Transcription
3. PHASE 1:URGENT ANDDIAGNOSTIC36 slides, about 1.5 hourJK Mitchell, DDSTreatmentPlanningTutorial
Learning Objectives1. Recognize Key Decision points in a treatment plan.2. Give examples of what treatments go into Phase 1,2,3.3. Be able to explain space infections, what influences theirlocation, the sequence of treatment, and why Ludwig’sAngina and Parapharyngeal space infections are asignificant threat.4. List when antibiotics are indicated and when they are notindicated.5. List and clinically recognize the three treatment planningindications for considering an orthodontic evaluation.Recognize when a case is disease controlled for referral.6. Define how to determine restorability and list thesequence of restorative and endodontic treatment.JK Mitchell, DDS
Phase 32Data Collection Tx PlanWe’ve developed a Problem and Diagnosis List, and havesome sense for what kind of treatment this patient isinterested in both tooth by tooth and overall.Now we need to start to develop our Treatment PlanCollect Data RadiographicInterpretation OM exam* MakeimpressionsDevelop TxPlan Problem List Diagnosis List DevelopPhase 1 Plan Develop Phase 2Plan, alternates Develop Phase 3Plan, alternates* Pt presentGray work done between apptsJK Mitchell, DDSPhase 1, 2Approval DXR appt* Eval casts Reviewcharting,dental exam Get ptsignature on txplan estimateSimpleApprove at DXR*Phase 3Includes FixedProsAfter Phase 2completed, approvewith a Fixed Prosfaculty member*Phase 3 TxPlanning BoardIf RPD planned,schedule for TxPlanning Board.*Exception: C/RPD,which is approvedby Rem Pros facultymember
Moving from Diagnosis to aTreatment Plan with PhasesMATCHING DIAGNOSES AND TREATMENTSDEVELOPING PRIORITIES WITH PATIENTWHAT GOES IN WHICH PHASEJK Mitchell, DDS
Where do you start?3 What do you do with this list ofproblems and diagnoses andpatient concerns and who knowswhat else? How do you get from adisorganized mess to an organizedplan a logical sequence thataddresses all problems in the rightorder at that right time? When it’s time to sort out yoursock drawer, you dump them allout and inspect them.Then you match them up intopairs, right?JK Mitchell, DDS
With a treatment plan 4 You dump out all the diagnoses and inthe light of the patient’s: Medical concerns Personal preferences Economic resourcesyou plan at least one (usually several)reasonable treatment options for eachone. Looking at all your socks, you mightsort them by function maybeWorkout socks vs Dress socks vs Crazycolor socks, whatever. Once you’ve paired up diagnoses withtreatments, decide which phase eachof these treatments belongs in.Let’s try an example. Remember Jill?JK Mitchell, DDS
Remember Jill’s Problem List?Developtreatmentplan51.Chief concern identified as“stained teeth” and “spacesbetween teeth.”2.Jill’s medical history includesType 1 diabetes. Last HbA1cwas 4 mo ago.3.Pain “pain with thermalstimuli” in site 19.4.You also noted: JK Mitchell, DDSPeriodontal problemsCariesMissing teethOcclusal plane problems
Start thinking of possible treatments61.Chief concern identified as“stained teeth” and “spacesbetween teeth.”2.Jill’s medical history includesType 1 diabetes. Last HbA1cwas 4 mo ago.Pain “pain with thermalstimuli” in site 19.3.You also noted:4. Periodontal problemsCariesMissing teethOcclusal plane problemsJK Mitchell, DDS1.Several options . Porcelainveneers? Orthodontics?Bleaching and directbonding?2.Get current HbA1c3.Diagnose pain #19, then gofrom there to develop tx plan.4.Other problems: Perio- D0180, scale, root planeCaries- list needed restorationsMissing teeth- options implants?RPDs?Occlusal plane problems. Wild card!How are we going to manage this? land mine. Keep an eye on this!
And focus on the Key Decision PointsDeveloptreatmentplan7Knowing Jill’s problems, you look at her study casts, and start thinking. Some problemsdon’t have any real options her diabetes is going to be followed up with an HbA1c. Butother problems have options, and the big decisions that are going to determine the overalldirection of the case are key decision points. leTreatmentsAdvantagesDisadvantagesPorcelain VeneersBest EstheticsUsually last longerMore expensiveRequires tooth prepVital Bleach Composite BondingLess expensiveNo prep /reversible,Not as long lastingImplants, fixed partial Very functionaldenture (“bridge”)Not removableRemovable partialdenture (RPD)Less expensiveNo surgery requiredReasonably quick treatmentExpensive, requires surgeryTakes up to a year to complete (healing,etc)Less effective chewing, looseHas to be taken out at night.Tends to increase caries, perio riskWhat if you can’t tell if there’s enough space? Or how it might work? To help you seeBack towhich might be possible, you will often do a diagnostic set-up in wax.JK Mitchell, DDSReview
But which would work for Jill?Developtreatmentplan8 You’ve had a chance to talk to Jill. You know her concerns pretty well, and youhave a sense for her priorities. BUT You always want to offer all feasible treatment plans! Maybe she hasn’tsaid she’s interested in implants because she’s heard they cost 50,000. If shefinds out that here they are only 10,000, she might be delighted to do that.Maybe not. Maybe she just doesn’t want screws in her jaw. You really never knowunless you offer all the options with estimates. Bottom line never assume you know what people can or can’t afford. Everydentist has a story of some poorly dressed patient who paid cash for the highestend treatment plan. (Go read the story of why Stanford University was foundedfor a useful lesson on that idea.) And never talk down to a patient. After you give Jill some ball-park estimates and talk over the advantages anddisadvantages of each treatment, she gives you some direction on what shewants. Now you can start matching up problems with her preferred treatments.JK Mitchell, DDS
Matching up Jill’s preferred treatments:Developtreatmentplan9Vital Bleaching(lighten color)Medical HistoryType 1 diabetesOcclusal plane#2,3,4supraeruptedVerify control withcurrent HbA1cHigh CariesCRA 22#8,92,4D0180Scl/RPJK Mitchell, DDSEndodontic#19- pain withthermal stimuliCrown#3,4Extract 2PeriodontalDx ModerateEsthetic ConcernsStained teeth and “spacesbetween teeth”Dietary counselingDaily Fluoride x4Office Fluoride q 3 moXylitol 3x/dayComposites 8,9Amalgam 2,4Direct BondedComposites(close spaces)Verify diagnosis,RCT #19Missing #29-32MandibularRPD Land mine. Be careful!!!
Matching up Jill’s preferred treatments:Developtreatmentplan9Vital Bleaching(lighten color)Medical HistoryType 1 diabetesOcclusal plane#2,3,4supraeruptedCrown#3,4Extract 2So which ofthese doyou doD0180Scl/RPEndodontic#19- pain withthermal stimulifirst? Dietary counselingHigh CariesCRA 22#8,92,4PeriodontalDx ModerateJK Mitchell, DDSEsthetic ConcernsStained teeth and “spacesbetween teeth”Verify control withcurrent HbA1cDaily Fluoride x4Office Fluoride q 3 moXylitol 3x/dayComposites 8,9Amalgam 2,4Direct BondedComposites(close spaces)Verify diagnosis,RCT #19Missing #29-32MandibularRPD Land mine. Be careful!!!
What order do we do these things in?Developtreatmentplan10It helps to think about what our priorities are 1.First Priority. Address urgent problems, like relieving pain,following up on health concerns, and making sure a suspiciouslesion isn’t cancer. You also need to get areas of uncertaintycleared up before you can formulate a final treatment plan.2.Control Disease and Preparatory Treatment. Caries andPeriodontal disease need to be controlled before we move on toany other treatment. Any other treatment to prepare the dentitionfor final rehabilitation treatment is done here.3.Rehabilitation. Now we can turn to providing restoration of form,function, and esthetics.JK Mitchell, DDS
Where do those priorities fit with our plan?11CollectdataDeveloptreatmentplanGet patientand facultyapprovalJK Mitchell, DDSTreatmentPhase 1.TreatmentPhase 2.Urgent atmentPhase 3.DefinitiveRestorativeMaintenance
What fits in each phase:Developtreatmentplan12Phase 1.Urgent & Problem SolvingAddress urgent problemsand answer key questionsthat will affect the finaldirection of treatment plan.Urgent problems:Answer medical questions,Relieve pain, Biopsysuspicious lesions,Provisional replacement ofmissing anterior teethSample Key Questions:Is this tooth restorable?Does endo need to beredone? Can an implant beplaced there? Should wedo ortho first?JK Mitchell, DDSPhase 2.Disease ControlControl disease and preparepatient for Phase 3. Usuallydoes not leave pt worse if donot progress to Phase 3.Ortho- arrange teeth toprepare for prosthetic care.Endo- treat pulpal pathosisPerio- treat perio diseaseSurgery- remove hopelessteeth, place implants, shapebone for denture placementCaries- Control disease withdiet counseling, fluoride, etc.Operative to restore cariouslesions.Phase 3.Definitive RestorativeRestore form, function,and esthetics.Ortho- definitive careEndo- when done forrestorative reasonsPerio- Esthetic,mucogingival, or changingridge shape in conjunctionwith prosthetic treatment.Fixed Pros- Crowns, fixedpartial denturesRemovable Pros- RPD,complete dentures.Back toReview
Now start sorting!!Developtreatmentplan13So which category-which bin- do youthrow each of Jill’s treatments into?JK Mitchell, DDS
DeveloptreatmentplanSort the socks by function:14Medical HistoryType 1 diabetesVerify control withcurrent HbA1cVital Bleaching(lighten color)Esthetic ConcernsStained teeth and“spaces”Direct BondedComposites(close spaces)Composites 8,9Amalgam 2,4Endodontic#19- pain withthermal stimuliVerify diagnosis,RCT #19Phase 1.Urgent & DiagnosticJK Mitchell, DDSCariesCRA 22#8,92,4PeriodontalDx ModerateDietary counselingDaily Fluoride x4Office Fluoride q 3 moXylitol 3x/dayOcclusal plane#2,3,4supraeruptedCrown#3,4Extract 2Missing #29-32MandibularRPDD0180Scl/RPPhase 2.Disease Control,PreparatoryPhase 3.Rehabilitation
But wait Developtreatmentplan15 You’re probably thinking “since when are stained teethand spaces part of Disease Control?” and you’d be right. But- That was her chief concern! If we don’t address thatfairly soon, we aren’t being responsive to her needs.Besides, since we’re going to be doing composites on #8and 9, we would need to do the vital bleaching first (sowe would be selecting the correct shade, right?) so whynot go ahead and meet her esthetic needs? A happypatient refers her friends JK Mitchell, DDS
Begin with the end in mind.Developtreatmentplan16The complexity comes when you learn how many options thereare to treat any particular diagnosis.Take a look at Jill: Her carious lesions in #2, 4 could be restored with eithercomposite or amalgam. Which is best? Depends. But wait, didn’t you say you’re going to extract #2 because it’ssupraerupted and there isn’t enough space for an RPD? Orcrown it to make it shorter so the RPD will fit? Yep. You need to figure all that out before you“Boom”start drilling away on anything. Occlusion always has to be part of the plan!JK Mitchell, DDS
Treatment before Treatment Planning Board17 But there are going to be times when you can’t get aTreatment Planning Board appointment for a few weeks andyou’re going to ask “can I start on the directs while I’mwaiting for Treatment Planning Board?” Well, you can, if you know the difference between directsthat will be done in any treatment plan, and those thatdepend on which Phase 3 plan is chosen. So- do your homework. In your Phase 2 Treatment Plan(which will be approved at DXR) sequence it so that you knowwhich direct restorations will not be affected by decisionsmade at Treatment Planning Board.JK Mitchell, DDS
Phase 1: Urgent and ProblemSolvingUrgent Treatment: Problem Solving: JK Mitchell, DDSSpace InfectionsAcute riodonticsEndodonticsRestorability
Phase 1. Urgent and Problem SolvingPhase 1Urgent18 Let’s start with urgent. It’s easyto define: Pain. Bleeding.Swelling. Infections. But alsogiving a patient a front tooth sothey can go to work can beurgent. We’ve covered pain already,and you will learn options forthat missing front tooth inProsthodontics. Bleeding (likefrom trauma) will be handled inOral Surgery. What about swelling? Usuallyswelling means an infection.JK Mitchell, DDSSpace InfectionsGeneral concepts on management:1. Once the infection is out into the fascial spaces,just starting endo or removing the tooth is notenough. First, the space infection must bemanaged, then the original problem (endo, 3rdmolar, etc) is addressed.2. “Pus must pass” - an incision must be made intothe infected area and a drain put in.3. Generally, these should be managed by an Oraland Maxillofacial Surgeon. Make friends with oneyou can really learn a lot from them
Red Flags19 Any of these symptoms shouldmake you sit up and pay attention! FeverSwellingTrouble swallowingTrouble breathingTrismus If you can’t find the origin of theproblem, or are not sure you havesolved the problem, get thepatient to someone who can (iean Oral Surgeon)! Follow these patients! Call themeven if they don’t come back tothe clinic.JK Mitchell, DDS
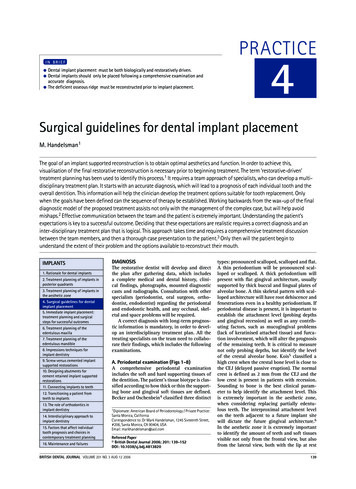
Applied Head and NeckLet’s put your Head and Neck Anatomyclasses to practical use!This is a drawing I made to help visualizeand remember space infections.Key concepts:- Infections usually start from the apex ofan abscessed tooth or pericoronitis on a 3rdmolar.- Drainage direction and structure location(like muscle origin and insertion) determinewhich space is infected.-Some of the spaces are connectedinfection can flow around. Life-threatening:Ludwigs Angina is bilaterally submental ,sublingual, and submandibular, leaving noroom for the tongue but into the airway.Parapharyngeal space can go into the neckspaces which blocks off the airway.Both of these can compromise theairway and are life-threatening.- There are only 10 of these spaces, and ifyou think about where the muscles are andhow they relate to the teeth, you can have apretty good guess of which space is which.There’s a copy of this on the class website.Print it out so you can read it.You may need it some day JK Mitchell, DDS20Back toReview
Case 1. SuzannePhase 1Urgent21 Which space is this mostlikely to be? aSubmandibular bSubmental cSublingual Which tooth is most likelyThis patient remembers having a badtoothache “a month or two ago” and then adull ache that started about 5 days ago. Twodays ago she woke up with a swelling whichhas rapidly worsened to this condition. Theswelling is relatively hard with a softfluctuant central area. She has a temp of101.2.JK Mitchell, DDSto be the origin? a#26 b#29 c#31
Indications for AntibioticsPhase 1Urgent22Not indicated:Indicated for:PulpitisPersistent infectionsNecrotic pulp radiolucencyApical periodontitisSinus tractSystemic illness:Temp 100, Malaise,LymphadenopathyLocalized, fluctuant swelling(may need to be drained, butstill may not need AB’s)Progressive infection:Trismus, Cellulitis,Increasing swelling“I don’t have time to takethat tooth out or start aroot canal today, so I’ll giveyou this to hold you till Ican get you in.”Osteomyelitis (OMFSreferral!)“I’d feel more comfortableif you took some antibiotics”The patient wants aprescription for something JK Mitchell, DDS While we’re talking about this,let’s make sure you understandwhen antibiotics work and whenthey don’t work. Antibiotics are still hugelyoverprescribed for many things,dentistry among them. The idea that antibiotics willhelp control pain in pulpitis orperiapical inflammation hasbeen disproven in study afterstudy but many dentists stillstubbornly cling to the belief,even when confronted with theevidence.“Don’t be that guy”Back toReview
Understanding Pain ManagementPhase 1Urgent23 You will take your Pharmacology coursein the Junior year, but in the mean time,here is the basic plan for dealing withpain. Over the counter medications are quiteeffective for mild-moderate pain. We’vegot research. Reassure your patientconfidence works. Ibuprofen is dose-dependant. It is agood pain reliever at lower doses: 400 mg every 4 hours (q4h)600 mg every 6 hours (qid)But for it to be anti-inflammatory, itneeds to be the highest dose: 800 mg every 8 hours (tid)And Ibuprofen has a very slow onset ofrelief (40 minutes). Start pts on it beforeanesthetic wears off, and have themtake it by the clock instead of waitinguntil they hurt.JK Mitchell, DDSMild Aspirin Tylenol Ibuprofen 400mg, 600 mgModerate Ibuprofen 800 mg threetimes a day (tid) by the clock Consider adding narcoticsSevere Mod breakthrough med: Narcotics q4h as needed
Case 1. SuzannePhase 1Urgent24You take a radiograph and see this image.The patient wishes to save the tooth.What do you do?Start a non-surgical root canal treatmenta (endo) and drain through the access, startantibiotics.and drain the abscess surgically,b Inciseplace a drain, and when the acuteinfection is resolved start endo.Incise and drain the abscess surgically,c place a drain and start endo the same dayto remove the source of the infection.After the procedure, what will youprescribe/recommend?Suzanne is an otherwise healthypatient with no allergies to anymedications.a Antibioticsb Over the counter pain medicationsc Narcotic pain medicationsJK Mitchell, DDS
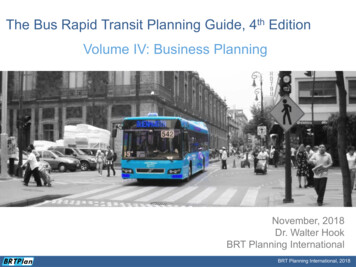
Acute Periodontal InfectionsPhase 1Urgent25 Remember learning about an acute periodontal abscess?There is another kind of periodontal disease that is quitepainful.It used to be called “trench mouth” because it was commonin the trenches in WWI. They thought it was an infectiousdisease, but really it was only because in the trenches theywere getting shot at so they were stressed out and nutritionwas poor.It was common again in the early days of HIV before currentmedications were available. Now you can see it on collegecampuses during finals (cold pizza, anyone?) or boot camps orin anyone who is stressed. It’s called NUP or NecrotizingUlcerative Periodontitis.The bacteria invade the gingival papilla causing rapid loss ofpapilla, bone, and attachment mechanism. It has a classicgrayish slimy “pseudomenbrane” and “punched out” papillaeand a really vile smell that you will never forget once youhave gotten a whiff. Tends to attack first molars andmandibular anterior molars.Treatment? Sleep, good nutrition, and good oral hygiene aswell as antibiotics.JK Mitchell, DDS“Pseudomembrane”“Punched out” papillaeScratch n’ sniff forcharacteristic odor
Phase 1. Problem SolvingPhase 1ProblemSolving26 Problem solving is a harderconcept, and we need to spendsome time on this one. Let’s look at the kinds ofquestions we might be asking: Let’s look at #19Let’s assume that we would really liketo keep #19 for the treatment plan. Sowhat are you thinking .1. Does it need endo?2. Is it restorable?JK Mitchell, DDS Is that soft tissue lesion anythingwe should worry about?Is this tooth restorable?Does the endo need to be redonebefore I put a crown on it?Can I plan implants for that space?How many will I need?Should we do ortho first?
Answer Medical Questions27 As you were taught in OralMedicine, you are the besttrained person to know theparameters for dental care. But if there are issues inthe medical history thatrequire clarification ortesting, the time to get theanswers you need is beforeyou start treatment.JK Mitchell, DDSPhase 1ProblemSolving
Specialty Consults: OrthodonticsPhase 1ProblemSolving28 Ortho- it’s not just for kids anyThis patient had a single large spacebetween his centrals partly closed withcomposite. Imagine how BIG these teethwould be if veneers were placed on themin this position! But after ortho, the spacewas shared and the teeth could be sizednormally for a nice result.JK Mitchell, DDSmore! It can be quite helpful in settingup restorative care. You will learn more in your orthoclass, but for now, consider orthowhen dealing with:1.Space or crowding issues ifyou’re doing Fixed Pros2.Implants! Once they are in,you can’t move them, or theteeth around them. Think ofortho before you put inimplants!
Orthodontic Adjunctive Care:Molar Uprighting293. Problem: Tipped molar. Sometimesyou want to use for an FPD abutment,but you can’t prepare it correctly if it’stipped too far- you’ll see why in FixedPros lab. But notice the center of rotation- apoint in the center of the root. This usually means the crownrotates above the plane ofocclusion- keep that in mind foryour planning. Finally, ortho is NOT a fairy-dustanswer: you can’t just say “oh, I’llmove those teeth” without knowingthat it is feasible. You have to moveteeth where there is bone, forexample. It’s harder than it looks .JK Mitchell, DDSIn this case, the toothis well below the planeof occlusion, so afteruprighting it willprobably only needminor adjustment. Butif it was at or above theplane, it would end upwell above it andmaybe unusable.Phase 1ProblemSolving
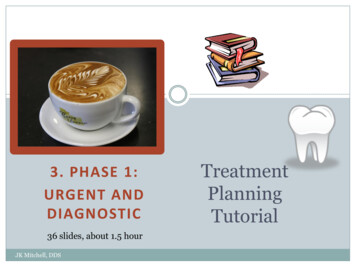
Adjunctive Orthodontic CarePhase 1ProblemSolving30BUT Before an orthodontist will considerthe case, they will ask the referringdentist two questions: Is the patient caries active?Does the patient have active periodisease? Why? Because Ortho treatment willaggravate both of these diseasesand the patient will be worse offthan if they had not had thetreatment. You want to have a good workingrelationship with your referringorthodontists to get these diseasesunder control before placingappliances.JK Mitchell, DDSNote the pattern of caries and white spotlesions around areas where the bracketswere bonded, where the S.Mutans ladenplaque builds up. This is not the estheticresult orthodontists want to show on theirwebsites! It’s much harder to brush andfloss around ortho appliances, too, so periodisease is a consideration. Back toReview
ImplantsPhase 1ProblemSolving31 We will talk more aboutimplants in a later tutorial,but for now let’s say thepatient is interested. Areimplants a feasible option? The major questions are: Is there enough bone to supportan implant?Is there enough space for thecrown /FPD?Is the patient a good candidatehealth-wise and psychologically? You will go through patientservices, who will assign themto one of three departmentsfor an evaluation. (OralSurgery, Perio, GPR)JK Mitchell, DDS
Periodontics32 The question- Is tooth #7 savableperiodontally? If so, what wouldbe required? This patient would require aD0180 rather than just a prophy,right? Your perio exam will look at eachtooth on it’s own, but also keepin mind your overall treatmentplan, and what role this toothmight play. Are you thinking of using thattooth to support an FPD? AnRPD? You might run that pastthe periodontist as part of theoverall consideration.JK Mitchell, DDSPhase 1ProblemSolving
EndodonticsPhase 1ProblemSolving33 You’ve already learned how toWhat if you are thinking of putting crowns onthese teeth for esthetics? Would you need toredo these endo txs first? Would it be smart todo that? I’d sure ask an endodontist.JK Mitchell, DDSevaluate a tooth endodonticallygenerally do your own diagnosisbefore you refer. But what if the tooth is alreadyendodontically treated, but doesn’tlook right radiographically orclinically? Best answer is an endoconsult. What if an endo treated tooth still hasnot been restored correctly? If theendo fill itself (the gutta percha) hasbeen exposed to saliva for more than3-4 weeks, consider redoing the endo.The oral bacteria have contaminatedthe endo fill and it may fail. Again, tell the Endodontist yourrestorative plan so they can give youthe best advice!
Is this tooth restorable?Phase 1ProblemSolving34Let’s get to the bottom line: You generally can’ttell from a radiograph or even visually if a toothis restorable or not if it’s borderline. What works? Remove the caries and see if youcan get a matrix band on it. If you can get amatrix band on it, then you can restore it. Crucial concept: you must determine if thetooth is restorable before you do the endo.Why?1. Let’s say you don’t, and after the endo youfind out the tooth is NOT restorable! Ouch!(Pull out your checkbook ) Planning keepsyou from the embarrassing position of takingout a tooth you just did a root canal on.2. A good restoration helps hold on the rubberdam retainer.3. With a good restoration in place, you canbetter control the sodium hypochlorite(bleach) that’s used to irrigate the root canalspace- it won’t leak out through the deepcavity if there’s a nice restoration in it. JK Mitchell, DDSBack toReview
Summary: Overview of estionsRestore form,function, BleedingSwellingPhase 1.Urgent & DiagnosticJK Mitchell, DDSPhase 2.Disease ControlPreparatoryPhase 3.Rehabilitation
Review of Learning Objectives36If you have trouble with any of these, click on the link. Some cover severalpages before the Return to Review button appears. Be sure you know all theterms in blue or red in the tutorial.1. Be able to recognize Key Decision points in a treatment plan.2.Give examples of what treatments go into Phase 1,2,3.Be able to explain space infections, what influences theirlocation, the sequence of treatment, and why Ludwig’s Anginaand Parapharyngeal space infections are a significant threat.4. List when antibiotics are indicated and when they are notindicated.5. List and clinically recognize the three treatment planningindications for considering an orthodontic evaluation.Recognize when a case is disease controlled for referral6. Define how to determine restorability and list the sequence ofrestorative and endodontic treatment.3.JK Mitchell, DDS123456
Now that you know the basics Read Chapter 3 pg 53-65 (before occlusion): Developing theTreatment Plan Read Chapter 6 pg 113-135: Acute Phase of Treatment.Gives you a very good overview of how to handle anemergency patient start to finish. Also has a good review ofthe pain material we covered last semester, but in moredetail.JK Mitchell, DDS
Nicework!Nicework!42St James ChurchChipping CampdenJK Mitchell, DDS
Case 1: You chose a “Submandibular Space” Correct! You probably noticed thatthe swelling is on one sideonly (eliminating theunpaired Submental spacewhich would be right in themiddle) and that it is underthe Mylohyoid muscle. Nice work!ReturnJK Mitchell, DDS
Case 1: You chose b “Submental Space” Probably not. Check the diagram and tryagain!ReturnJK Mitchell, DDS
Case 1: You chose c “Sublingual space” Probably not Check the diagram and tryagain!ReturnJK Mitchell, DDS
Case 1: You chose a “#26” Probably not Check the diagram and tryagain!ReturnJK Mitchell, DDS
Case 1: You chose b “#29” Probably not. Check the diagram and tryagain!ReturnJK Mitchell, DDS
Case 1: You chose c “#31” Correct! You probably noted thatthe most likely tooth to bebelow the mylohyoidinsertion is a second molar,so #31 is a likely option. Nice work!ReturnJK Mitchell, DDS
Case 1. You chose a- Endo Not really the best choice. Read the slide on infectionsand try again!ReturnJK Mitchell, DDS
You chose b.50 I&D, delay endo - Correct! Of course you want to getthe endo done as soon asyou can, but generallypatients like this will havetrouble opening and youwill make them much moresore if you try to do it all atonce. Good job!ReturnJK Mitchell, DDS
Case 1. You chose c- I&D Endo Not really the best choice. Read the slide on infectionsand try again!ReturnJK Mitchell, DDS
Suzanne: You chose AntibioticsNot indicated:Indicated for: YES!PulpitisPersistent infections This is clearly a case forNecrotic pulp radiolucencyApical periodontitisSinus tractSystemic illness:Temp 100, Malaise,LymphadenopathyLocalized, fluctuant swelling(may need to be drained, butstill may not need AB’s)Progressive infection:Trismus, Cellulitis,Increasing swelling“I don’t have time to takethat tooth out or start aroot canal today, so I’ll giveyou this to hold you till Ican get you in.”Osteomyelitis (OMFSreferral!)antibiotics. The patient has afever and a progressinginfection. Good choice, doctor! Keep clicking, though“I’d feel more comfortableif you took some antibiotics”The patient wants aprescription for something ReturnJK Mitchell, DDS
Suzanne: You chose OTC Pain Meds Good idea! Not because that is going to be enough for her pain afterthe I&D surgery (it won’t be) but because it is antiinflammatory. You would give it at the highest dose: 800 mg every 8 hours (tid) She will have less overall pain if the inflammation iscontrolled, not just the pain. Keep looking, thoughReturnJK Mitchell, DDS
Suzanne: You chose Narcotic Pain Meds Of course. This woman is going to be in a lot of pain after weopen up her neck, drain out a lot of pus, and put in adrain. This is not a fun day. Ibuprofen is not going tokeep her comfortable. Patients need narcotics for this sort of pain, and you arewise to prescribe it in advance of the pain. Keep looking, thoughReturnJK Mitchell, DDS
Treatment Planning Board appointment for a few weeks and you’re going to ask “can I start on the directs while I’m waiting for Treatment Planning oard?” Well, you can, if you know the difference between directs that will be done in any treatme