Transcription
2016Oregon Rural And Frontier Health FacilityLISTENINGTOURIMPROVING THE QUALITY, AVAILABILIT Y AND ACCESSIBILIT Y OF HEALTH CARE FOR RURAL OREGONIANS
The Oregon Office of Rural Health (ORH) coordinates an annualListening Tour of rural and frontier health facilities to discuss andshare current challenges, and to encourage partner collaborationto address solutions. This report is an overview of the commonissues heard during the 2016 Listening Tour.More detail, including current partner activities to address these challenges,is available on the ORH website at: www.ohsu.edu/orh.The 2016 Rural and Frontier Listening Tour report was made possible with funding from the OregonRural Health Association and support by the Health Resources and Services Administration (HRSA)of the U.S. Department of Health and Human Services (HHS) under the Medicare Rural HospitalFlexibility and State Offices of Rural Health Grant Programs.
If you have any questions orsuggestions, please contact:REBECCA DOBERT, Field Services Program Coordinatordobert@ohsu.edu 503.494.6627MEREDITH GUARDINO, Director of Field Servicesguardino@ohsu.edu 503.494.8961CONTENT SACKNOW L E D GE M E NT S4Facility Participants. 4Partner Participants. 5INTR O D U C T I O N6EMERSON ONG, Data and GIS Analystonge@ohsu.edu 503.494.5226What Is Rural and Frontier?. 8STACIE ROTHWELL, Program Managerrothwels@ohsu.edu 971.235.3978WOR KFO R C E10Overview of Challenges. 11Availability and Affordability of Housing. 12The Nursing Challenge. 13Credentialed Medical Assistants. 14Health Information Technology. 15ACC E SS16Overview of Challenges. 17Primary Care Providers. 18Specialists. 22Long-Term Care. 31
AcknowledgementsAdventist Health Tillamook Medical Group,Bay Ocean, Manzanita and TillamookApplegate Valley Family Medicine, Grants PassBlue Mountain Hospital, John DayThank YouFacilityParticipantsBETWEEN AUGUST 22 ANDNOVEMBER 7, 2016, 45 FACILITIESPARTICIPATED IN THE LISTENING TOUR.THEY INCLUDED:14 Critical Access Hospitals (CAHs)2 Type C (50 beds) Rural Hospitals23 Rural Health Clinics (RHCs)Clackamas County Community Health Centers,Oregon CityCoast Community Health Center, BandonColumbia River Community Health Services, BoardmanLower Umpqua Hospital, ReedsportMalheur Memorial Health Clinic, NyssaMercy Medical Center, RoseburgNorth Bend Medical Centers, Coos Bay,Bandon, Gold BeachOHSU Family Medicine, ScappooseOrchid Health Clinic, OakridgeCoquille Valley Hospital, CoquillePeaceHealth Cottage Grove Community Medical Center,Cottage GroveCurry Family Medical, Port OrfordPeaceHealth Peace Harbor Medical Center, FlorenceCurry General Hospital, Gold BeachPioneer Memorial Hospital and Nursing Facility, HeppnerDunes Family Health Care, ReedsportPioneer Memorial Clinic, HeppnerGifford Medical Center, HermistonReedsport Medical Clinic, ReedsportGood Shepherd Medical Center, HermistonSaint Alphonsus Medical Center, Baker CityGood Shepherd Medical Group, HermistonSalem Health West Valley, DallasHarney District Hospital, BurnsSamaritan Coastal Clinic, Lincoln CityHarney District Hospital Family Care, BurnsSamaritan Medical Clinic, Lincoln CityIone Community Clinic, IoneSamaritan North Lincoln Hospital, Lincoln CityIrrigon Medical Center, IrrigonSouth Gilliam Health Center, CondonLake District Hospital, LakeviewStrawberry Wilderness Community Clinic, John DayLake Health Clinic, LakeviewTillamook Regional Medical Center, TillamookValley Family Health Care- Vale Medical Clinic, Vale1 Rural Clinic4 Federally QualifiedHealth Centers (FQHCs)1 Tribal Clinic4Willamette Valley Medical Center, McMinnvilleYellowhawk Tribal Health Center, Pendleton
CareOregonOregon Center for Nursing (OCN)Mindy StadtlanderJana BittonDirector of Network andClinical SupportThank YouParticipatingPartnersFacility participants were askedto choose which partners andrepresentatives they would like theOregon Office of Rural Health to bringto their visit. Thank you to the36 partners who participated inthis year’s Listening Tour.Columbia Pacific CoordinatedCare OrganizationMimi HayleyExecutive DirectorExecutive DirectorBarb Van SlykeOregon Health Authority (OHA)Licensing ManagerNetia MilesDIRECTOR’S OFFICETribal LiaisonEXTERNAL RELATIONSJeston BlackDirector of Legislative andGovernment AffairsKevin CampbellOFFICE OF HEALTHINFORMATION TECHNOLOGYCEOPaul McGinnisDirector of IntegrationKristin BorkLead Policy AnalystMarta MakarushkaSusan MontgomeryLead Policy AnalystTroy SoenenDirectorProvider Relations CoordinatorDirector of CommunityHealth DevelopmentSusan OtterOFFICE OF HEALTH POLICYAND ANALYTICSNorth Bend City/Coos-CurryHousing AuthorityJackie FabrickMarka TurnerMarc OverbeckExecutive DirectorOregon Association of Hospitalsand Health Systems (OAHHS)Andrea EastonBehavioral Health Policy AnalystDirector of the Primary Care OfficeJeffrey ScrogginPolicy AnalystPROVIDER SERVICESAssociate Vice Presidentof Government Affairsand AdvocacyJoell ArchibaldKatie HarrisTRANSFORMATION CENTERDirector of Program ManagementAndy Van PeltExecutive Vice PresidentNicole KrishnaswamiOperations and Policy AnalystJill BoydPrimary CareTransformation SpecialistKathleen HaleyExecutive DirectorBoard MemberKarol DixonEastern Oregon CoordinatedCare Organization/GreaterOregon Behavioral Health, Inc.(EOCCO/GOBHI)Oregon Medical Board (OMB)Innovator AgentSummer BoslaughTransformation AnalystOregon RepresentativesDavid GombergDistrict 10Dallas HeardDistrict 2Oregon Rural Practice-BasedNetwork (ORPRN)Angela CombePractice Enhancement ResearchCoordinatorAnn RomerComprehensive Primary Care InitiativePractice Enhancement ResearchCoordinatorBeth SommersPractice Enhancement ResearchCoordinatorOregon Senators and StaffSenator Betsy JohnsonDistrict 16Senator Arnie RoblanDistrict 5Rosie ShatkinPolicy Advisor for Senator Arnie RoblanAdam WalshSenator Arnie Roblan’s OfficeTrillium CoordinatedCare OrganizationJim ConnollyVice President ofNetwork Development5
INTRODUCTION36% of Oregon’s population livesin rural and frontier communities.
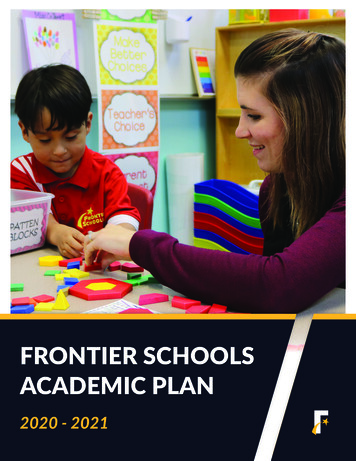
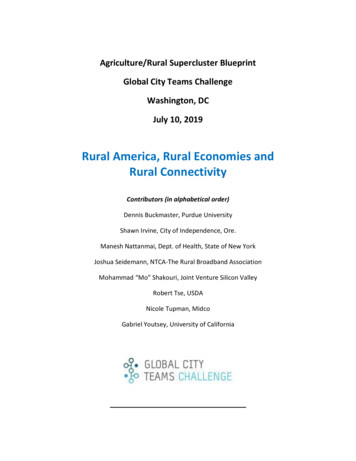
SA F E T Y N E T FACI LI T I ES I N R UR AL AND F R ON TIER ORE G ONLEG E ND7
IntroductionWhat Is Ruraland Frontier?The Oregon Office of Rural Health (ORH)defines rural as any geographic areas in Oregonten or more miles from the centroid of apopulation center of 40,000 people or more.Frontier counties are defined as those withsix or fewer people per square mile. ORH hasidentified 10 of Oregon’s 36 counties as frontier.The Oregon Office of Rural Health analyzesdata at the zip code level in order to identifythe unique characteristics of communities.To do this, ORH breaks Oregon into 130 PrimaryCare Service Areas, 86 of which are rural and18 are frontier. These areas are updatedannually according to changes in populationand health utilization.For more information on definitionsof rural and frontier, and a map of theprimary care service areas, visit ourwebsite at: www.ohsu.edu/orh.8Frontier Is Not theSame as RuralBorders Are a ChallengeBeing a frontier facility requires thinkingdifferently about service and staffing models.Distances to specialty care and higher leveltrauma hospitals are greater. For example,a patient at South Gilliam Health Center inCondon is carried by ambulance 70 milesone-way to the nearest hospital. Whendischarged, the patient must coordinate andfinance transportation for the 70-mile triphome. With distances like these, frontierfacilities must work more independently thantheir urban or rural colleagues. For a frontierfacility, this necessitates recruiting providerswho are skilled and comfortable workingwithout a nearby referral safety net.For facilities near state borders orCoordinated Care Organization (CCO)coverage area boundaries, referrals andcoordinating care can be a challenge.Patient preferences often do not alignwith these borders. For example, a patientmay prefer to seek specialist care in theclosest city rather than travel further inorder to stay within the CCO coveragearea or within Oregon. Many facilitiesare struggling with the lack of specialistreferrals available in their area, the lengthof time for the out-of-network referral tobe approved and length of time followingapproval before specialists can see apatient. Adding to this care coordinationchallenge is the impact of having little orno health information exchange withinOregon and between states.Most frontier facilities do not have a largeenough population to pay for expandedservices (through health tax district funds orpatient volume). Instead they must rely onimpermanent grant or state funds, resultingin an increased need for staff to focus oncare coordination and grant administration.As one hospital CEO stated, “Here a grant,there a grant everywhere a grant, grant.”
“Hospital leadership is not uniquewe need to share resources.”— CEO OF A CRITICAL ACCESS HOSPITALRegional Scale andSolutions Are NeededTo offset the expenses and challengesthat result from being in remote areas,regional partnerships have becomeincreasingly important. Partnershipinitiatives highlighted during the ListeningTour included: Collaboration by Veterans Affairs andsouthern Oregon hospitals to developan accredited allied and mentalhealth college in Roseburg; Partnership between Curry GeneralHospital in Gold Beach and CoastCommunity Health Center in Bandonto improve services in Port Orford; andWasco A successful collaborative grantapplication for regional Lean trainingby Grant, Harney, Lake and MorrowHealth Districts.Suggestions for where regional partnerscould work together to create scaleincluded: leadership and new staff training,administrative support services, datacollection, home and social supportservices, and regulatory compliance.Tumalo FallsKiger Gorge9
WORKFORCERecruiting and retaining a qualified workforcecontinues to be a priority challenge for ruraland frontier health facilities.
Overview ofChallengesProvider Recruitmentand RetentionAdministrationand LeadershipThe most commonly discussed providershortages focused on primary care providers,dentists, behavioral health specialists andancillary staff.While enthusiastic about health reform, facilitiesare concerned about regulatory change andrequirements. Rapidly changing regulationsoften necessitate additional staff work withno additional reimbursement, creating eitheruntenable workloads for current staff or the needto hire staff not budgeted for. As one hospitalCEO noted, “Rural hospitals are held to the samestandards, but with fewer resources.”Facilities differed on preferences for newgraduates versus experienced providers.While some prefer experienced providers,others prefer to hire new graduates who areknowledgeable about technology and readyto build a practice.The most commonly discussed concerns aboutprovider recruitment and retention included: Funding recruitment incentives Loan repayment and forgivenessprogram restrictions Regional competition Residencies and rotations to getstudents into the communities Finding the right fit for thecommunity- not just the job Housing availability and affordability Process delays for licensing Process delays for provider andpayor credentialingAs a result of high senior leadership turnoverduring the past year, especially for CEOs atCritical Access Hospitals, facilities requestedthat a leadership workforce pool and careerdevelopment opportunities be developed.John Day“I need a nurse,not a report.”— CLINIC ADMINISTRATORFor detail on ORH and partner programsto address these challenges, includingthe Oregon Health Authority’s CommonCredentialing and Provider Incentiveprograms, please visit the ORH websiteat www.ohsu.edu/orh.11
“I personally have been acting as a realtor.”WORKFORCE:Availability andAffordability of Housing— A CHIEF NURSING OFFICER ON RECRUITING PROVIDERSPopulationBurns7,152John ed housingunits/percentage3,869 / 82%3,090 / 81%3,120 / 76%6,902 / 64%Vacant housingunits/percentage865 / 18%732 / 19%981 / 24%3,930 / 36%Owner-occupiedunits/percentage2,793 / 72%2,094 / 68%2,295 / 74%4,607 / 67%Rental-occupiedunits/percentage1,076 / 28%996 / 32%825 / 26%2,295 / 33%9418186592,113 646 566 597 737Nielsen Claritas 2016Population Facts by ZIP Code.A lack of affordable housing impacts a facility’s ability torecruit and retain providers and ancillary staff as well asits ability to coordinate care for patients whose housingdifficulties can impact their access to healthcare oradherence to care plans.Support from Coordinated Care Organizations9 provide short-term rental assistance8 provide services to keep individuals in permanent housing5 provide rental advocacy with property owners,including lease negotiations— OHA REPORT ON OREGON CCO HOUSING SUPPORTS: SEPTEMBER, 2016HOUSING OCCUPANCYTotal housing unitsGROSS RENTOccupied unitspaying rentMedian (dollars)AIRBNB (www.airbnb.com) RENTALS AS OF JANUARY 17, 2017Active rentalsFacilities located in high tourism communities, primarily alongthe Oregon coast, were concerned that lucrative vacation rentalsthrough companies like VRBO and Airbnb are driving up rentalprices and decreasing the amount of long-term rentals as well ashomes for sale.Facilities in communities such as John Day and Burns experiencepopulation increases due to seasonal workers (e.g., firefightersand farm workers), which impacts the availability of rentals in thespring and summer.To illustrate these challenges for four service areas, the tableshows census housing unit data* as well as snapshot views ofhomes for sale on Zillow and available rentals on VRBO and Airbnb.12Bandon7,574Rentals that are anentire home393162528112236645VRBO (www.vrbo.com) RENTALS AS OF JANUARY 17, 2017Active rentals(all full homes)1100HOMES FOR SALE ON ZILLOW (www.zillow.com) AS OF JANUARY 16, 2017Information is from a search of Zillow for 2 to 4 bedrooms/ 1 bathroom houses for sale.Any properties with 5 bedrooms or 10 acres of land were removed from the results.Number for sale78411756Lowest price 89,000 35,000 56,500 62,400Highest price 2,750,000 260,000 499,000 2,000,000Median 399,000 99,000 105,000 395,000* Census data was obtained from the 2010-2014 American Community Survey for each ZIP Code thatmakes up the service areas. A housing unit is defined as: a house, an apartment, a group of rooms,or a single room occupied or intended for occupancy as separate living quarters. Separate livingquarters are those in which the occupants do not live and eat with other persons in the structureand which have direct access from the outside of the building or through a common hall.
WORKFORCE:The Nursing ChallengeOregon is projected to have a shortage of nursesstatewide by 2025. Rural and frontier areas are alreadyexperiencing shortages and are facing challenges withrecruiting and retaining nurses at all levels.Developing a “Home-Grown”Nursing Workforce: Insufficient nursing faculty and education programs in rural andfrontier Oregon limit the number of nurses available in these areas. Insufficient rural and frontier clinical training sites, especially foracute shortage specialties like obstetrics or ambulatory care,make finding nurses difficult.Recruiting a Nursing Workforce: Sites reported that a licensure compact in Oregon would allowrural and frontier sites to better compete for out-of-state nurses.Facilities described the time it takes to obtain an Oregon nurselicense as unpredictable, ranging from two weeks to three months. Working as a nurse in a rural or frontier area requires an ability towork independently and to the full scope of their license.For more information on the nursing workforce in Oregon, includinginformation on Oregon’s nurse faculty challenges, visit the OregonCenter for Nursing’s website at: www.oregoncenterfornursing.organd the Oregon State Board of Nursing at: www.oregon.gov/OSBN.CERTIFIED NURSINGASSISTANTS (CNAs)REGISTEREDNURSES (RNs)NURSE PRACTITIONERS(NPs)Practicing in Oregon(2014): 16,233Practicing in Oregon(2014): 38,832Practicing in Oregon(2014): 2,404Licensed in Oregon(2014): 18,414Licensed in Oregon(2014): 47,456Licensed in Oregon(2014): 2,794Level 2 approved trainingprograms in Oregon(2015): 19Median hourly wage(2016): 39.51Approved trainingprograms in Oregon(2015): 2Graduates: NAMedian hourly wage(2016): 14.42Median annual salary(2016): 82,181Median annual salary(2016): 29,987ASSOCIATE DEGREEAvailable seats atapproved schools(2014-2015): 778LICENSED PRACTICALNURSES (LPNs)Total number ofapplicants (2014-2015):2,738Practicing in Oregon(2014): 3,737Total number of newgraduates (2014-2015):613Licensed in Oregon(2014): 4,660Approved trainingprograms in Oregon(2015): 15Graduates (2015): 411Median hourly wage(2016): 23.32Median annual salary(2016): 48,515Graduates: NAMedian hourly wage(2016): 53.17Median annual salary(2016): 110,603BACCALAUREATEDEGREEAvailable seats atapproved schools (20142015): 832Total number ofapplicants (2014-2015):4,293Total number of newgraduates (2014-2015):747SOURCES:Supply Statistics: Oregon Health Authority “Oregon Health Professions: Occupational andCounty Profiles” found at aduate rates: Oregon State Board of Nursing: www.oregon.gov/OSBN/Pages/educational programs.aspx and www.oregon.gov/OSBN/pdfs/passrates.pdf.Average salaries: State of Oregon Employment Department: https://www.qualityinfo.org13
WORKFORCE:CredentialedMedical AssistantsMany facilities noted a need for ancillary medical staff; specifically, for Credentialed Medical Assistants (CMAs) a critical component of facility staffing and team-based care models. The shortage of CMAs is illustrative of theneed for access to education and financial support for all levels of healthcare staff in rural and frontier areas.What IsMeaningful Use?The Role of CredentialedMedical AssistantsCredentialing MedicalAssistantsMeaningful Use (MU) is a federalprogram that provides financial incentiveto Eligible Providers (EPs) and facilitiesfor the transition to, and use of electronichealth records (EHRs). Meaningful Usepayments can be an important source offinancial support. During the first year,facilities that implemented a certifiedEHR received 21,250 for each of theirMedicaid EHR Incentive EPs. Years twothrough five, facilities receive 8,500 perEP that achieves MU.One MU requirement is computerizedphysician order entry (CPOE), enteringclinician instructions electronically in orderto reduce errors. In practice settings,Medical Assistants (MA) may completethese tasks under the supervision of anEP, allowing the EP to spend more timeproviding direct patient care. The use ofnon-credentialed MAs to complete CPOEcan put EPs and facilities at risk of notreceiving significant MU dollars.Facilities noted that there is interest fromcommunity members to become CMAs. However,tuition costs and the distance to attend educationprograms often contribute to the limitations of a“home-grown” solution.Employment opportunity for MAs in Oregon isexpected to grow by 24.6%, with 441 total jobopenings yearly, from 2014 to 2024.*A Medical Assistant can be credentialed by:1. Graduating from an accredited MA program.This qualifies students to take an exam tobecome credentialed by the accrediting bodyaffiliated with their program.14There is no single, standard accrediting body forcertified MA education programs. Tuition costsfor these programs ranged from approximately 4,400 to 15,000 in 2016.2. Previously licensed and workingbut non-credentialed MAsmay take some accreditingorganizations’ credentialing examsif they meet requirements. Examsneed to be taken at a test centerthat provides proctoring, most ofwhich are in urban areas. In 2014, 26 Oregon MA programs graduated1,206 students. 15 of those programs were in urban/metro areas. Only 2 programs were west of The Dalles,in Ontario and Pendleton.To help reduce the travel costs forMAs wishing to take credentialingexams, facilities such as HarneyDistrict Hospital and WindingWaters Clinic have found accreditingorganizations that certify facility staffas proctors and enable facilities tobecome approved testing sites.* For more detail on Oregon MA programs visit the State of Oregon Employment Department atwww.qualityinfo.org and the ORH website at www.ohsu.edu/orh.
WORKFORCE:Health InformationTechnology“One of the first questions I get asked by potentialrecruits is “what EHR do you use?””— HOSPITAL DIRECTOR OF HUMAN RESOURCESA fundamental Health Information Technology(HIT) challenge in rural and frontier Oregonis a lack of broadband availability and limitedinternet access. Examples of challenges forfacilities included: limiting simultaneous internetusers to ensure there is enough bandwidthfor critical functions, frequently losinginternet access due to seasonal weather, aninability to provide direct-to-home telehealthservices or for patients to access their recordselectronically because of little or no internetaccess in outlying communities.Facilities raised multiple HIT concerns impactingproviders and care coordination. They included: The need and cost to increase IT staff tomanage HIT components of work and keeppace with an evolving HIT environment; Limitations of Electronic Health Recordsand frustrations with prohibitive costs toupgrade or improve functionality; The lack of system interoperabilitybetween facilities and referral networks,including behavioral health and HomeHealth Agencies; The need for improved electronic healthinformation exchange (including acrossstate borders) for care coordination.Oregon Health Authority Information Technology to Support Providers:The Oregon Prescription Drug Monitoring Program (PDMP) to support theappropriate use of prescription drugs. Pharmacies submit prescription data to the PDMPsystem for all Schedule II, III and IV controlled substances dispensed to Oregon residents.The Emergency Department Information Exchange (EDIE) to enable emergencydepartment clinicians to identify patients who visit the emergency room more than five timesin a 12 month period or patients with complex care needs. EDIE alerts hospitals in real timethrough the EHR or fax, enabling instant viewing of patient information.PreManage to leverage the EDIE data and send hospital utilization information, as well ascare guidelines to pre-defined health plans, CCOs, and provider groups (including behavioralhealth and long-term care) on a real-time basis for specified member or patient populations.The Oregon Common Credentialing Program (OCCP) (expected in 2018)to minimize health care practitioner burdens and credentialing organization redundancies.Under the OCCP, providers must submit their credentialing information to a web-based systemwhich all credentialing organizations will be required to use, rather than each organizationcollecting and verifying it separately.Oregon’s Provider Directory (expected in 2018) to serve as an accurate source ofhealthcare practitioner and practice information needed for operations, analytics and healthinformation exchange.“I feel like our EHR vendor has a gag order on me.”— A HOSPITAL CFO ON THE NEED FOR STATE OVERSIGHT OF EHR VENDORSTO CONTROL COSTS AND QUALITY OF SERVICES PROVIDED“We’re doing a lot of faxing ”— A CLINIC PROVIDER ON THEIR INTERNET CONNECTIVITY15
ACCESSAccess to primary care providers, specialistsand acute care placement options remains achallenge that contributes to changing servicedelivery models.
Overview ofChallenges“We are in the messy middle between volume and value.”— CEO OF A CRITICAL ACCESS HOSPITALSpecialists and PrimaryCare ProvidersLack of Acute CarePlacementsIt is not feasible for many remote,low volume hospitals to hire full-timespecialists. Rural and frontier facilitiesoften depend on primary care providersfor an expanded scope of services. Manyfacilities discussed efforts to educatetheir patients and communities aboutthe services primary care providers canprovide locally, to try and deter patientsfrom traveling far distances to seespecialists (e.g. pediatricians).A consistently discussed challenge for facilitieswas the lack of acute care availability in theirareas. This included:However, many facilities continue to havedifficulty recruiting and retaining primarycare providers. At the time of the listeningtour visit, one hospital had recentlypublished a letter to the communityapologizing for the high turnover inprimary care providers and explainingthe changes they were making to improverecruitment efforts.Other avenues to provide specialistaccess include telehealth programmingand traveling or contracted specialists.The lack of telehealth reimbursement,available specialists and slow Medicaidpre-authorizations were commonlyidentified barriers. Acute mental health care bedsMany hospitals continue to reportsignificant difficulty finding inpatienttreatment for mental health patients,necessitating lengthy stays in emergencydepartment hold rooms. Substance abuse treatmentMany facilities referenced the lack ofcoordination between mental health andaddiction services in their county and thegrowing need for addiction and substanceabuse resources- including specializedmental health providers, treatmentfacilities and medical interventions suchas Suboxone. Long-term careFacilities reported that the lack of HomeHealth Agencies and residential long-termcare facilities makes it difficult for patientsto find care close to home. Two facilitieshighlighted that Traumatic Brain Injury andaging dementia patients continue to bebrought to hospital hold rooms due to alack of memory care unit beds.New Models of CareMany of the independent and smallerhospitals discussed recent transitions intheir service models, partly as a resultof access challenges. Specifically, theyare shifting towards outpatient andurgent care, with concerns about how touse shrinking revenue to build strongerambulatory programs.In 2017, the Oregon HealthAuthority plans to release:1.Recommendations from theBehavioral Health Collaborative onbuilding a 21st Century BehavioralHealth System.2. A report, with recommendations,to the Oregon legislature regardingthe problem of boarding patientswith mental illness in hospitalemergency departments.3. A behavioral health mapping tool.These will be accessible on theORH website once they aremade available.17
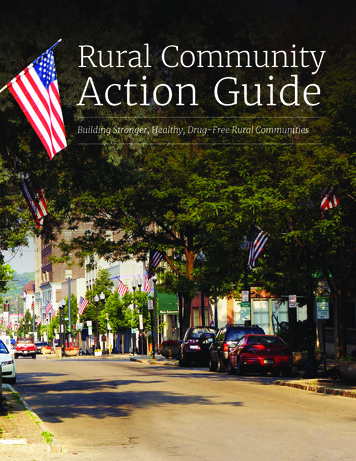
ACCESS:The primary care and specialist maps includephysicians and physician assistants (PAs). In ruraland frontier Oregon PAs often manage full patientcaseloads under their supervising physician.Additionally, specialists from larger epicenters oftentravel to small communities to see patients. Manyspecialists have integrated PAs into these rotations.Primary Care ProvidersPrimary Care Physicians andPhysician Assistants FTE byService Area, 2015The percentage of rural Oregonians with insurancecoverage has increased since the introduction of theAffordable Care Act as has the number of physicianspracticing in Oregon. While not reaching optimum percapita levels, the increase of physicians in rural andfrontier Oregon is encouraging.Key Statistics20132015 % ChangeOREGONPrimary Care mary Care Physicians1,619.9Population2,480,504RURALPrimary Care PhysiciansPopulationFRONTIERPrimary Care PhysiciansPopulation18
LEGENDSOURCE: Oregon Medical Board, 201519
ACCESS:Primary Care ProvidersNumber of ActiveNurse Practitioners byService Area, 2016LEGEND20SOURCE: Oregon State Board of Nursing, 2016
ACCESS:Primary Care ProvidersNumber of ActiveDentists byService Area, 2016LEGENDSOURCE: Oregon Board of Dentistry, 201621
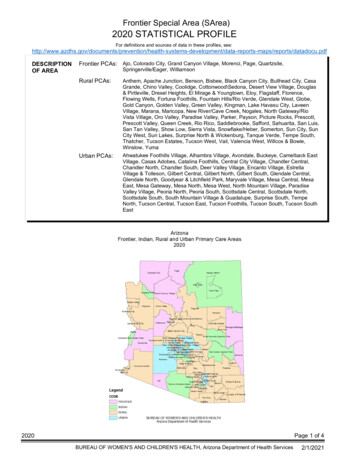
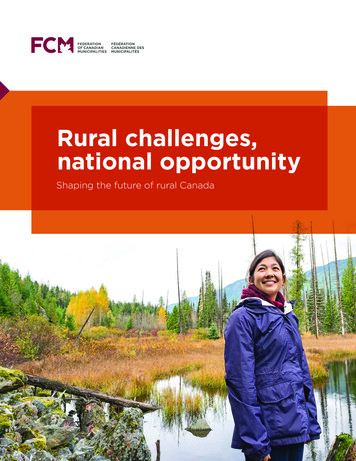
ACCESS:SpecialistsOncologists FTE byService Area, 2015 andCancer Death Rates,2010-2014 Average Per YearCancer is the leading cause ofdeath in Oregon with highermortality rates in rural andfrontier Oregon compared tourban areas.KeyStatisticsTotalDeathsPer100,000 CancerPeople DeathsOregon820.9 243.4Urban708.1 203.9RuralFrontier1,020.9316.51,051.1 296.6LEGEND22SOURCE: Oregon Medical Board, 2015
ACCESS:SpecialistsCardiologists FTE by ServiceArea, 2015 and HeartDisease Death Rates, 20102014 Average Per YearHeart disease is the secondleading cause of death in Oregonwith higher mortality ratesin rural and frontier Oregoncompared to urban areas.KeyStatisticsTotalDeathsPerHeart100,000 DiseasePeople ,051.1225.2RuralFrontierLEGENDSOURCE: Oregon Medical Board, 201523
ACCESS:SpecialistsCardiovascular SpecialistsFTE by Service Area, 2015and Heart Disease DeathRates, 2010-2014 AveragePer YearLEGEND24SOURCE: Oregon Medical Board, 2015
ACCESS:SpecialistsPulmonary Specialists FTE byService Area, 2015 and ChronicLower Respiratory Death Rates,2010-2014 Average Per YearChronic Lower Respiratory Disease(Chronic Obstructive PulmonaryDisease) is the third leading cause ofdeath in Oregon, with the mortalityrate in frontier Oregon almostdouble the rate of urban areas. Withthe exception of Bend and Ontario,there are no pulmonary specialistsin central or eastern ENDSOURCE: Oregon Medical Board, 201525
ACCESS:SpecialistsGeriatric Specialists FTEby Service Area, 2015 andAlzheimer’s Death Rates,2010-2014 Average Per YearA recent telehealth pilot project, funded by the Oregon State Innovation Model funds,may offer assistance to rural and frontier Alzheimer’s patients and their caregivers:The Layton Center at Oregon Health & Science
health college in Roseburg; Partnership between Curry General Hospital in Gold Beach and Coast Community Health Center in Bandon to improve services in Port Orford; and A successful collaborative grant application for regional Lean training by Grant, Harney, Lake and Morrow Health Districts. Suggestions for where regional partners