndrome(ACS) Cardiac GILow CO with CVP/PAD Renal PulmonaryNausea/vomitingAbdominal painAbdominaldistensionLow urine output NeuroDysnpnea tidal volumes intrathoracicpressuresSpinal Cord Ischemia (SCI)IAH and ACS In high risk patients, measure intraabdominal pressure (IAP) via bladderpressure measurementsGet baselineMeasure every 2 – 6 hours IAH IAP 12 mmHgACS IAP 20 mmHg andassociated organ failure/dysfunction ICPAnxietyConfusionLethargy The spinal cord like the brainNo room for anything but thecord and CSFAnd it is unyielding to increasedspinal pressures ParalysisOccurs in about 3 - 6% of allrepairs of the descendingthoracic aneurysmDue to interference in the bloodsupply to the spinal cord ThoracicAortaAbdominalAortaMay occur immediatelypostop or from 1 – 21 days16
Spinal Cord Ischemia Ischemia to the cordLeads to cord edemaCan cause the lumbar ICP to rise &impede normal flow of CSF within thespinal cana Thoracic or lumbar spinal corddamage causes paraplegiaSimilar to muscular ‘compartmentsyndrome’At risk for permanent andtransient paraplegia Spinal Cord Ischemia (SCI) The mechanisms leading to SCI:The interruption of multiple branchvessels that provide spinal cordperfusion. Hypotension - MAP 70 - 90Periop &/or postopCan be a precipitating factor causingSCIPrevention of Spinal Cord IschemiaComplicated Type B dissectionHybrid aortic proceduresAortic transectionChronic renal failureSmoking Treatment Spinal Cord IschemiaLumbar Cerebral Spinal Fluid DrainDrainage of the lumbar CSF canreduce the risk of cord damage whenreducing pressure to 7 – 10 mmHgKeep MAP 90 - 99 mmHg Prevent Hypotension MAP 70 - 90Treat with fluids to keep CVP 6Also called:Lumbar drain, Lumbarsubarchonoid catheter,intrathecal catheter, CSF drain Placed in the LumbarSubarachonoid spaceUse for those at high risk forparaplegiaPrevious infrarenal repairLong segments of spinal cordSpinal pressure 10 cm H2017
Lumbar CSF Drain SafetyLumbar Cerebral Spinal Fluid DrainPurposePreventparaplegia Adjust drip chamberheight until black level isat the proper drainageresistance. Frequently 10cmH20The “Zero” reference point mustbe positioned at the level of thecatheter insertion site Spinal Ischemia Assessment Record CSF output hourlyNotify MD if CSF drainage is 20 –30 ml/hrNote color of CSFHourly spinal cord assessment forchanges in sensation and/ormovementCSF Drainage InfectionOverdrainageSubdural hematomaHerniation Spinal cord hematomaHeadachePneumocranium (from air enteringsystem)Maintain CSF pressure 10 – 15mmHg for the first 24 hoursThen let rise to 15 mmHGIf CSF pressure goes up abovenormal, blood flow to the spinal cordgoes down, resulting in cordischemiaComplication of CSFLumbar Drain OverdrainageComplications of CSF Drain Place CSF transducer on opposite side ofbed as hemodynamic pressure monitoringMust be a nonflush pressure systemTurn drainage system off when gettingpatient up to chairLevel after repositioning patientRemember to unclampAseptic technique is a must! Low pressure headacheRadiculopathyPneumocephalusSagging Brain /intracranialhypotensionHemorrhageSubdural, intraduralHematomaCranial nerve palsiesTensionPneumocephalusBrainstem herniation18
Post removal of Lumbar drain Cap 24 hours prior to removalAssess for lower extremity weaknessor loss of sensationSCI can occur up to 30 days post op.Teach patients to come to EDimmediately for aggressivetreatment if they notice any change,numbness, or weakness in their legs.Respiratory Complications Due to general anesthesia andsmokingIncentive Spirometry every 1- 2 hourswhile awakeAggressive ActivityHOB 30oChair when stableAmbulate 200’ evening of surgeryThen Ambulate 4- 6 times per day Left Pleural EffusionSomething may be bleedingType A Lactic AcidosisOngoing Metabolic Acidosismeans something is not being perfused Serum lactate levels used to assessthe acid-base state and adequacy oftissue perfusionBy product of anaerobic metabolismif tissue hypoxia existsStroke 4- 7% riskRoutine neuro checksAdmission ABGsWhat would you do?Patient Aph7.29pCO260p02132TCO231O2 %98BE-1Patient B7.33411002298-6The Value of LactateSerial lactate levels predictor of perfusionNormal 2.5mmol/LMild acidosis 2.5-4.9mmol/L(mortality 25-35%)Moderate acidosis 5.0-9.9mmol/L(mortality 60-75%)Severe acidosis 10mmol/L(mortality 95%)Shoemaker, WC et al. Textbook of critical care. 1995. WB Saunders19
Serum Lactate levels Serum Lactate levels every 4 hoursx 24 hoursLevel will be around 4 – 5mmol/L onadmissionLactate levels need to decreaseMay be the first indication thatsomething is wrongFollow-upDischarge References CT scan at 1, 2, 6, and 12 monthsand then annually to assess for aorticgrowthTeachingAvoidance of exertional activitiesBetablockers blunt pressure spikesAvoidance of extreme emotional upsetsAbdominal – POD #1 from CVICUThoracic -- POD #2 or 3Teaching10 days post procedure the patientshould be back to normal activitiesMRI conditional up to 3 Tesla Desai ND, Pochettino A, Szeto W, et al. Thoracic endovascular aortic repair:Evolution of therapy, patterns of use, and results in a 10 year experience. JThorac Cardiovasc Surg. 2011;142(3):587-594.Elefreriades JA, Farakas EA. Thoracic aortic aneurysm: Clinically pertinentcontroversies and uncertainties. J Am Coll Cardiol 2010;55:841-856.Gallager H. (2010) Intra-Abdomonial Hypertension. AACN Adv Crit Care:21(2):205-217.Hiratzka LF, Bakris GL, Beckman JA et al. 2010ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STA/SVM guidelines for the diagnosisand management of patients with thoracic aortic disease: a report of theAmerican College of Thoracic Surgery, American College of Radiology, AmericanStroke Association, Society of Cardiovascular Anesthesiologists, Society forCardiovascular Angiography and Interventions, Society of InterventionalRadiology, Society of Thoracic Surgeons, and Society for Vascular Medicine.Circ 2010;121:eMethodist DeBakey Heart & Vascular Center. DeBakey Cardiovascular Journal.July – Sept 2011;7(3):1-56. (17 articles in this journal relating to endovascularstenting)Moser D, Riegal B. (2008). Cardiac Nursing: A companion to Braunwald’s HeartDisease. St Louis MO: Sanders Elsevier.Steuer J, Eriksson MO, Nyman R, Bjorck M, Wanhainen A. Early and long-termoutcome after thoracic endovascular aortic repair (TEVAR) for acutecomplicated type B aortic dissection. 2001;41:318-323.Svensson LG, Kouchoukos NT, Miller C et al. Expert consensus document onthe treatment of descending thoracic aortic disease using endovascular stentgrafts. Ann Thorac Surg 2008;85:S1-41.Ullery BW, Cheung AT, Fairman RM, et al. Risk factor, outcomes, and clinicalmanifestations of spinal cord ischemia following thoracic endovascular aorticrepair. J Vasc Surg 2011;54:677-684.20
4 High Risk Examination Features Pulse deficit Systolic BP limb differential 20mm Hg Focal neurologic deficit Murmur of aortic regurgitation Hypotension or shock state Thoracic Dissection Symptoms Severe tearing pain of sudden onset Pain has a tendency to migrate from its point of origin to other locations following the path of dissection