Transcription
Aortic Dissections:Treatment andManagementPresented byClyde Marquis MSN, APRN, ACNP-BC
rtoon.jpg
Disclosures
Anatomy of the l-payers/
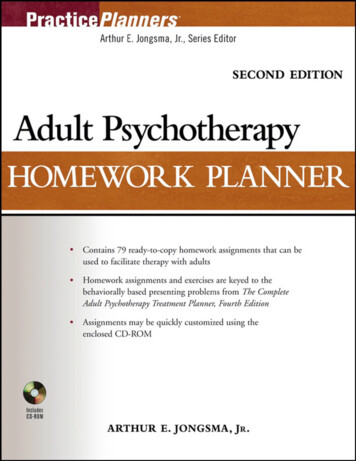
Aortic DissectionAortic dissectionis defined asseparation of thelayers within theaortic wall. Tearsin the intimal layerresult in thespread ofdissection(proximally ordistally)secondary toblood entering ent/uploads/2007/12/aorticdissection.jpg
Case courtesy of Dr Vincent Tatco, https://radiopaedia.org/" Radiopaedia.org /a . From the case ahref "https://radiopaedia.org/cases/48452" rID: 48452 /a
PxPkY4bPeddq*Rdvk6RA3/typeadissectionct.jpg
Aortic Dissection Epidemiology In the United States, aortic dissection is an uncommon disease.The incidence of aortic dissection is estimated to be 5-30 casesper 1 million people per year.Aortic dissection occurs once per 10,000 patients admitted to thehospital; approximately 2000 new cases are reported each year inthe United States.Aortic dissection is more common in blacks than in whites and isless common in Asians than in whites.Aortic dissection is more common in males than in females, with amale-to-female ratio of 2-3:1.Approximately 75% of dissections occur in those aged 40-70years, with a peak in the range of 50-65 years.Patients with Marfan syndrome present earlier, usually in the 3rd or4th decades of -overview#a0156 updated December5,2014
Aortic Dissection - Symptoms Sudden onset of severe and tearing chestpain, although this description is notuniversal. Some patients present with only mild pain,often mistaken for a symptom ofmusculoskeletal conditions located in thethorax, groin, or back. Some patientspresent with no pain. The pain is usually localized to the front orback of the chest, often the interscapularregion, and typically migrates with spreadof the dissection.
Aortic Dissection - Symptoms The pain of aortic dissection is typicallydistinguished from the pain of acutemyocardial infarction by its abrupt onset,although the presentations of the twoconditions overlap to some degree and areeasily confused. Aortic dissection can be presumed inpatients with symptoms and signssuggestive of myocardial infarction butwithout classic ECG findings. NSTEMI vs Aortic Dissection
Aortic Dissection – Laboratory Aortic dissection is usually diagnosedusing imaging techniques before the resultof blood work is interpreted. BUN and creatinine levels may beelevated, possibly indicating involvementof the renal arteries or prerenal azotemiaresulting from blood loss or associateddehydration (mainly when the BUN-tocreatinine ratio is 20). Cardiac enzymes are elevated if thedissection has involved the coronaryarteries and caused myocardial ischemia.
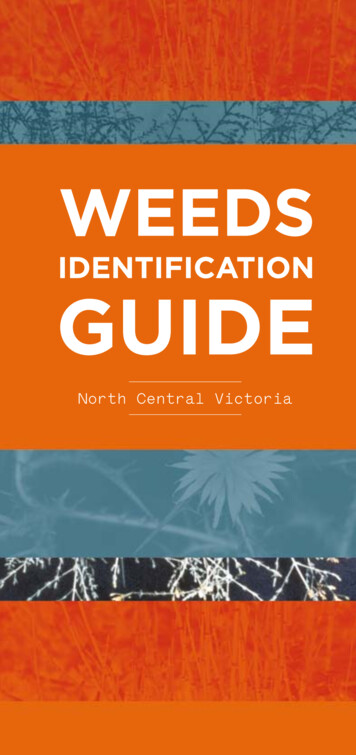
Aortic Dissection - Diagnostic tools Aortic dissection can be diagnosed with imaging Chest x-ray is the initial imaging technique andmay or may not reveal any abnormality. Widening of the mediastinum is a classic finding Hemothorax may be evident if the dissection hasruptured An absence of mediastinal widening is observedin 40% of patients. With type A, an abnormalaortic contour is observed in a minority ofpatients. An absence of both is observed in 20%of patients. Other chest radiograph findings include deviationof the trachea to the right or pleural effusion. No abnormality is observed in 12% of patients.
rticaneurysm/
Chest radiograph demonstrates a large aneurysm of the thoracicaorta. Note the deviation of the trachea to the right. Contrastenhanced CT of the aorta confirms the radiographic findings andshows the extent of the aneurysm , as it involves the entire thoracicaorta as well as the abdominal aorta. A small right pleural effusionis also -aneurysm-3
Aortic Dissection - Diagnostic tools CT scanning with contrast is used mostfrequently. Echocardiography is an important imagingmodality for detecting aortic dissection. MRI is as accurate as CT scanning in thediagnosis of aortic dissection. Twelve-lead ECG most frequentlydemonstrates a nonspecific abnormalityand normal results .
culum/Surgery/dissecting aorta.htm
culum/Surgery/dissecting aorta.htm
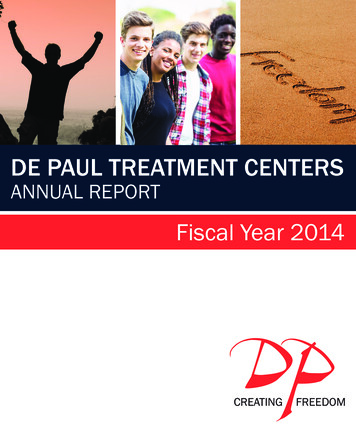
Classification of aortic 108/5/628
Aortic Dissection - Treatments Admit to ICU for assessment of hemodynamic stability,pain control, BP control and consult CV surgeon. Intubate hemodynamically unstable patients. Control BP: Systolic 100–120 mm Hg, or lowest tolerated IV beta blocker (Esmolol and Labetaolol) to achieve HR60, alternatively can use a calcium channel blocker(Cardene, Verapamil, Diltiazem) Consider placement of central venous catheter and/orarterial line For medical management start oral medications as soonas possible for B/P and pain control Changing Esmolol to Labetaolol after 24 hours can savedthe hospital thousands of dollars
Aortic Dissection - TreatmentsIf hypotensive, avoid inotropes.Determine etiology of hypotension: Rupture Blood loss Tamponade Heart failure Not titrating medications correctlyCareful observation: Neurologic assessment for changes inmentation and neurologic signs Evidence of organ dysfunction, foley catheterto follow urine output Pain control
Type A Dissection Treatment Surgery is the treatment of choice fordissections of the ascending aorta (80%treated surgically) Dissection of the ascending aorta is asurgical emergency because of risk ofaortic regurgitation, cardiac tamponade,myocardial infarction Hemorrhagic stroke is relativecontraindication to surgical repair due torisk posed by intra-operativeanticoagulation
Surgical indications forType B Dissection Extension of dissectionContinued aortic expansionImpending ruptureOcclusion of major aortic branchInability to control painBleeding into pleural space
Considerations for Surgical, Medical, andInterventional Therapyin Aortic Dissection SurgerySurgery Treatment of choice in acute type A dissection Acute type B dissection complicated by the following:-Retrograde extension into the ascending aorta-Rupture or impending rupture (stent-grafts?)-Progression with compromise of vital organs (stenting?)Medical therapy Treatment of choice in uncomplicated type B dissection Stable, isolated arch dissection Stable type B dissection (chronic, 2 weeks of onset) If surgicalrepair of aneurysm is indicated, do not delay repair toevaluate for CAD and valvular dysfunction.Nienaber, C.A and Eagle, K.A. (2003). Aortic dissection: new frontiers in diagnosis and management: part II: therapeutic management and follow-up. Circulation 108,772-778
Outcomes of Medical Managementof Acute Type B Aortic Dissection Conclusions—Medical management for acutetype B aortic dissection is associated withacceptable outcomes. Outcomes of other management strategiessuch as endovascular stenting for acute typeB aortic dissection need to be compared withopen repair and medical management.Estrera, A. L., Miller, C., Safi, H. J., Goodrick, J. S., Keyhani, A., Porat, E. E., & et al. (2006). Outcomes ofMedical Management of Acute Type B Aortic Dissection. Circulation, 114, I-384–I-389.
Long Term Management Three main management issues in patients whohave survived the initial dissection: medical therapyto minimize aortic wall shear stress; serial imagingto detect signs of dissection progression, redissection, or aneurysm formation and reoperationwhen indicated. Medical therapy — All patients should receive lifelong therapy with an oral beta blocker to reducesystemic blood pressure and the rate of rise insystolic pressure, both of which will minimize aorticwall stress. A target systolic blood pressure of lessthan 120 mmHg. Combination antihypertensivedrug therapy is usually required. Avoidance of strenuous physical activity is alsorecommended as another method to minimizeaortic shear stress.
Long Term Management Serial imaging — A baseline thoracic MRI or chestCT scan prior to discharge with follow-upexaminations at 3, 6, and 12 months, even if thepatient remains asymptomatic. Subsequentscreening studies are then performed every one totwo years if there is no evidence of progression. Reoperation — Repeat surgery is required in 12 to30 percent of patients, usually because ofextension or recurrence of dissection at theprevious site of intervention, localized aneurysmformation remote from the site of repair, graftdehiscence or infection, or aortic regurgitation.
QuestionsandComments
ReferencesBarkley, T. W. & Myers, C.M. (2008). Practice guidelines foracute care nurse practitioners (2nd ed.). St. Louis:Saunders ElsevierCooper, D., & Kranik, A. (Eds.). (2007). The Washingtonmanual of medical therapeutics. Philadelphia: Lippincott,Williams & Wilkins.Estrera, A. L., Miller, C., Safi, H. J., Goodrick, J. S., Keyhani,A., Porat, E. E., & et al. (2006). Outcomes of MedicalManagement of Acute Type B Aortic Dissection.Circulation, 114, I-384–I-389.Hellenic Journal of Cardiology. (2010) Acute Type-B AorticDissection: The Treatment Strategy. Retrieved February8, 2015 fromhttp://www.hellenicjcardiol.com/archive/full text/2010/4/2010 4 338.pdfKasper, D.L, Braunwald, E., Fauci, A. S., Kasper, D. L.,Fauci, A.S., Hauser, S., Longo, D., & Jameson, J. (Eds.).(2008). Harrison's principles of internal medicine. NewYork: McGraw-Hill.
ReferencesNienaber, C.A and Eagle, K.A. (2003). Aortic dissection: newfrontiers in diagnosis and management: part II:therapeutic management and follow-up. Circulation 108,772-778Ramanath, V. S., Oh, J. E., Sundt III, T. M., & Eagle, K. A.(2009). Acute Aortic Syndromes and Thoracic AorticAneurysm. Mayo Clinic Proceedings, 84, (5), 465-481.
Aortic Dissection Epidemiology In the United States, aortic dissection is an uncommon disease. The inc