Transcription
The Role of ThiamineDeficiency inAlcoholic Brain DiseasePeter R. Martin, M.D., Charles K. Singleton, Ph.D.,and Susanne Hiller-Sturmhöfel, Ph.D.A deficiency in the essential nutrient thiamine resulting from chronic alcohol consumption isone factor underlying alcohol-induced brain damage. Thiamine is a helper molecule (i.e., acofactor) required by three enzymes involved in two pathways of carbohydrate metabolism.Because intermediate products of these pathways are needed for the generation of otheressential molecules in the cells (e.g., building blocks of proteins and DNA as well as brainchemicals), a reduction in thiamine can interfere with numerous cellular functions, leading toserious brain disorders, including Wernicke-Korsakoff syndrome, which is foundpredominantly in alcoholics. Chronic alcohol consumption can result in thiamine deficiencyby causing inadequate nutritional thiamine intake, decreased absorption of thiamine from thegastrointestinal tract, and impaired thiamine utilization in the cells. People differ in theirsusceptibility to thiamine deficiency, however, and different brain regions also may be moreor less sensitive to this condition. KEY WORDS: thiamine deficiency; alcoholic brain syndrome;chronic AODE (alcohol and other drug effects); Wernicke’s encephalopathy; Wernicke-Korsakoffpsychosis; alcoholic cerebellar degeneration; AODR (alcohol and other drug related) structural braindamage; malnutrition; disease susceptibility; survey of researchAlcohol consumption can damagethe brain through numerousmechanisms, many of which arediscussed in the articles in this issue ofAlcohol Research & Health. One of thesemechanisms involves the reduced availability of an essential nutrient, thiamine,to the brain as a consequence of chronicalcohol consumption. This articledescribes the normal role of thiaminein brain functioning as well as thepathological consequences that resultfrom thiamine deficiency. Specificactions of thiamine on a cellular levelthen are reviewed, followed by a discussion of how alcohol affects the body’sprocessing and availability of thiamineas well as thiamine utilization by thecells. Finally, the article explores thehypothesis that people may differ in134their sensitivity to thiamine deficiencyand that different brain regions maybe more or less sensitive to a deficiencyin this important nutrient. Thiaminedeficiency is particularly importantbecause it can exacerbate many of theother processes by which alcohol inducesbrain injury, as described in otherarticles in this issue of Alcohol Research& Health.What Is Thiamine andWhat Are the Consequencesof Thiamine Deficiency?Thiamine, also known as vitamin B1, isan essential nutrient required by all tissues, including the brain. The humanbody itself cannot produce thiaminebut must ingest it with the diet. Thiaminerich foods include meat (e.g., pork)and poultry; whole grain cereals (e.g.,brown rice and bran); nuts; and driedbeans, peas, and soybeans. In addition,PETER R. MARTIN, M.D., is professorof psychiatry and pharmacology atVanderbilt University School of Medicineand director of the Vanderbilt AddictionCenter, Nashville, Tennessee.CHARLES K. SINGLETON, PH.D., isprofessor and chair in the Department ofBiological Science, Vanderbilt University,Nashville, Tennessee.SUSANNE HILLER-STURMHÖFEL, PH.D.,is a science editor for Alcohol Research& Health.Alcohol Research & Health
Thiamine Deficiency in Alcoholic Brain Diseasemany foods in the United States com monly are fortified with thiamine, includ ing breads and cereals. Humans requirea minimum of 0.33 milligrams (mg) thi amine for every 1,000 kilocalories (kcal)of energy they consume—in other words,people who consume a regular 2,000kcal diet per day should ingest a minimumof 0.66 mg thiamine daily (Hoyumpa1980). To provide a safety margin, adaily intake of 1.1 mg thiamine is cur rently recommended for adult womenand 1.2 mg for adult men.1 Studieshave found that most healthy peopletypically consume 0.4 to 2.0 mg thi amine daily (Woodhill and Nobile 1972).In the body, particularly high con centrations of thiamine are found inskeletal muscles and in the heart, liver,kidney, and brain (Singleton and Martin2001). In the tissues, thiamine is requiredfor the assembly and proper functioningof several enzymes that are importantfor the breakdown, or metabolism, ofsugar molecules into other types ofmolecules (i.e., in carbohydrate catabolism).Proper functioning of these thiamineusing enzymes is required for numer ous critical biochemical reactions in thebody, including the synthesis of certainbrain chemicals (i.e., neurotransmitters);production of the molecules makingup the cells’ genetic material (i.e.,nucleic acids); and production of fattyacids, steroids, and certain complexsugar molecules. In addition, inadequatefunctioning of the thiamine-usingenzymes can interfere with the body’sdefense against the damage (i.e., oxida tive stress) caused by harmful, highlyreactive oxygen molecules called freeradicals. (For more information, see thesection “Thiamine’s Actions in the Cell.”)Because thiamine and the thiamineusing enzymes are present in all cellsof the body, it would be plausible thatinadequate thiamine affects all organsystems; however, the cells of the nervoussystem and heart seem particularly sen sitive to the effects of thiamine deficiency.Therefore, the resulting impairmentin the functioning of the thiamine-usingenzymes primarily affects the cardiovas 1Lower levels are recommended for children, and slightlyhigher levels (1.4 mg thiamine per day) are recommendedfor pregnant and breast-feeding women.Vol. 27, No. 2, 2003cular and nervous systems. The classicalmanifestations of thiamine deficiency–related heart disease include increasedblood flow through the vessels in thebody, heart failure, and sodium andwater retention in the blood. In thebrain, thiamine is required both by thenerve cells (i.e., neurons) and by othersupporting cells in the nervous system(i.e., glia cells). Thiamine deficiency isthe established cause of an alcohollinked neurological disorder known asWernicke-Korsakoff syndrome (WKS),but it also contributes significantly toother forms of alcohol-induced braininjury, such as various degrees of cogni tive impairment, including the mostsevere, alcohol-induced persistingdementia (i.e., “alcoholic dementia”).These disorders are discussed in thefollowing sections.Wernicke’s Encephalopathy andKorsakoff ’s PsychosisWKS typically consists of two compo nents, a short-lived and severe conditioncalled Wernicke’s encephalopathy (WE)and a long-lasting and debilitatingcondition known as Korsakoff ’s psy chosis. WE is an acute life-threateningneurologic disorder caused by thiaminedeficiency. In affluent countries, wherepeople normally receive adequatethiamine from their diets, thiaminedeficiency is most commonly causedby alcoholism (Singleton and Martin2001); accordingly, in these countriesWE is primarily found in alcoholics(Ragan et al. 1999). The symptomsof WE include mental confusion,paralysis of the nerves that move theeyes (i.e., oculomotor disturbances),and an impaired ability to coordinatemovements, particularly of the lowerextremities (i.e., ataxia). For example,patients with WE may be too confusedto find their way out of a room or maynot even be able to walk. Many WEpatients, however, do not exhibit allthree of these signs and symptoms, andclinicians working with alcoholics mustbe aware that WE may be present evenif the patient presents with only one ortwo of them. In fact, neuropathologicalstudies after death indicate that manycases of thiamine deficiency–relatedencephalopathy may not be diagnosedin life because not all the “classic” signsand symptoms are present or recognized.Approximately 80 to 90 percent ofalcoholics with WE develop Korsakoff ’spsychosis, a chronic neuropsychiatricsyndrome characterized by behavioralabnormalities and memory impairments(Victor et al. 1989). Although thesepatients have problems rememberingold information (i.e., retrograde amne sia), it is the disturbance in acquisitionof new information (i.e., anterogradeamnesia) that is most striking. Forexample, these patients can engage ina detailed discussion of events in theirlives but cannot remember ever havinghad that conversation an hour later.Because of these characteristic memorydeficits, Korsakoff’s psychosis also iscalled alcohol amnestic disorder. It isstill somewhat controversial, however,whether Korsakoff’s psychosis always ispreceded by WE or whether it developsin fits and starts, without an overtepisode of WE.The role of thiamine in the develop ment of WKS is supported by findingsthat giving this nutrient to patientswith WKS reverses many of the acutesymptoms of the disease, although insome people certain chronic neuropsy chiatric consequences of previous thi amine deficiency may persist even withappropriate treatment (see Singletonand Martin 2001). In the most severecases, these persistent symptoms meetthe criteria of full-blown Korsakoff ’spsychosis. Other people may exhibit moresubtle neurological signs and symptoms,such as abnormalities in a brain regioncalled the cerebellum (as described inthe following section) and an inflam mation or degeneration of peripheralnerves (i.e., neuropathy) as well as changesin behavior and problems with learn ing, memory, and decisionmaking.In affluent countries such as theUnited States, where other forms ofmalnutrition are uncommon, thiaminedeficiency and the resulting WKSoccur most commonly among alcoholics.To date there are only a few estimates ofhow common WKS is among alcoholics.In autopsy studies, brain abnormalitiescharacteristic of WKS were present inapproximately 13 percent of alcoholics135
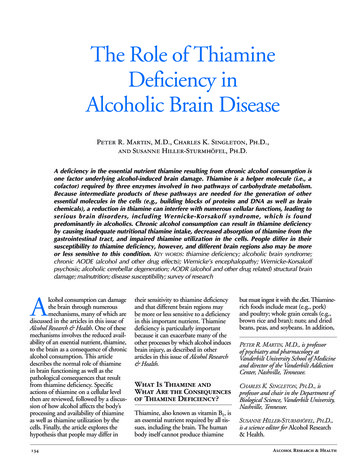
(Harper et al. 1988). These abnormalitiesinclude lesions in brain areas called themamillary bodies, thalamus, hypothala mus, brain stem, and cerebellum (seefigure 1). Other studies have found thatonly about 20 percent of alcoholics inwhom the presence of WKS was con firmed at autopsy had been diagnosedwith the disorder before death (Harper1998). Thus, the clinical presentation isnot always easily recognized by physicians;often examination of the brain at autopsyis required for definitive diagnosis.Although WKS in developed coun tries occurs most commonly amongalcoholics, other groups of patients arealso at risk of developing the disease.For example, all people who are mal nourished (e.g., because they are HIVinfected or are undergoing cancerchemotherapy) or who have a metabolicdisease leading to impaired thiamineabsorption (i.e., uptake) or utilizationcan develop thiamine deficiency. Patientswith severe kidney disease who are under going regular dialysis are also prone toencephalopathy, and a substantial por tion of them have been found to sufferfrom thiamine deficiency (Hung et al.2001). Finally, patients who receiveintravenous infusions of carbohydrates(e.g., the sugar dextrose) may experi ence episodes of thiamine deficiency,particularly if they are already at risk ofreceiving inadequate levels of this nutri ent because they are alcoholics, as thi amine is used in the metabolism of thosecarbohydrates (see Ferguson et al. 1997).Cerebellar DegenerationConsiderably more common than WKSamong alcoholics is a condition calledcerebellar degeneration, which typicallydevelops after 10 or more years of heavydrinking (Charness 1993). In autopsystudies, 40 percent or more of alcoholicsshowed signs of this condition (Torvik1987), which is characterized by shrink age (i.e., atrophy) of certain regions ofthe cerebellum. This brain area is involvedprimarily in muscle coordination. Italso is increasingly recognized for itsrole in various aspects of cognitive andsensory functioning (Parks et al. 2003).Accordingly, cerebellar degeneration isassociated with difficulties in movement136coordination and involuntary eye move ments, such as nystagmus. Cerebellardegeneration is found both in alcoholicswith WKS and in those without it, butbecause WKS patients typically have ahigher degree of cerebellar atrophy, itappears likely that thiamine deficiencyalso is the predominant cause of cere bellar degeneration.The frequent occurrence of cerebellardegeneration in alcoholics is consistentwith studies demonstrating that thecerebellum is particularly sensitive tothe effects of thiamine deficiency. (Formore information on these studies, seethe section “Differential Sensitivity ofVarious Brain Regions.”) As a result ofthis particular susceptibility, the effectsof thiamine deficiency would be expectedto appear first in the cerebellum, mani festing as cerebellar degeneration andits associated symptoms. In a smallernumber of patients, the consequencesof insufficient thiamine then wouldprogress to other brain regions and leadto more widespread brain dysfunction,including alcohol amnestic disorder oralcohol-induced persisting dementia.Thiamine’s Actionsin the CellTo understand the mechanisms throughwhich thiamine deficiency, whetherinduced by alcoholism or other causes,leads to brain damage, one first mustunderstand the normal role of thiaminein the cell. Investigations of this issuehave focused on three enzymes thatrequire thiamine as a cofactor. Theseenzymes are called transketolase, pyru vate dehydrogenase (PDH) and alphaketoglutarate dehydrogenase (α-KGDH);they all participate in the catabolism ofsugar molecules (i.e., carbohydrates) inthe body, as described in the followingparagraphs. Each of these enzymes con sists of several components that must beassembled to yield the functional enzyme,and the addition of thiamine is a criti cal step in this assembly process. As aresult, thiamine deficiency causes sub optimal levels of functional enzymes inthe cell, in addition to interfering withthe activity of those enzymes.Transketolase is an important enzymein a biochemical pathway called thepentose phosphate pathway. In this setof biochemical reactions, a moleculecalled glucose-6-phosphate, which isderived from the sugar glucose, ismodified by transketolase, yieldingtwo products—a sugar called ribose5-phosphate and a molecule calledreduced nicotinamide adenine dinu cleotide phosphate (NADPH) (seefigure 2). Both of these molecules areessential for the production of numer ous other important molecules in thecell. Ribose-5-phosphate is needed forthe synthesis of nucleic acids, complexsugar molecules, and other compounds.NADPH provides hydrogen atoms forchemical reactions that result in theproduction of steroids, fatty acids, aminoacids, certain neurotransmitters, andother molecules. In addition, NADPHplays an important role in the synthesisof glutathione, a compound that isessential in the body’s defense againstoxidative stress. To function properly,all cells require certain levels of NADPHand ribose-5-phosphate, and the bio chemical reaction mediated by trans ketolase is crucial for maintaining theappropriate levels of both molecules.The other two enzymes requiringthiamine, PDH and α-KGDH, alsoparticipate in different steps of thebreakdown and conversion of glucose6-phosphate through two consecutivechains of biochemical reactions calledglycolysis and the citric acid cycle (seefigure 3). The main function of thesepathways is the generation of a moleculecalled adenosine triphosphate (ATP),which provides energy for numerouscellular processes and reactions. Decreasesin the activities of PDH and α-KGDHcan result in reduced ATP synthesis,which in turn can contribute to celldamage and even cell death. In addition,proper functioning of PDH is essentialfor the production of the neurotrans mitter acetylcholine as well as for thesynthesis of a compound called myelin,which forms a sheath around the exten sions (i.e., axons) of many neurons,thereby ensuring the ability of theseneurons to conduct signals. The citricacid cycle and α-KGDH play a rolein maintaining the levels of the neuroAlcohol Research & Health
Thiamine Deficiency in Alcoholic Brain Diseasetransmitters glutamate, gamma aminobutyric acid (GABA), and aspartate,as well as in protein synthesis. Thus,the thiamine-using enzymes play numer ous vital roles in the functioning of cells,and particularly of neurons.When thiamine levels decrease, theactivity levels of all three enzymes arereduced to some extent. The specificreductions depend both on the enzymeand on the cell type studied (Singletonand Martin 2001). Overall, transketo lase activity may be the most sensitivemeasure of thiamine deficiency. Studiesusing rats found that transketolaseactivity may be reduced as much as 90percent in the brain regions that aremost sensitive to thiamine deficiency(Gibson et al. 1984). Substantial declinein transketolase activity resulting fromthiamine deficiency has even beenfound in various brain areas of alco holics who do not exhibit the clinicaland neuropathological signs of WE(Lavoie and Butterworth 1995), sug gesting that thiamine deficiency cancause adverse effects even before severebrain damage becomes obvious.Thiamine Uptake Into the CellThiamine is ingested with the diet, andto exert its effects in the cells it must betransported from the gastrointestinaltract to the tissues and cells. This trans port involves at least four steps: Uptake from the intestine into thecells that line the intestine Transport out of those cells intothe bloodstream Uptake from the blood into the tis sues and cells; for thiamine trans ported to the brain this also includescrossing the blood–brain barrier Transport within the cells to theareas where the thiamine is needed(e.g., to the cell’s energy factories,the mitochondria, where PDHand α-KGDH act, or to thenucleus, where thiamine regulatesgene activity).Vol. 27, No. 2, 2003Frontal lobeThalamusHypothalamusCerebellumMamillary bodyBrain stemFigure 1 Brain regions affected by thiamine deficiency include the cerebellum,mamillary bodies, thalamus, hypothalamus, and brain stem.GlucoseGlucose-6-PhosphatePentose PhosphatePathwayRibose-5-PhosphateNucleic acidsComplex sugarsCoenzymesTransketolase andother enzymes NADPHCoenzymes, Steroids,Fatty acids, Amino acids,Neurotransmitters, andGlutathioneFigure 2 The thiamine-dependent enzyme transketolase is an important enzymein the breakdown of glucose through a biochemical pathway called thepentose phosphate pathway. Glucose is first converted to a molecule calledglucose-6-phosphate, which enters the pentose phosphate pathwaywhere it is further modified by transketolase. During that reaction, twoproducts are formed—the sugar ribose-5-phosphate and a moleculecalled reduced nicotinamide adenine dinucleotide phosphate (NADPH).Ribose-5-phosphate is needed for the synthesis of nucleic acids, com plex sugar molecules, and other compounds called coenzymes that areessential for the functioning of various enzymes. NADPH provides hydro gen atoms for chemical reactions that result in the production of coen zymes, steroids, fatty acids, amino acids, and neurotransmitters. In addi tion, NADPH plays an important role in the synthesis of glutathione, acompound that is essential to the body’s defense against damage fromoxidative stress. Reduced transketolase activity interferes with all theseessential biochemical processes.137
These transport steps are accomplishedby one or more thiamine transportermolecules. Researchers recently haveidentified and cloned the gene for ahuman thiamine transporter (see Singletonand Martin 2001). However, the char acteristics of the thiamine transportprocess differ among different tissuesand cell types, suggesting that variantsof one transporter type or even differenttypes of transporters may exist. Indeed,a second thiamine transporter generecently has been cloned (Rajgopal et al.2001). As will be described in more detailin the section “Differential Sensitivity toThiamine Deficiency,” subtle variationsin the transporter molecule among cellsor among people, resulting in a reducedcapacity to transport thiamine, maycontribute to the differential sensitivityto thiamine deficiency.Once taken up into the cells, thi amine first is modified by the additionof one or more phosphate groups. Thecompound containing two phosphategroups (thiamine diphosphate [ThDP])is the actual active molecule that servesas a cofactor for the various thiaminerequiring enzymes. The levels of phosphatefree thiamine in the cell are uvatePyruvate DehydrogenaseAcetylcholineCitricAcid s of ThiamineDeficiency–Induced Cell DamageThiamine deficiency can lead to celldamage in the central nervous systemthrough several mechanisms. First, thechanges in carbohydrate metabolism,particularly the reduction in α-KGDHactivity, can lead to damage to themitochondria. Because the mitochondriaproduce by far the most energy requiredfor cellular function, mitochondrialdamage can result in cell death througha mechanism called necrosis (see Singletonand Martin 2001). Second, disturbancesassociated with thiamine deficiency insome cell types lead to apoptosis—aform of programmed cell death (or cellsuicide) that serves to remove damagedcells from the organism (see Singletonand Martin 2001). Third, alteredcarbohydrate metabolism can lead toa cellular state called oxidative stress(Calingasan et al. 1999; Todd andButterworth 1999), characterized byexcess levels of highly reactive moleculescalled free radicals and/or the presenceof insufficient levels of compounds toeliminate those free radicals (i.e., antiox idants, such as glutathione). Oxidativestress can lead to various types of celldamage and even cell eGlutamateGABAAspartateFigure 3 The thiamine-dependent enzymes pyruvate dehydrogenase (PDH) andα-ketoglutarate dehydrogenase (α KGDH) participate in the metabolismof glucose through two biochemical reactions, glycolysis and the citricacid cycle. The main function of these two sets of reactions is to gener ate adenosine triphosphate (ATP), which provides energy for the cells.Reduced PDH and α KGDH activity resulting from thiamine deficiencycan lead to less ATP synthesis, which in turn can contribute to cell dam age and even cell death. In addition, PDH is needed to produce the neu rotransmitter acetylcholine and to generate myelin, a compound thatforms a sheath around the extensions (i.e., axons) of many neurons,thereby ensuring proper neuronal functioning. The citric acid cycle andα KGDH play a role in maintaining the levels of the neurotransmittersglutamate, gamma-aminobutyric acid (GABA), and aspartate, as well asin protein synthesis.138low and are tightly regulated by rapidconversion to the phosphorylated forms.Alcohol’s Effectson Thiamine Uptakeand FunctionAs noted earlier, thiamine deficiency inaffluent countries clearly is linked toalcoholism, occurring in up to 80 per cent of alcoholics (e.g., Morgan 1982).However, only a subset of these alco holics develop brain disorders such asWKS. Moreover, identical twins (whoshare all of their genetic information)show greater similarity with respect toalcohol-induced brain disease than dofraternal twins (who share on average50 percent of their genetic informa tion). These two observations have ledto the conclusion that a genetic predis position to thiamine deficiency and itseffects may exist, as will be discussed inAlcohol Research & Health
Thiamine Deficiency in Alcoholic Brain Diseasemore detail in the section “DifferentialSensitivity to Thiamine Deficiency.”Research over the past 30 years hasidentified several mechanisms throughwhich alcoholism may contribute tothiamine deficiency. The most impor tant of these mechanisms (as discussedin Hoyumpa 1980) include: Inadequate nutritional intake Decreased absorption of thiaminefrom the gastrointestinal tract andreduced uptake into cells Impaired utilization of thiamine inthe cells.Inadequate Nutritional IntakeAlthough most people require a mini mum of 0.33 mg thiamine for each1,000 kcal of energy they consume,alcoholics tend to consume less than0.29 mg/1,000 kcal (Woodhill andNobile 1972). In fact, in an early studyof 3,000 alcoholics admitted to hospitalsbecause of alcohol withdrawal symp toms or other alcohol-related illnesses,40 percent exhibited periodic thiaminedeficiency during drinking binges, 25percent exhibited prolonged thiaminedeficiency with some periods of normalintake, and 35 percent exhibited con tinuous thiamine deficiency (Leevy andBaker 1968). A later study found thatalcoholic patients had significantly loweraverage levels of a thiamine compoundcontaining one phosphate group (i.e.,thiamine monophosphate), but theaverage levels of free thiamine and ThDPwere similar in alcoholics and controlsubjects (Tallaksen et al. 1992). However,some of the alcoholics in that studyhad extremely high levels of free thi amine, suggesting that they may havehad a problem in the steps that lead tothe conversion of thiamine into itsactive, phosphate-containing form.Decreased Uptake of ThiamineFrom the Gastrointestinal TractAnimal studies have helped elucidate themechanisms of normal and alcoholimpaired thiamine uptake from the gas trointestinal tract into the blood andVol. 27, No. 2, 2003cells. To be used by the body, thiaminemust cross a number of barriers, firsttransferring across the membranes of thecells lining the gut (i.e., enterocytes),then entering those cells, and then cross ing the membranes at the other end ofthe cells to enter the bloodstream. At lowthiamine concentrations, such as thosenormally found in the human body, thistransfer is achieved by a specific thiaminetransporter molecule that requiresenergy. This is called an active transportprocess and seems to be associated withthe rapid addition of two phosphateThis finding suggests that TPK is lessactive in the alcoholics.Thiamine malabsorption couldbecome clinically significant if com bined with the reduced dietary thiamineintake that is typically found in alco holics, when other aspects of thiamineutilization are compromised by alcohol,or when a person requires increased thi amine amounts because of his or herspecific metabolism or condition (e.g.,in pregnant or lactating women).Impaired Thiamine UtilizationResearch over thepast 30 years hasidentified severalmechanisms throughwhich alcoholismmay contribute tothiamine deficiency.groups by the enzyme thiamine diphos phokinase (TPK) once the thiamine isinside the cell. At high thiamine concen trations, however, such as can be achievedafter additional thiamine is administered,thiamine transport occurs through a pas sive process—that is, a mechanism thatrequires no energy.Acute alcohol exposure interferes withthe absorption of thiamine from the gas trointestinal tract at low, but not at high,thiamine concentrations (Hoyumpa1980). Furthermore, in studies using rats,the activity of the TPK enzyme from vari ous tissues decreased with acute alcoholexposure to about 70 percent of the activ ity level in control animals, and withchronic alcohol exposure to about 50 per cent (Laforenza et al. 1990). Although nostudies have addressed whether alcoholdirectly affects TPK in humans, indirectanalyses have found that the ratio of phos phorylated thiamine (primarily ThDP)to thiamine is significantly lower in alco holics than in nonalcoholics (Poupon etal. 1990; Tallaksen et al. 1992)—that is,that less thiamine is converted to ThDP.The cells’ utilization of thiamine can beaffected in different ways by chronic alco hol use. As mentioned earlier, once thi amine is imported into the cells, it is firstconverted into ThDP by the addition oftwo phosphate groups. ThDP then bindsto the thiamine-using enzymes, a reactionthat requires the presence of magnesium.Chronic alcohol consumption frequentlyleads to magnesium deficiency, however(Morgan 1982; Rindi et al. 1992), whichalso may contribute to an inadequatefunctioning of the thiamine-using enzymesand may cause symptoms resemblingthose of thiamine deficiency. In this case,any thiamine that reaches the cells cannotbe used effectively, exacerbating any con currently existing thiamine deficiency.Abstinence from alcohol andimproved nutrition have been shown toreverse some of the impairments associ ated with thiamine deficiency, includingimproving brain functioning (Martin etal. 1986). Researchers also administeredthiamine to alcoholic patients and labo ratory animals and found that this treat ment reversed some of the behavioraland metabolic consequences of thiaminedeficiency (Victor et al. 1989; Lee et al.1995). Most recently, researchers admin istered different thiamine doses for twodays to a group of alcoholics undergoingdetoxification, none of whom were diag nosed with WKS, and then tested theparticipant’s working memory. Thesestudies found that participants whoreceived the highest thiamine dose per formed best on tests of working memory(Ambrose et al. 2001).139
Differential Sensitivityto Thiamine DeficiencyDifferences in SensitivityAmong PeopleSeveral findings suggest that not all peo ple are equally sensitive to thiamine defi ciency and its consequences. For exam ple, although thiamine deficiency mayoccur in up to 80 percent of alcoholics(Tallaksen et al. 1992; Hoyumpa 1980;Morgan 1982), only about 13 percentof alcoholics develop WKS (Harper etal. 1988). This means that the severestconsequences of thiamine deficiencydevelop only in a subset of people whoconsume alcohol and have poor nutri tion on a chronic basis. A possible expla nation for this differential sensitivity isthat some people are genetically predis posed to develop brain damage afterexperiencing repeated episodes of alcoholrelated thiamine deficiency. To investi gate this hypothesis, researchers havestudied the activities of thiamine-usingenzymes in patients with and withoutKorsakoff ’s psychosis, arguing that vari ants of these enzymes may exist thatcould differ in their susceptibility tothiamine deficiency. The results of theseinvestigations, however, have beeninconsistent.2One study (Blass and Gibso
the brain through numerous and that different brain regions may rich foods include meat (e.g., pork) mechanisms, many of which are be more or less sensitive to a deficiency and poultry; whole grain cereals (e.g., discussed in the articles in this issue of in this important