Transcription
CHAPTERSuccess is the plateau that one rests upon totake a breath and look down from upon thestraight and difficult path, but one does notclimb upon a plateau.—Josephine Preston Peabody29Nursing ManagementObstructive Pulmonary DiseasesJane Steinman Kaufmanttp:h // evolve. elsevier. com / Lewis/ medsurg Answer Guidelines for Case Study on p.Concept Map for Case Study on p.Audio Lecture: AsthmaeTables eTable 29-1: Asthma Action Plan (Spanish)eFigure eFig. 29-1: Postural drainage positionsInteractive Case Studies Patient with Asthma Patient with Chronic ObstructivePulmonary Disease Patient with Cystic FibrosisCustomizable Nursing Care Plan Patient with Asthma Patient with Chronic ObstructivePulmonary Disease Patient and Caregiver Teaching Guides inEnglish and Spanish Home Oxygen Use How to Use a Dry Powder Inhaler (DPI) How to Use a Peak Flow MeterContent UpdatesKey Points (Printable and CD/MP3 Download)Concept Map CreatorNCLEX Examination Review QuestionComprehensive Audio Glossary and KeyTerm Flash CardsElectronic CalculatorsClinical Reference: Laboratory ValuesWebLinks Stress-Busting Kit for Nursing StudentsNCLEX Examination Review QuestionsComprehensive Audio GlossaryLEARNING OUTCOMES1. Describe the etiology, pathophysiology, clinical manifestations,and collaborative care of asthma.2. Describe the nursing management of the patient with asthma.3. Differentiate among the etiology, pathophysiology, clinicalmanifestations, and collaborative care of the patient with chronicobstructive pulmonary disease (COPD).4. Describe the effects of cigarette smoking on the lungs.5. Identify the indications for O2 therapy, methods of delivery,and complications of O2 administration.6. Explain the nursing management of the patient with COPD.7. Describe the pathophysiology, clinical manifestations, collaborativecare, and nursing management of the patient with cystic fibrosis.8. Describe the pathophysiology, clinical manifestations, collaborativecare, and nursing management of the patient with bronchiectasis.KEY TERMSα1-antitrypsin deficiency, p. 611asthma, p. 588bronchiectasis, p. 635chest physiotherapy, p. 623chronic bronchitis, p. 610chronic obstructive pulmonary disease(COPD), p. 610cor pulmonale, p. 613cystic fibrosis, p. 631emphysema, p. 610Imagine needing to consciously think about every breath thatyou take for minutes, hours, or days. Many individuals withobstructive lung disease have this experience. Approximately30 million adult Americans are living with chronic obstructivepulmonary disease (COPD) or asthma.1 Obstructive pulmonary disease, the most common chronic lung disease, includesdiseases characterized by increased resistance to airflow as aO2 toxicity, p. 621postural drainage, p. 624pursed-lip breathing, p. 623result of airway obstruction or airway narrowing. Types ofobstructive lung diseases are asthma, COPD, cystic fibrosis,and bronchiectasis. Asthma is a c hronic inflammatory lungdisease that results in variable episodes of airflow obstruction,but it is usually reversible. COPD is an obstructive pulmonarydisease with progressive limitation in airflow that is not fullyreversible.2-4Reviewed by Margaret Clifton, RN-BC, MS, CLNC, Department Chair, Nursing and Fire Science, Community College of Rhode Island, Warwick,R.I.; Julie Miller, RN, BSN, CCRN, Staff Development Educator—Critical Care, Trinity Mother Frances Hospital, Tyler, Tex.; Susan A. Sandstrom,MSN, RNC, CNE, A ssociate Professor of Nursing, College of Saint Mary, Omaha, N eb.; and Merita Konstantacos, RN, MS N, CCNS, StaffRN—CVSICU/CVSSD, Aultman Hospital, Canton, Ohio.587
588SECTION 5Problems of Oxygenation: VentilationThe patient with asthma has variations in airflow over time,usually with normal lung function between exacerbations,whereas the limitation in expiratory airflow in the patient withCOPD is generally more constant. The pathology of asthma andresponse to therapy differ from COPD. However, the patientwith a diagnosis o f obstructive pulmonary disease may havefeatures of both asthma and COPD. Patients with asthma whohave less responsive reversible airflow obstruction are difficultto distinguish from COPD patients.2Cystic fibrosis, another form of obstructive pulmonary disease, is a g enetic disorder that produces airway obstructionbecause of changes in exocrine glandular secretions, resultingin increased mucus production. Bronchiectasis is an obstructivedisease characterized by dilated bronchioles most f requentlyresulting from untreated or poorly treated pulmonary infections that cause an increase in sputum production.ASTHMAAsthma is a chronic inflammatory disorder of the airways. Thechronic inflammation leads to recurrent episodes of wheezing,breathlessness, chest tightness, and cough, particularly at nightor in the early morning. These episodes are associated with widespread but variable airflow obstruction that is usually reversible,either spontaneously or with treatment. The clinical course ofasthma is unpredictable, ranging from periods of adequate control to exacerbations with poor control of symptoms.4Asthma affects an estimated 16 millio n adult Americans.Among adults, women are 66% mo re likely to have asthmathan men. Asthma is a public health concern with over 10 million lost w orkdays in ad ults.5 The significant morbidity ratesrelated to asthma may be attributed to limited access to healthcare, an inaccurate assessment of disease severity, a dela y inseeking help, inadequate medical tr eatment, nonadherence toprescribed therapy because of the high cost, and an increase inallergens in the environment, especially in the inner city. Olderadults may be underdiagnosed with asthma primarily becausetheir symptoms are similar to those of COPD and pulmonaryfunction testing is not commonly done in this age-group.5After a long period of a steady increase in rates, it appears thatmortality and morbidity rates from asthma have reached a plateau and/or decreased. However, in people older than 15 yearsof age, annually there are over 3700 deaths with more than 50%in people older than 65 y ears of age. (Gender and cultural/ethnic differences are presented in boxes below.)Risk Factors for Asthma and Triggers of Asthma AttacksRisk factors for asthma and triggers of asthma attacks can berelated to the patient (e.g., genetic factors) or the environmentGENDER DIFFERENCESAsthmaMENWOMEN Before puberty,boys are moreaffected than girls. After puberty and into adulthood, morewomen are affected than men. Women who are admitted to the emergency department are more likely to needhospitalization. Death rate from asthma is greater inwomen than men.CULTURAL AND ETHNIC HEALTHDISPARITIESObstructive Pulmonary Diseases Asthma prevalence rates are over 38% higher among African Americans than whites. Puerto Ricans have higher asthma prevalence rates and age-adjusteddeath rates than all other racial and ethnic subgroups. Female African Americans have the highest mortality rates fromasthma among all ethnic/gender groups. Whites have the highest incidence of chronic obstructive pulmonarydisease despite high rates of smoking among other ethnic groups. Whites have the highest incidence of cystic fibrosis. Cystic fibrosis is uncommon among African Americans, Hispanics,and Asian Americans.(Table 29-1). Male gender is a r isk factor for asthma in c hildren (but not adults) for unclear reasons. Obesity has also beenshown to be a risk factor for asthma.3 Other factors and triggersare discussed in this section.Genetics. Asthma has a co mponent that is inher ited, butthe genetics are complex. Numerous genes may be involved inthe development of asthma and different ethnicities may havedifferent genes.3,4 Atopy, the genetic predisposition to developan allergic (immunoglobulin E [I gE]– mediated) response tocommon allergens, is a major risk factor for asthma.Immune Response. The hygiene hypothesis suggests that anewborn baby’s immune system must be educated so it willfunction properly during infancy and the rest of life. If a personis exposed to certain infections early in life, uses few antibiotics,is exposed to other children (e.g., siblings, day care), or lives inthe country or with pets, he or she will have a lower incidence ofasthma. If these factors are not present in one’s childhood, theperson has a higher rate of asthma.4Allergens. Indoor and outdoor allergens are well known totrigger asthma symptoms, but their role in the development ofasthma is unclear. House dust mites are a pervasive problem asTABLE 29-1TRIGGERS OF ACUTE ASTHMAATTACKSAllergen inhalation Animal dander (e.g., cats,mice, guinea pigs) House dust mite Cockroaches Pollens MoldsAir pollutants Exhaust fumes Perfumes Oxidants Sulfur dioxides Cigarette smoke Aerosol spraysViral upper respiratory infectionSinusitisExercise and cold, dry airStressDrugs Aspirin Nonsteroidal antiinflammatory drugs β-Adrenergic blockersOccupational exposure Agriculture, farming Paints, solvents Laundry detergents Metal salts Wood and vegetable dusts Industrial chemicals andplastics Pharmaceutical agentsFood additives Sulfites (bisulfites andmetabisulfites) Beer, wine, dried fruit,shrimp, processed potatoes Monosodium glutamate TartrazineHormones/mensesGastroesophageal reflux disease(GERD)
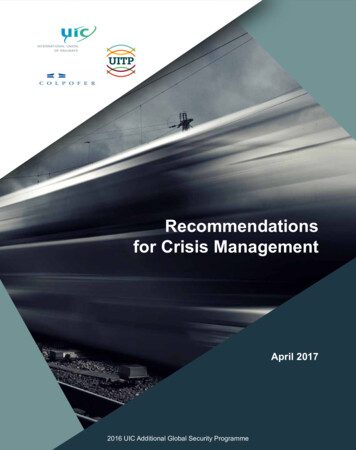
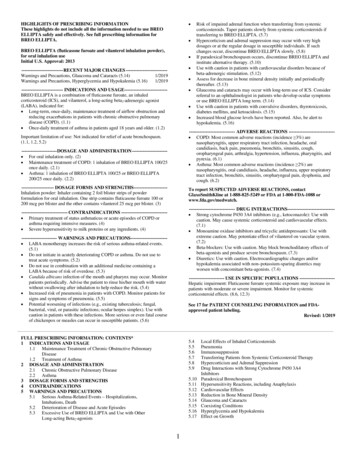
CHAPTER 29they are almost impossible to eliminate. Cockroaches, furry animals, fungi, and molds can trigger asthma attacks, but the rolein the actual development of asthma is not as clear.3,4Exercise. Asthma that is ind uced or exacerbated duringphysical exertion is called exercise-induced asthma (EIA). Typically, EIA occurs after vigorous exercise, not during it (e.g., jogging, aerobics, walking briskly, climbing stairs). Symptoms ofEIA are pronounced during activities where there is exposure tocold, dry air. For example, swimming in an indoor heated poolis less likely to produce symptoms than downhill skiing. Airwayobstruction may occur due to changes in t he airway mucosacaused by the hyperventilation occurring during exercise witheither cooling or rewarming of air and capillary leakage in theairway wall.Air Pollutants. Various air pollutants, cigarette or woodsmoke, vehicle exhaust, elevated ozone levels, sulfur dioxide,and nitrogen dioxide can trigger asthma attacks. In heavilyindustrialized or densely populated areas, climatic conditionsoften lead to concentrated pollution in t he atmosphere, especially with thermal inversions and stagnant air masses. Ozonealert days are regularly noted on the news reports, and patientsshould minimize outdoor activity during these times. Cigarettesmoking is associated with an accelerated decline of lung functioning in a p erson with asthma, increases the severity of thedisease, may cause the patient to be less responsive to treatmentwith corticosteroids (either systemic or inhaled), a nd reducesthe chance of the asthma being controlled.3Occupational Factors. Occupational asthma is the mostcommon occupational respiratory disorder with up to 15% ofnew asthma cases arising from job-related exposures.6 Irritantscause a c hange in t he responsiveness of the airways. Agricultural workers, painters (including spray painting), plastics manufacturing, and cleaning work are occupations with a high risk.Characteristically, patients will give a history of arriving at workfeeling well but experience gradual development of symptomsby the end of the day.Respiratory Infections. Respiratory infections (i.e., viral andnot bacterial) are often the major precipitating factor of an acuteasthma attack. The respiratory syncytial virus (RSV) in childrenand the rhinovirus are two major factors in the development andpossibly the severity of asthma.4 Infections cause an increase inthe hyperresponsiveness of the bronchial system that may lastfrom 2 to 8 weeks after the infection in both normal and asthmatic persons. It is thought that viruses cause asthma exacerbations by activating the immune system. This ultimately resultsin production of inflammatory mediators leading to the onsetof asthma symptoms.Nose and Sinus Problems. Allergic rhinitis is a major predictor of adult asthma.7 Treatment of allergic rhinitis reduces thefrequency of asthma exacerbations. Some patients with asthmahave chronic sinus problems that cause inflammation of themucous membranes. Although the cause is usuall y noninfectious (e.g., allergies), bacterial infections may also be a cause.Sinusitis must be treated and large nasal polyps removed for theasthma patient to have good control. (Sinusitis is discussed inChapter 27.)Drugs and Food Additives. Sensitivity to specific drugs mayoccur in some persons, especially those with nasal polyps andsinusitis. Some people with asthma have what is ter med theasthma triad—nasal polyps, asthma, and sensitivity to aspirinand nonsteroidal antiinflammatory drugs (NSAIDs). Salicylicacid can be found in many over-the-counter (OTC) drugs andObstructive Pulmonary Diseases589some foods, beverages, and flavorings. In some asthmatics whouse aspirin or NSAIDs (e.g., ibuprofen [Motrin]), wheezing willdevelop within 2 hours. In addition, there is usually profoundrhinorrhea, congestion, and tearing. Facial flushing, gastrointestinal symptoms, and angioedema can occur. Although sensitivity to salicylates persists for many years, the nature andseverity of the reaction can change over time. Avoidance ofaspirin and NSAIDs is required. However, patients with aspirinsensitivity under the care of an allergist can be desensitized bydaily administration of the drug.β-Adrenergic blockers in oral form (e.g., metoprolol [Toprol])or topical eyedrops (e.g., timolol [Timoptic]) may trigger asthmabecause of bronchospasm. Angiotensin-converting enzyme(ACE) inhibitors (e.g., lisinopril [Prinivil]) may produce coughin susceptible individuals, thus making asthma symptoms worse.Other agents that may precipitate asthma in the susceptiblepatient are tartrazine (yellow dye no. 5, f ound in ma ny foods)and sulfiting agents widely used in t he food and pharmaceutical industries as p reservatives and sanitizing agents. Sulfitingagents are commonly found in f ruits, beer, and wine and usedextensively in s alad bars to protect vegetables from oxidation.Asthma exacerbations have been reported after the use of sulfitecontaining preservatives found in topical ophthalmic solutions,intravenous (IV) corticosteroids, and some inhaled bronchodilator solutions. Food allergies triggering asthma reactions in adultsare rare. Avoidance diets are not recommended until an allergyhas been demonstrated, usually by oral challenges.3Gastroesophageal Reflux Disease. The exact mechanismby which gastroesophageal reflux disease (GERD) tr iggersasthma is unknown. It is postulated that reflux of stomach acidinto the esophagus can be aspirated into the lungs, causingreflex vagal stim ulation and bronchoconstriction. AlthoughGERD is primarily involved in nocturnal asthma, it can triggerdaytime asthma as well. (GERD is discussed in Chapter 42.)Psychologic Factors. Asthma is no t a psy chosomatic disease. However, emotional stress that is s een with extremes ofemotion such as cr ying, laughing, anger, and fear can lead tohyperventilation and hypocapnia, which can cause airway narrowing.3 An ast hma attack caused by any triggering mechanism can produce panic, stress, and anxiety, which are notunexpected emotions during this experience. Panic is a normalresponse to not being able to breathe. The extent to which psychologic factors contribute to the induction and continuationof any given acute exacerbation is unkno wn, but it probablyvaries from patient to patient and in the same patient from episode to episode.PathophysiologyThe primary pathophysiologic process in ast hma is p ersistent but variable inflammation of the airways. The airflow islimited because the inflammation results in bronchoconstriction, airway hyperresponsiveness (hyperreactivity), and edemaof the airways. Exposure to allergens or irritants initiates theinflammatory cascade (Fig. 29-1). A va riety of inflammatorycells are involved including mast cells, macr ophages, eosinophils, neutrophils, T and B lymphocytes, and epithelial cells ofthe airways.4As the inflammatory process begins, mast cells (f oundbeneath the basement membrane of the bronchial wall) degranulate and release multiple inflammatory mediators (Fig. 29-2 ).IgE antibodies are linked to mast cells and the allergen crosslinks the IgE. Then common inflammatory mediators such as
590SECTION 5Problems of Oxygenation: VentilationPATHOPHYSIOLOGY MAPTriggers Infection Allergens Exercise IrritantsMast cell degranulationImmune activation(IL-4, IgE production)Inflammatory mediatorsVasodilationIncreased capillary permeability BronchospasmVascular congestionEdema formationMucus secretionImpaired mucociliary functionThickening of airway walls Bronchial hyperresponsiveness Airway obstructionFIG. 29-1Cellular infiltration(neutrophils, lymphocytes, eosinophils)Neuropeptides releasedwith autonomicnervous system effectsAirwayremodelingPathophysiology of asthma. IL, Interleukin.leukotrienes, histamine, cytokines (e.g., interleukins-4 and 5),prostaglandins, and nitric oxide are released. Some inflammatorymediators have effects on the blood vessels, causing vasodilationand increasing capillary permeability. Some mediators result inthe airways being infiltrated by eosinophils, lymphocytes, andneutrophils. The resulting inflammatory process results in vascular congestion; edema formation; production of thick, tenaciousmucus; bronchial muscle spasm; thickening of airway walls; andincreased bronchial hyperresponsiveness8 (Fig. 29-3 Th). is wholeprocess is s ometimes referred to as t he early-phase response inasthma. Clinically it can occur within 30 to 60 min utes afterexposure to the allergen or irritant.Symptoms can recur 4 t o 10 ho urs after the initial attackbecause of eosinophil and lymphocyte activation and further release of more inflammatory mediators. The epithelialcells also produce cytokines and other inflammatory mediators. This delayed response is called t he late-phase response inasthma. Only about 30% t o 50% o f patients experience thisdelayed response. It can be more severe than the early-phaseresponse and persist for 24 hours or more. It is characterizedby a s elf-sustaining cycle of inflammation. Airflow may belimited from the swelling of the airways with or without bronchoconstriction. Corticosteroids are effective in tr eating thisinflammation.Alterations in the neural control of the airways also occur inasthma. The autonomic nervous system, consisting of the parasympathetic and sympathetic systems, innervates the bronchi.Airway smooth muscle tone is regulated by the parasympatheticnervous system. In asthma, there is overactivity of the parasympathetic nervous system. When airway nerve endings are stimulated by mechanical or chemical stimuli (e.g., air pollution, coldair, dust, allergens), increased release of acetylcholine resultsin increased smooth muscle contraction and mucus secretion,ultimately leading to bronchoconstriction.Chronic inflammation may result in str uctural changes inthe bronchial wall known as remodeling. A progressive loss oflung function occurs that is not prevented or fully reversed bytherapy. The changes in str ucture may include fibrosis of thesubepithelium, smooth muscle hypertrophy of the airways,mucus hypersecretion, continued inflammation, and angiogenesis (proliferation of new blood vessels). Remodeling is thoughtto explain why some individuals have persistent asthma andlimited response to therapy.3,4Hyperventilation occurs during an asthma attack as l ungreceptors respond to increased lung volume from trappedair and airflow limitation. Decreased perfusion and ventilation of the alveoli and increased alveolar gas p ressure lead toventilation-perfusion abnormalities in t he lungs. The patientwill be hypoxemic early on with decreased PaCO2 and increasedpH (respiratory alkalosis) as he o r she is h yperventilating. Asthe airflow limitation worsens with air trapping, the patientworks much harder to breathe. The PaCO2 will normalize as thepatient tires, and then it will increase to produce respiratory acidosis, which is an ominous sign signifying respiratory failure.8
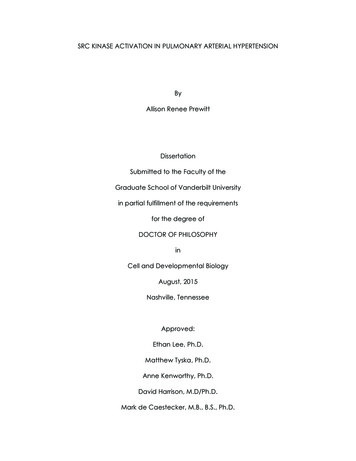
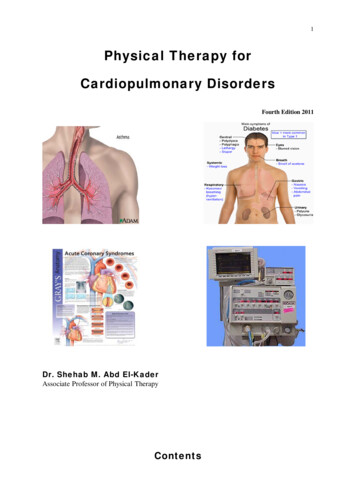
CHAPTER 29B-lymphocyteAllergensMast cellIgE antibodiesPlasma cells591Obstructive Pulmonary DiseasesSmooth muscleSwollen mucosaMusclein spasmMucusAAllergensHistamineMucusInflammatory mediatorsMast cellBMucusFIG. 29-3 Factors causing obstruction (especially expiratory obstruction) in asthma. A, Cross section of a bronchiole occluded by musclespasm, swollen mucosa, and mucus in the lumen. B, Longitudinal section of a bronchiole.FIG. 29-2 Allergic asthma is triggered when an allergen cross-links IgEreceptors on mast cells, which are then activated to release histamineand other inflammatory mediators (early-phase response). A late-phaseresponse may occur due to further inflammation.Clinical ManifestationsAsthma is c haracterized by an unpredictable and variablecourse from seemingly minor interferences in b reathing tolife-threatening episodes that can occur in t he same person.Depending on an individual’s response, asthma can rapidlyprogress from normal breathing to acute severe asthma. Recurrent episodes of wheezing, breathlessness, chest tightness, andcough, particularly at night and in the early morning, are typicalin asthma. An attack of asthma may have an abrupt onset, butusually symptoms occur more gradually. Attacks may last for afew minutes to several hours. Between attacks the patient maybe asymptomatic with normal or near-normal pulmonary function, depending on the severity of disease. However, in s omepersons, compromised pulmonary function may result in a stateof continuous symptoms and chronic debilitation characterizedby irreversible airway disease.The characteristic clinical manifestations of asthma arewheezing, cough, dyspnea, and chest tightness after exposure toa precipitating factor or trigger. Expiration may be prolonged.Instead of a normal inspiratory-expiratory ratio of 1:2, it may beprolonged to 1:3 or 1:4. Normally the bronchioles constrict during expiration. However, as a r esult of bronchospasm, edema,and mucus in t he bronchioles, the airways become narrowerthan usual. Thus it takes longer for the air to move out of thebronchioles. This produces the characteristic wheezing, air trapping, and hyperinflation.Wheezing is a n unreliable sign t o gauge the severity ofan attack. Many patients with minor attacks wheeze loudly,whereas others with severe attacks do not wheeze. The patientwith severe asthmatic attacks may have no a udible wheezingbecause of the marked reduction in a irflow. For wheezing tooccur, the patient must be able to move enough air to producethe sound. Wheezing usually occurs first on exhalation. Asasthma progresses, the patient may wheeze during inspirationand expiration.In some patients with asthma, cough is the only symptom,and this is ter med cough variant asthma. The bronchospasmmay not be severe enough to cause airflow obstruction, but itcan increase bronchial tone and cause irritation with stimulation of the cough receptors. The cough may be nonproductive.Secretions may be thick, tenacious, white, gelatinous mucus,which makes their removal difficult.The person with asthma has difficulty with air movementin and out of the lungs, which creates a feeling of suffocation.Therefore during an acute attack, the person with asthmausually sits upright or slightly bent forward using the accessory muscles of respiration to try to get enough air. The moredifficult the breathing becomes, the more anxious the patientfeels.Examination of the patient during an acute attack usuallyreveals signs of hypoxemia, which may include restlessness,increased anxiety, inappropriate behavior, increased pulseand blood pressure, and pulsus paradoxus (a dr op in syst olicpressure during the inspiratory cycle greater than 10 mm Hg).(Measurement of pulsus paradoxus is presented in Table 37-8.)As the patient worsens, it becomes difficult to speak in complete sentences. The respiratory rate is significantly increased(greater than 30 breaths/min) with the use of accessory muscles. Percussion of the lungs indicates hyperresonance, andauscultation indicates the presence of inspiratory or expiratorywheezing. As the episode resolves, coughing produces thick,stringy mucus.Diminished or absent breath sounds may indicate a significant decrease in air movement resulting from exhaustion and aninability to generate enough muscle force to ventilate. Severelydiminished breath sounds, often referred to as the “silent chest,”are an ominous sign, indicating severe obstruction and impending respiratory failure.
592SECTION 5Problems of Oxygenation: VentilationClassification of AsthmaAsthma can be classified as intermittent, mild persistent, moderate persistent, or severe persistent4 (Table 29-2 ).The classification system is us ed at diagnosis t o determine the initialtreatment. The classification is based on the current impairmentof the person (i.e., symptoms, lung function measurements)and the risk for future exacerbations that require oral corticosteroids. Patients may move to different asthma classificationsover the course of their disease.ComplicationsSevere Acute Asthma and Life-Threatening Asthma. Severeasthma exacerbations occur when the patient is d yspneic atrest and the patient speaks in words, not sentences, because ofthe difficulty breathing. The patient is usuall y sitting forwardto maximize t he diaphragmatic movement with prominentwheezes and a respiratory rate higher than 30 per minute andpulse higher than 120 p er minute. Accessory muscles in t heneck are straining to try to lift the chest wall and the patient isoften agitated. The peak flow (peak expiratory flow rate [PEFR])is 40% of the personal best or less than 150 mL. Arterial bloodgas (ABG) changes are listed in Table 29-3. Neck vein distentionand a p ulsus paradoxus of 40 mm H g or greater may result.Usually it is difficult to auscultate pulsus paradoxus secondaryto a noisy chest or increased work of breathing. These patientsusually are seen in emergency departments (EDs) or hospitalized.3,4TABLE 29-2A few patients perceive asthma symptoms poorly and mayhave a significant decrease in lung function without any changein symptoms. Patients with life-threatening asthma are typicallytoo dyspneic to speak and will be perspiring profusely. They mayeven be drowsy or confused as t he ABGs further deteriorate.The breath sounds may be very difficult to hear, and no wheezing is apparent as the airflow is exceptionally limited. Peak flowis less than 25% of the personal best. They become bradycardicand are close to respiratory arrest. These patients require ED orhospital care and are often admitted to an intensive care unit.SAFETY ALERT If the patient has been wheezing and then there is an absence of awheeze (i.e., silent chest) and the patient is obviously struggling, thisis a life-threatening situation that may require mechanical ventilation.Diagnostic StudiesUnderdiagnosis of asthma is co mmon. A det ailed history isimportant in determining if a person has had previous attacks ofa similar nature, often precipitated by a known cause or trigger asdiscussed previously in the chapter. Because wheezing and coughare seen with a variety of disorders, this complicates the diagnosis of asthma. These disorders include COPD, pulmonary embolism, GERD, obesity, vocal cord dysfunction, and heart failure.Some controversy exists about how to best diagnose asthma.Common diagnostic measures are presented in Table 29-4. Ingeneral, the health care provider should consider the diagnosisof asthma if va rious indicators (i.e., clinical manifestations,CLASSIFICATION OF ASTHMA SEVERITYCLASSIFICATION OF ASTHMA SEVERITYPERSISTENTMILDMODERATECOMPONENTS OF SEVERITYImpairmentINTERMITTENTSymptomsNighttime awakeningsSABA use for symptomsInterference with normal activityLung function* 2 days/wk 2 /mo 2 days/wkNoneNormal FEV1 betweenexacerbationsFEV1 80%FEV1/FVC normal 2 days/wk, not daily3-4 /mo 2 days/wk, not dailyMinor limitationFEV1 80% predictedFEV1/FVC normalExacerbations requiring oralcorticosteroids0-1/yr 2/yr even in the absence of impairment ------------------------------ Consider severity and interval since last exacerbation. ----- Frequency and severity may fluctuate over time. --------------- Relative annual risk of exacerbation may be related to FEV1. mended Step forInitiating TreatmentStep 1Step 2Step 3†Reevaluate asthma control in 2-6 wk and adjust therapy accordinglyDaily 1 /wk, not nightlyDailySome limitationFEV1 60%-80% predictedFEV1/FVC reducedby 5%SEVEREContinuousOften, 7 /wkSeveral times per dayExtremely limitedFEV1 60% predictedFEV1/FVC reducedby 5%RiskStep 4 or 5†Guidelines for Using Table Patients should be assigned to the most severe step in which any feature occurs. Clinical features for individual patients may overlap across steps.Determine level of severity by assessment of both impairment and risk. Assess impairment by patient’s recall of previous 2-4 wk and spirometryresults. An individual’s classification should change over time as treatment is initiated. After treatment, the focus switches to level of control, not the classification of severity. Patients at any level of severity of chronic asthma can have mild, moderate, or severe exacerbations of asthma. Some patients with intermittent asthmaexperience severe and life-threatening exacerbations separated by long periods of normal lung function and no symptoms.Source: Adapted from Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Asthma Education
6. Explain the nursing management of the patient with COPD. 7. Describe the pathophysiology, clinical manifestations, collaborative care, and nursing management of the patient with cystic fi brosis. 8. Describe the pathophysiology, clinical manifestations, collaborative care, and nursin