Transcription
A Personal Guide toManaging Chest DrainageDry SealChest Drainage
Table of contentsYour personal guide to Managing Dry Seal ChestDrainage is a quick and easy reference to help extendyour understanding of dry seal chest tube drainage andto help answer questions which may come up fromtime to time. It is provided as an educational serviceby Maquet. This booklet has been prepared as aneducational aid only and is not intended to replace anymedical or nursing practices or hospital policies. Dueto numerous model types available, it is important tocarefully read and follow each corresponding productinsert prior to use.IntroductionMaking it simple to understand. . . . . . . . . . . . . . . . .4How dry seal chest drains functionThe basic operating system. . . . . . . . . . . . . . . . . . . .Fluid collection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dry seal valve and air leak monitor . . . . . . . . . . . . . .Dry suction control. . . . . . . . . . . . . . . . . . . . . . . . . . .5667The Maquet systemAll the water you need.and less! . . . . . . . . . . . . . . . 8Features, benefits, functions . . . . . . . . . . . . . . . . . . 10Product feature summary. . . . . . . . . . . . . . . . . . . . . 12System set upOpen package. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Requirements for set up. . . . . . . . . . . . . . . . . . . . . . 14Four step set up. . . . . . . . . . . . . . . . . . . . . . . . . . . . 14What to check during system operationVerifying suction operation. . . . . . . . . . . . . . . . . . . . 18Increase vacuum source when bellowsis not expanded to s mark . . . . . . . . . . . . . . . . . 182
Changing suction pressure . . . . . . . . . . . . . . . . . . . 19Recording drainage volume . . . . . . . . . . . . . . . . . . 19Placement of unit. . . . . . . . . . . . . . . . . . . . . . . . . . . 19Verifying air leak monitor operation. . . . . . . . . . . . . 20Observing air leak monitor for patient air leaks. . . . 20Vacuum indicator. . . . . . . . . . . . . . . . . . . . . . . . . . . 21Graduated air leak monitor . . . . . . . . . . . . . . . . . . . . 21Sampling patient drainage. . . . . . . . . . . . . . . . . . . . 21In-line patient tube connector . . . . . . . . . . . . . . . . . 21Positive pressure protection . . . . . . . . . . . . . . . . . . 22Swing out floor stand. . . . . . . . . . . . . . . . . . . . . . . . 22Multi-position hangers. . . . . . . . . . . . . . . . . . . . . . . 22Manual high negativity vent. . . . . . . . . . . . . . . . . . . 22Patient tube clamp. . . . . . . . . . . . . . . . . . . . . . . . . . 23Gravity drainage. . . . . . . . . . . . . . . . . . . . . . . . . . . . 23System disconnection . . . . . . . . . . . . . . . . . . . . . . . 23Anatomy and physiology reviewAnatomy of the chest. . . . . . . . . . . . . . . . . . . . . . . . 24Why the lungs are expanded. . . . . . . . . . . . . . . . . . 25The mechanics of breathing. . . . . . . . . . . . . . . . . . . 26Why dry seal chest drains are usedClinical needs for chest tube drainage. . . . . . . . . . . 27What to check for during drain use. . . . . . . . . . . . 30Chest tube placementChest tube insertion. . . . . . . . . . . . . . . . . . . . . . . . . 31Chest tube nursing responsibilities . . . . . . . . . . . . . 32Troubleshooting guideQuestions and answers. . . . . . . . . . . . . . . . . . . . . . 333
IntroductionMaking it simple to understandThe purpose of any chest drainage device is to helpre-establish normal vacuum pressures by removing airand fluid in a closed, one-way fashion.The need for chest drainage is also required followingopen heart surgery and chest trauma to evacuate anypooling blood which, if left in the mediastinal cavity,can cause cardiac distress or tamponade. Hence, chestdrainage is indeed a life-saving procedure and oneof the most important services a physician and nurseclinician can render.While the practical application of dry seal chestdrainage techniques are relatively simple, sometimesthe chest drain and its accompanying terminology mayappear complex. However, dry seal chest drainagesystems are actually quite simple to manage andeasy to understand. It is our hope that a review of theeducational aid booklet will help enhance your workingknowledge of chest drainage and further familiarize youwith Maquet’s easy-to-use dry seal operating system.Customer serviceIf a question or need arises for customer service, productinformation, or to request inservice educational material,we invite you to call anytime.In the U.S.A. 1-800-528-7486Outside the U.S.A. 603-880-1433FAX 603-880-6718www.maquet.comFor additional information about Atriumproducts refer to www.atriummed.com4
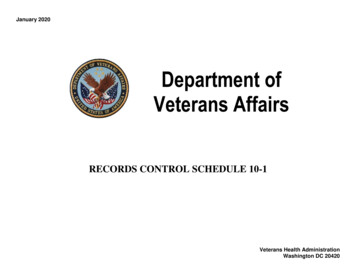
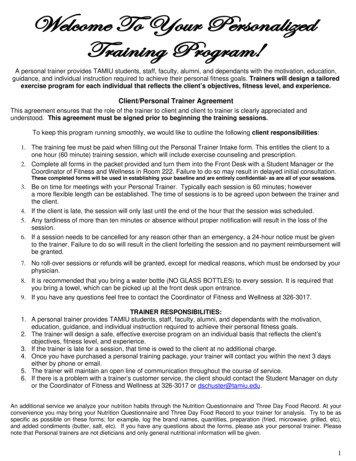
How dry seal chest drainsfunctionThe basic operating systemToday’s dry seal drainage systems are comprised of aone-piece, 3-chamber setup, which separates thefunctions of fluid collection, dry seal (which serves asa one-way valve), and suction control. Unlike Atrium’sOcean and Oasis series chest drains that utilize atraditional water seal for one-way seal protection,the Express features a dry seal valve as its seal. Thismechanical one-way valve allows air to escape from thechest and prevents air from going back to the chest. Theadvantage of a dry seal valve is it does not require waterto operate and it is not position sensitive like a waterseal. On the other hand, a mechanical dry seal valve doesnot provide the same level of patient assessment as atraditional calibrated water seal. Dry seal drains must relyon other means to provide information such as a separateFEABDA Dry suction controlB Vacuum indicatorC Air leak monitorD Collection chamberE Tube to suctionCF Tube from patient5
air leak monitor for optional air leak detection and avacuum indicator to determine when vacuum is presentin the collection chamber.Over the past several years, advances in engineeringhave enabled dry suction technology to beincorporated into familiar chest drain operatingsystems. Consequently, today’s dry seal operatingsystems not only provide a simple and convenientmethod to maintain a required amount of vacuumin a patient’s chest, but provide faster setup times,quiet operation and the ability to impose higher levelsof controlled suction with the simple turn of the dial.Additionally, these new compact, lightweight chestdrains better address the hospital’s critical need forreduced disposal costs.Fluid collectionIn a dry seal operating system, fluidsdrain from the patient directly into a largecollection chamber via a 6-foot patienttube (3/8" I.D.). As drainage fluids collectin this chamber, the nurse will recordthe amount of fluid that collects on aspecified schedule. Hence, an easy-toread, well calibrated collection chamberis an important feature for any chestdrainage system.Dry seal valve & air leak monitor6The dry seal valve, located inside the chest drain,allows air from the patient (positive pressure) to passthrough the mechanical one-way valve, and preventsair from returning to the patient. A dry seal valve is asimple, cost effective means for protecting the patientbecause it is not position sensitive. That means thepatient is protected at all times even if the drain isknocked over. The air leak monitor (if filled with
pre-packaged sterile water provided)allows for visualization of a patient air leak.When bubbles are observed going fromright to left, this will confirm a patient airleak. Intermittent bubbling will confirm thepresence of an intermittent air leak. Nobubbling will indicate no air leak is present.With the addition of a manual and automatichigh negative pressure release valve, apatient is protected from the dangers ofaccumulating high vacuum pressures orhigh negativity, which can be induced from chest tubestripping or milking. Every Maquet chest drain modelprovides such patient protection both manually andautomatically.Dry suction controlThe addition of suction improves the rateof and flow of drainage, as well as helpsovercome an air leak by improving therate of airflow out of the patient. Today’sadvanced chest drains incorporate drysuction control technology to maintainsafe and effective levels of vacuum tothe patient. Similar to how a traditionalcalibrated water chamber controls suction, Maquet’sdry suction control regulator works by continuouslybalancing the forces of suction and atmosphere.Maquet’s dynamic automatic control valve (ACV),located inside the regulator, continually responds andadjusts to changes in patient air leaks and fluctuationsin suction source vacuum to deliver accurate, reliablesuction to the patient. Suction pressure can be setto any desired pressure between -10 cmH2O and -40cmH2O by adjusting the rotary dry suction control dial.Expansion of the bellows across the suction monitorwindow (E) will readily confirm that suction is operating.7
The Maquet systemAll the water you need.and less!From the beginning, Maquet has pioneered advances inthoracic drainage with chest drains that are user friendlyand cost effective. We’ve continued our commitmentto product innovation with the latest series of AtriumExpress dry seal chest drains, featuring a dry sealoperating system with the enhanced performance andconvenience of dry suction control. Maquet’s family ofdry seal chest drains has been carefully engineered toprovide collection performance and satisfy today’s criticalneed for more cost effective blood management. With pre-packaged water, system setup is fast andconvenient. Dry seal valve protects patient like a water seal. Knock-over nozzles allow fluid levels to be recoveredin the event of a knock-over. Finger-tip suction control dial can be adjusted to anysuction setting between -10 cmH2O and -40 cmH2Ofor a wide range of chest drainage applications. Highly visible suction monitor bellows readilyconfirms suction operation. Large, easy-to-read graphics provide fast, accuratedrainage assessment. Automatic high negativity pressure relief valve activatesto limit system pressure at approximately -50 cmH2O. Blue tint water in air leak monitor (if filled with sterilewater provided) offers enhanced visibility for air leakdetection.8
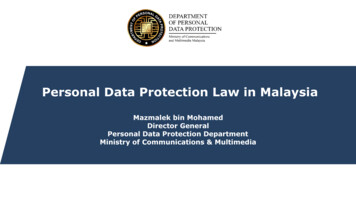
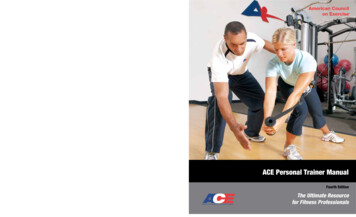
KLFHIGJBADECMNA Dry suction regulatorHSuction portB Vacuum indicatorIFiltered manual highnegativity ventD Collection chamberJMulti-position hangersE Suction monitor bellowsKIn-line connectorF Easy-to-grip handleLNeedleless access portG Positive pressurerelease valveMPatient pressure float ballNSwing out floor standC Air leak monitor9
Maquet’s dry suction control regulator providesaccurate, dependable suction for a wide range of chestdrainage applications. The regulator design continuallyand automatically adjustsDial up toto changes in patient airincreaseleaks and/or fluctuationssuctionin hospital wall suctionDial downto lowerto help maintain a moresuctionconsistent vacuum levelto the patient. Suctionpressure can be set toany desired pressure levelbetween -10 cmH2O andup to a maximum of -40 cmH2O. Changing the suctionpressure is accomplished by adjusting the rotary drysuction control dial located on the side of the drain.Dial down to lower the suction setting and dial up toincrease the suction pressure setting.Suction monitor bellowsMaquet’s suction monitorbellows allows easyconfirmation of vacuumoperation. Expansion of thebellows across the suctionmonitor window will confirmsuction operation.Bellows expanded to s mark or beyondconfirms adequate suction operation.Air leak monitor technologyAt the heart of every Atrium Express dry sealchest drain is an advanced air leak monitor design.Patient air leak assessment and system integrity areenhanced with Maquet’s blue tint water and knock-overprotection. Together with our automatic high negativepressure relief and an easy-to-use filtered manual10
vent, patients have protection from accumulating highnegative pressure.Vacuum indicatorWhen vacuumis present inthe collectionchamber, asymbol willremain visibleVacuum is present Vacuum is not presentin the vacuumindicatorwindow. When vacuum is not present (atmosphericpressure) no symbol will appear. All patient tubeconnections and the vacuum indicator window shouldbe checked regularly for vacuum confirmation.Automatic high negativity reliefDuring prolonged episodes of extreme negativepressure (as with chest tube stripping), Maquet’scontrolled release system will automatically relieveexcessive high negative pressure to a lower level(release set at approximately -50 cmH2O).System disconnection and optionsfor autotransfusionAll models are equippedwith in-line connectors.Maquet offers flexibilityfor prescribing post-opautotransfusion at anytime. These locking patienttube connectors providefor disconnection after useor rapid in-line ATS bloodbag attachment, whenrequired.11
Maquet product feature est draindesignEasy to store,handle, andtransport. Lesspackaging.Environmentally responsible.Less waste is more costsavings for the hospital.Adjustabledry suctioncontrolContinuallyand automatically adjuststo changes inpatient air leaksand/or fluctuations in hospitalwall suction.Regulator dial can be setto any desired suctionpressure between -10 cmH2Oand -40 cmH2O. Providesaccurate, reliable suctioncontrol for a wide range ofchest drainage applications.SuctionmonitorbellowsEasy confirmation of suctionoperation.Large, bright colored bellowsexpands across suction monitor window whensuction is operating.*PrepackagedwaterOnly the air leakmonitor needsto be filled.No more overfilled orunderfilled air leak monitors.The ultimate in time andcost savings.Blue tint airleak monitorEfficient air leakdetection.Air leak monitor turns bluewhen filled.Graduatedair leakmonitorFast, easydetection andmonitoringof patient airleaks.Air leak bubbling can rangefrom 1 (low) to 5 (high) formonitoring patient air leaktrends.Filteredmanual ventEasy-to-use tolower the watercolumnProvides effective manual ventcontrol when lowering height ofair leak monitor.HighnegativepressureprotectionAdvanced valveautomaticallyvents highvacuum.Valve design offers a controlledrelease during episodes ofprolonged high negativepressure (set at approximately-50 cmH2O).VacuumindicatorQuick and easyconfirmationof vacuumwhen presentin collectionchamber.symbol remainingvisible in the vacuumindicator window confirmsvacuum. No symbolindicates no vacuum.*patented12
mper resistantpositive pressurerelief valve automatically filter protection patient fromaccumulating positivepressure.Integral to the system,this valve automatically prevents tensionpneumothorax duringaccidental suction lineocclusion.Autotransfusion CapabilitiesMaquet providesnumerous options foremergency or postop autotransfusionon demand.Fast, convenient ATS baguse or continuous ATSvia infusion pump.In-lineconnectorSmooth, low-profiledesign has audiblelocking mechanism.Connector providessystem disconnectionor fast in-line ATS bagattachment.CollectionchambergraduationsImproved collectionchamber design iseasy to read.Large collection windowgraduations provide fastand accurate volumeassessment.Maximumknock-overprotectionDry seal offerspatient protection.Dry seal integrity ispreserved duringtransport andaccidental knock-over.Knock-overnozzlesAllows fluid volumesto be fully recoveredwhen drain is returned to the uprightposition.Reduces the incidenceof interchamber spills.Easy-to-griphandleComfortable designfacilitates hand-off.Makes patientambulation and patienttransport easy.FlexihangersAccommodatestoday’s newer beddesigns.Flexible hangers(located inside thehandle) allow drain to behung from a single point.Swing outfloor standSecure systemplacement during setup or on floor.Floor stand swings outfor maximum stability,closes for transport.NeedlelessaccesssamplingportIn-line fluid removal.No needle necessary.Connects to anystandard luer-locksyringe.13
System set upOpen packageRemove non-sterile outer protective bag. Maquet chestdrains are wrapped in CSR wrap and should be openedfollowing hospital approved sterile technique.Requirements for set up30 ml of water will be required. Follow hospital’s protocolfor type of water to be used. Sterile saline should be usedfor ATS applications.Four step set upSwing floor stand open for set up. For models equippedwith an in-line connector, move the patient tube clampcloser to the chest drain (next to the in-line connector)for set up convenience and patient safety. Follow steps1-4 and refer to each model’s operating instructions foradditional details concerning system set up, operation,indications for use, and warnings and cautions.14
Step 1Connect chest drain to patientRemove patient tube connector cap and insert steppedpatient connector into patient’s catheter(s). Remove orcut off stepped connector for “Y” connector insertion.If desired, use of nylon bands around catheter andpatient tube connections will assure an air-tightconnection. Connect chest drain to patient prior toinitiating suction.Indwelling chest tubeStep 2Connect chest drain to suctionAttach suction line to suction port on top of chest drain.Suction sourceThe suction source should provide a minimum vacuumpressure of -80 mmHg at 20 liters of air flow per minutefor chest drain operating efficiency at a suction controlsetting of -20 cmH2O. The suction source vacuumshould be greater than -80 mmHg when multiple chestdrains are connected to a single suction source.15
Step 3Turn suction source OnIncrease suction source vacuum to -80 mmHg orhigher. The suction monitor bellows must be expandedto the s mark or beyond for a -20 cmH2O or higherregulator setting. The regulator control dial, located onthe side of the drain, can be adjusted to any suctionsetting between -10 cmH2O and -40 cmH2O. Dial downto lower the suction setting and dial up to increase.Suction monitor bellowsWhen the suction control regulator is set at -20 cmH2Oor higher, the bellows must be expanded to the s markor beyond when suction is operating. If the bellows isobserved to be expanded, but less than the s mark,the suction source vacuum pressure must be increasedto -80 mmHg or higher. For a regulator setting lessthan -20 cmH2O suction (-10 cmH2O), any observedbellows expansion across the monitor window willconfirm suction operation. The bellows need not beexpanded to the s mark for pressures less than -20cmH2O, just visibly expanded to confirm suctionoperation.Turn suction source to -80 mmHg orhigher. Bellows must be expanded tos mark or beyond for -20 cmH2O orhigher regulator setting.16
Step 4Fill air leak monitorto fill lineFill air leak monitor to the fill line by syringe (no needle)with 30 ml of sterile water or sterile saline via theneedleless injection port located on the back of thedrain. For models available with sterile fluid, twist topoff syringe and insert tip into needleless luer port.Depress syringe plunger into luer port and squeezecontents into air leak monitor until fluid reaches fill line.H 2OOnce filled, water becomes tinted blue for visibilityof air leaks.17
What to check duringsystem operationVerifying suction operation via the suctionmonitor bellowsThe bellows locatedin the suction monitorwill expand only whensuction is operating.The monitor bellowswill not expand whensuction is not operatingor disconnected. Thecalibrated s mark allowsBellows must be expanded to sconfirmation of vacuummark or beyond for a -20 cmH2Ooperation over a wideor higher regulator setting.range of adjustable suctioncontrol settings.Increase vacuum source when bellows is notexpanded to s markIf the bellows is observed to be expanded, but lessthan the s mark, the vacuum source pressure must beincreased to -80 mmHg or higher.Not enoughvacuum for-20 cmH2O orhigher suctioncontrol setting.18Normal suctionoperation for-20 cmH2O orhigher.Increase suctionsource to -80 mmHgor higher.
Changing suction pressureChanging suction pressure is accomplished byadjusting the rotary dry suction control dial locatedon the side of the drain. Dial down to lower suctionpressure and dial up to increase suction pressure.NOTE: When changing suction pressure from a higherto lower level, use of the manual high negativity ventafter regulator adjustment will reduce excess vacuumdown to the lower prescribed level.Recording drainage volumeThe collection chamber incorporates a writing surfacewith easy-to-read fluid level graduations. Please referto individual product for specific graduation.Placement of unitFor optimum drainage results, always place chest drainbelow the level of the patient’s chest in an uprightposition. To avoid accidental knock-over, it isrecommended to swing the floor stand open for secureplacement on floor or to hang the system bedside withthe hangers provided.19
Verifying air leak monitor operationThe air leak monitor can be filled and maintained atthe fill line to ensure proper operation and should bechecked regularly when used for extended periods.As required, additional water may be added by syringevia the luer port located on the back. Fill to the fill line.Observing air leak monitor for patient air leaksAtrium Express chest drains offer air leak detectionwith rapid air leak assessment and improved visibilitydue to the tinted water. A patient air leak is confirmedwhen air bubbles are observed going from right to leftin the air leak monitor.Continuous bubbling in the bottom of the air leakmonitor will confirm a persistent air leak.Intermittent bubbling with float ball oscillation willconfirm the presence of an intermittent air leak.No bubbling with minimal float ball oscillation at thebottom of the air leak monitor will indicate no air leakis present.20
Vacuum indicatorWhen vacuum is present in the collection chamber,asymbol will remain visible in the vacuum indicatorwindow. When vacuum is not present (atmosphericpressure) no symbol will appear. All patient tubeconnections and the vacuum indicator window shouldbe checked regularly for vacuum confirmation.Graduated air leak monitorAir leak bubbling can range from 1 (low) to 5 (high).Air bubbles create an easy to follow air leak patternfor monitoring patient air leak trends.Sampling patient drainageSampling of patient drainage must be in accordancewith approved hospital infection control standards.Selected models include a needleless luer port on thepatient tube connector for sampling patient drainage.Alcohol swab the luer port prior to syringe attachment(no needle). Fluid samples can also be taken directlyfrom the patient tube by forming a temporarydependent loop and inserting a 20 gauge needle at anoblique angle. Alcohol swab the patient tube prior toinserting syringe at a shallow angle. Do not puncturepatient tube with an 18 gauge or larger needle.In-line patient tube connectorThe locking in-line patienttube connector providessystem replacement, simpledisconnection after use, andrapid in-line ATS blood bagattachment when required.The in-line connector mustremain securely connectedat all times during operation and patient connection.Do not separate in-line connector prior to clampingoff patient tube clamp.21
Positive pressure protectionMaquet’s positive pressurerelease valve, located on top ofdrain, opens instantly to releaseaccumulated positive pressure.Integral to the system, this valvedesign is tamper-resistant. Donot obstruct the positive pressure valve.Swing out floor standMaquet’s floor stand swings open for convenientsystem set up and secure placement on floor. It isrecommended that the floor stand be closed duringpatient transit or when unit is hung on bed.Multi-position hangersThe multi-position hangersare easily lifted from insidethe handle. Press hangersinto handle when not inuse. The flexible hangersallow the drain to be hungbedside from a single point.Lift tousePushin tolockManual high negativity ventTo manually lower theheight of the watercolumn or to lowerpatient pressure whenconnected to suction,temporarily depressthe filtered manual vent Do not use when suction is notoperating.located on top of thedrain until the watercolumn lowers to the desired level. Do not use manualvent to lower water column when suction is notoperating or when the patient is on gravity drainage.22
Patient tube clampThe removable patient tube slide clamp provided within-line connector models must remain open at all timesduring system operation. It is recommended to movethe patient tube clamp next to the in-line connector(closer to the chest drain) for set up convenience androutine visual check. Do not keep patient tube clampclosed when system is connected to patient. Tubeclamp must be closed prior to in-line connectorseparation.Move clampcloser to drain,next to in-lineconnectorCAUTION:Keep clampopen at alltimes whensystem isconnected topatientGravity drainageFor gravity drainage applications, the drain should beplaced below the patient’s chest in an upright position.Disconnect the suction source vacuum line from thesuction line port.System disconnectionFor models equipped with an in-line connector, closethe patient tube slide clamp prior to disconnectingthe chest drain patient tube from patient. Clamp offall indwelling thoracic catheters prior to disconnectingchest drain from patient.23
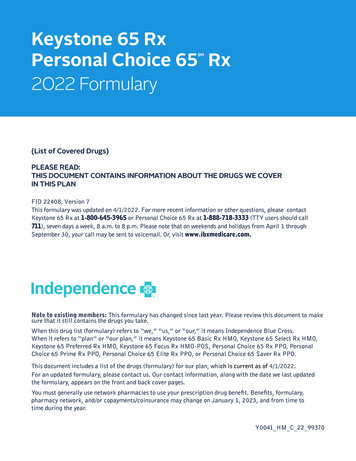
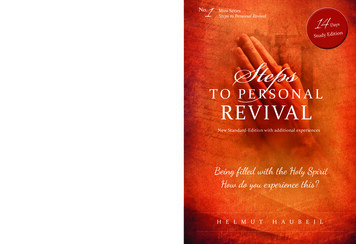
Anatomy and physiologyreviewAnatomy of the chestThe chest wall is composed of the ribs, sternum, andthoracic vertebrae and are all interlaced and covered withintercostal muscle to form a semi-rigid structure. Thelower boundary or floor of the thoracic cavity is known asthe diaphragm, which is also composed of muscle.Although the thoracic cavity contains two passagewayswhich are open to the outside environment, theesophagus and trachea, the cavity itself is an enclosedstructure. The interior of the thoracic cavity can bedivided into three distinct areas: the mediastinum andtwo separate chambers for each lung. The superiormediastinum consists of soft tissue which enclosesthe esophagus, trachea, heart, aorta, and other majorvessels. The mediastinum acts as a flexible partitionwhich extends from the front-to-back and top-tobottom of the central portion of the chest.The inside of the rib cage is lined by a membranecalled the parietal pleura while the lungs are coveredby another membrane called the pulmonary or visceralChest wallRightlung cavity24Left lungcavityDiaphragmMediastinalcavity
pleura. Under normal conditions, these two pleuralsurfaces slide against each other allowing the lungs toexpand and contract. These two surfaces are closelyheld to one another, being separated only by a verythin film of lubricating fluid secreted by the pleura,called pleural fluid.Why the lungs are expandedA principal factor which keeps the visceral and parietalpleurae together and not separating is vacuum,commonly referred to as negative pressure. Thisnegative pressure, or vacuum, is present during normalrespiration with the membranes closely intact undernormal conditions. The presence of negative pressurebetween these two membranes is what helps holdthe visceral pleura in close contact with the parietalpleura at all times. Hence, negative pressure or vacuumaround the outside of the elastic lung is what keepsthe lung in a fully expanded position, counteracting thelung’s normal tendency to shrink in size.ParietalpleuraPleuralspaceVisceralpleuraIf air, fluid, or blood were to enter the space betweenthese two membranes, the space created is known asa pleural space and is an abnormal occurrence. Whenthis occurs, the lungs can no longer fully expand witheach inspiration and intense pain results, inhibiting thevoluntary effort of breathing.25
The mechanics of breathingRespiration is the cycle of inspiration and expiration inwhich air moves in and out of the lungs due to changesin pressure. When the diaphragm is stimulated bythe phrenic nerve, it contracts and moves downward.With the help of the external intercostal muscles, therib cage moves up and out. The lung itself expandsbecause of the movement of the diaphragm and thechest wall. The surface tension of the pleural fluidtogether with the naturally occurring vacuum pressureinduced by the pulling action of the diaphragm is whatactually holds the pleural membranes together, thuskeeping the lungs fully expanded.Under normal conditions,there is always negativepressure in the pleuralcavity. The degree ofnegativity, however,changes duringrespiration. Duringnormal inspiration,intrapleural vacuumpressure is approximately -8 cmH2O,while during expirationthe vacuum pressurefalls to -4 cmH2O.With deep inspiration,intrapleural pressurescan be even morenegative.26Inspiration-8 cmH2OExpiration-4 cmH2O
Why dry seal chest drainsare usedClinical needs for chest tube drainageWhen the chest wall is opened either by surgery orchest injury, the in-rush of air causes the vacuum inthe patient’s pleural cavity to escape and atmosphericair to enter the intrapleural space. Since the normalnegative pressure or vacuum is no longer present, thelungs collapse as they depend upon this negativity orvacuum to stay fully expanded up against the insideof the chest wall. When air enters or becomes trappedinside the chest causing a pleural space, the lungscannot fully expand, and the patient will experiencedifficulty in breathing. This condition is known as apneumothorax. This is a frequent occurrence after allthoracic and cardiac surgeries, as well as with mostchest wall injuries. Often there is a combination of bothair and blood present in this abnormal space, causing asimilar effect on breathing. When blood collects in thepatient’s pleural space, it is known as a hemothoraxand when there is the combination of both blood andair, it is known as a hemopneumothorax.PneumothoraxHemopneumothorax27
Tension pneumothorax is a more serious complicationthat can develop when air continues to leak from ahole in the lung directly into the pleural space and hasno way to escape. As more and more
traditional water seal for one-way seal protection, the Express features a dry seal valve as its seal. This mechanical one-way valve allows air to escape from the chest and prevents air from going back to the chest. The advantage of a dry seal valve is it does not require water to operate and it is n