Transcription
Aberrant Root Canal Anatomy: A ReviewABERRANT ROOT CANAL ANATOMY: A REVIEWDr. Sasidhar NallapatiSuccessful endodontic treatment involves accuratediagnosis, good understanding of the biologicalprinciples and excellent execution of the treatment. Tobe able to execute an excellent treatment, it’s imperativethat the clinician has comprehensive knowledge of theroot canal anatomy and the know-how to locate andtreat this anatomy.B.D.S.Type II: Two canals that merge into one and exit asone canal (2-1)Type III: One canal that divides into two and exit astwo canals. (2-2)Vertucci’s classification was more elaborate and itcovered 8 types.Many outcome studies conducted over the past fewdecades showed incomplete debridement anddisinfection of root canal space as the most importantfactor in endodontic treatment failure (1,2,3). Missedcanal in the initial treatment as a significant cause ofroot canal failure was shown by Hoen et al (4). Theyalso showed a significant relation between anasymmetrical obturation in a root space and theincidence of a missed canal in an initial treatment.Type IType IIType IIIType IVType VType VIType VIIType VIII1-12-11-2 -12-21-22-1-21-2-1-23-3Methodology:Studies with Percentages:Root canal anatomy is studied by both in vitro and invivo methods. In vivo methods include clinical treatmentof a tooth followed by radiographic evaluation of theroot canal anatomy. In vitro methods includeThe methodology employed and the criteria used todescribe root canal anatomy will decide the percentagesof canals found in any tooth. For example Neaverth etal (5) have used “two separate canals could bevisualized on radiographic examination (two files or twoGP points to no less than a mm short of the length)” asthe criteria for two canals in a mesiobuccal root of amaxillary first molar. On the other hand Sempira et al(6) have used the presence of “two canals to at least 4mm from the apex” in the mesiobuccal root of maxillaryfirst molar to determine the percentage of Mb2 canal.These differences in criteria dictate the great variationseen in the percentages of root canals seen in differentstudies. However, if one reviews the published evidencecertain features of aberrant anatomy stand out in a tooth/root.1.2.3.4.5.6.7.8.9.10.Direct observationMicroscopic observationMacroscopic sectioningMicroscopic sectioningDyesFilling and decalcificationFilling and clearingRadiographyContrasting media (Hypaque)Cone beam Tomography.Ethnicity has a significant influence on aberrantanatomy,(26). Radix Entomolaris, an extra distal root ina mandibular molar, is often seen in Oriental and Eskimopopulations (23). Similarly 2 and 3 canal premolars areseen frequently in black populations (12,15,27).‘C’shaped anatomy is seen more commonly in Chinese,Korean and Indian populations (22,25).Classification:Weine classified root canal anatomy into 3 types.Type I:One canal with one orifice and one apicalforamen (1-1)Bilateral symmetry is a feature of aberrant anatomy.Rarer the aberration, the more common is the bilateralsymmetry (28).Dr. Sashi Nallapati obtained his dentaldegree from the Govt. Dental College andHospital, Hyderabad, India. He completedhis post graduate training in the specialtyof Endodontics from Nova SoutheasternUniversity (NSU), Davie, Florida, USA.He maintains a practice limited toEndodontics in Kingston, Jamaica. He serves on thefaculty of NSU in the dept. of Post Graduate Endodontics.Dr. Nallapati authored several clinical articles and lecturesacross the globe. His hobbies include digital photography,swimming and reading. he can be reached atwww.endojamaica.comClinical Management of Aberrant Anatomy:Radiography: Angled views of teeth reveal aberrantanatomy. Angled views allow us to visualize the rootanatomy in 3 dimensions so that better assessment ofthe root canal anatomy is made. It is imperative that atleast 2 angled views shall be taken before attemptingendodontic treatment.5050 - 62 Sasidhar Nallapati.pmd5012/5/2007, 12:50 PM
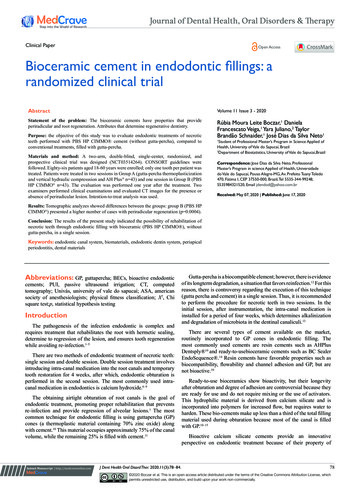
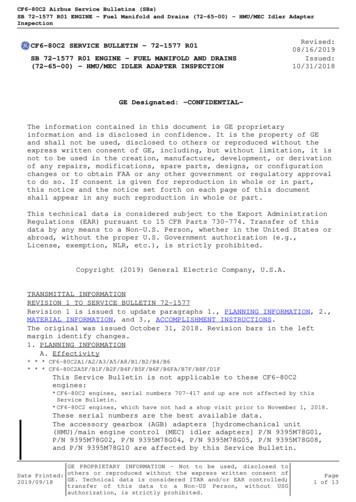
Aberrant Root Canal Anatomy: A ReviewToothFeatureMaxillary Central IncisorOver 60% lateral canals (7)Maxillary Lateral IncisorLingual curvatureLarge mid root canal diameterMaxillary CanineSingle canal (9)Lateral canalsMaxillary First PremolarThree canals with two canals in the buccal root (mesiobuccal, distobuccaland palatal canals) (11,12)Maxillary Second PremolarThree canals with two canals in the buccal root(mesiobuccal and distobuccaland palatal canals) (12)Maxillary First MolarTwo mesiobuccal canals in majority of cases. Occasionally three mesiobuccalcanals, two distobucal and two palatal canals (16,17,18,19)Maxillary Second MolarTwo mesiobuccal canals in majority of the cases. ‘C’ shaped canals (30)MandibularIncisorsTwo canals that join apically. Occasionally 2 separate canals (8)Mandibular CanineTwo canals. Buccal and lingual (9)Mandibular First PremolarTwo to three canals. Mesiobuccal, distobuccal and lingual.‘C’ shaped anatomyoccasionally (10,13,15)Mandibular Second PremolarTwo to three canals. Mesiobuccal, distobuccal and lingual.‘C’ shaped anatomyoccasionally (14,15)Mandibular First MolarFour to six canals. Three mesial canals and three distal canals. Radixentomolaris with a separate distolingual root (20,21,23,24)MandibularSecond MolarFour to five canals. Three mesial canals. ‘C’ shaped anatomy(22,25)Once a canal disappears mid-root, one shall alwayssuspect a bifurcation. Twin periodontal ligament outlinesof the root also indicate a broad root and therefore extraanatomy. Guide files are placed in root canals andradiographs are taken to reveal the symmetry of theguide file to the external contours of the root. If there isan asymmetry, it often means hidden anatomy. Alsoguide files reveal any hidden curvatures that are inmultiple planes. (Fig 1-3)Clinical Anatomy: Contour of the gingiva oftenindicates aberrant anatomy. For example, broad buccalgingiva in a maxillary or mandibular premolar maysuggest a broad buccal root. This in turn may suggestFigure 2: Distobuccal canal located.Figure 1: Off-centre appearance of guide file in thebuccal and palatal roots of maxillary premolar.Figure 3: All three canals obturated.5150 - 62 Sasidhar Nallapati.pmd5112/5/2007, 12:50 PM
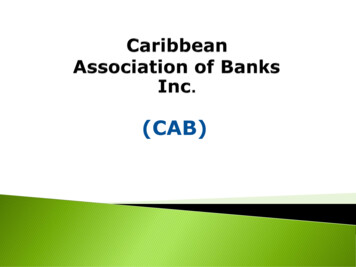
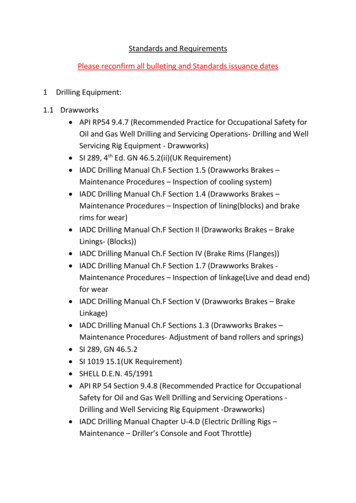
Aberrant Root Canal Anatomy: A ReviewMb2 in a maxillary molar, Middle mesial canal in themesial root of a mandibular molar, second buccal canalin a maxillary premolar and the radix entomolaris in amandibular molar. Initial access shape is determinedby the shape of the pulpal floor (32). Then, appropriateextensions are made to facilitate the location andstraight line access into all canals. Complete unroofingof the chamber roof is a basic step in access designand yet many clinicians err by not removing the roof ofthe chamber (fig10a,10b).the presence of two canals in the buccal root. Gingivalrecession some times may reveal a bifurcation of thebuccal root indicating two canals in maxillary andmandibular premolar teeth (fig 4). Teeth that have anextra cusp or an aberrant clinical crown may indicateaberrant pulp chamber and root canal anatomy (fig 58).Magnification: A surgical operating microscope (S.O.M)(www.globalsurgical.com) is highly recommended toperform all endodontic therapy (fig 9). An S.O.M notonly magnifies the chamber anatomy in great detail butalso allows great amount of light to illuminate the pulpchamber. This allows the operator to understand thesubtleties of pulp chamber anatomy, visualize the pulpalfloor and locate root canal orifices. This becomes evenmore useful when there are pulpal floor calcificationsblocking canal orifices (31). Significant amount ofpreparation of the pulpal floor is required to identify andcarve calcifications away to locate root canal orifices.The use of an SOM greatly facilitates this process andmakes endodontic therapy more predictable and lessstressful to the operator.Size and extension of access plays an important rolein the predictable location of all root canals. Modifiedaccess extensions are required to identify canals likeFigure 6: Access reveals two palatal canals andone mb canal that bifurcated.Figure 4: Gingival recession allows to see the bifurcationof the buccal root in a mandibular premolar.Figure 7: Preoperative radiograph of the molar.Figure 5: Extra cusp on the distal in a maxillary second molar.Figure 8: Post-operative radiograph of the molar.5250 - 62 Sasidhar Nallapati.pmd5212/5/2007, 12:50 PM
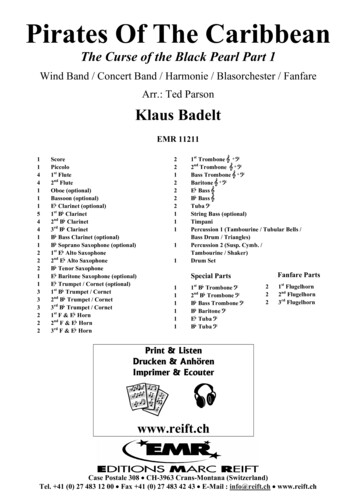
Aberrant Root Canal Anatomy: A ReviewSubtle color changes are observed between the coronaldentin and the pulpal floor dentin under the SOM. Thisis useful in the location of the pulp chamber and canalorifices. Pulpal floor is usually is dark gray in color andcontrasts from the light colored axial dentin. Whenaccess preparations are made this color differenceallows the operator to be very precise in removing theaxial dentin to expose the pulpal floor. There is also avery subtle difference in color between tertiary dentinand axial dentin. This difference allows the operator tobe once again very precise in carving away thisirritational dentin to expose the pulpal floor andsubsequently canal orifices.Figure 9: Surgical operating microscope.Isthmus: It is the space that connects two or morecanals that exist in the same root (29). Isthmus is thefrequent location of an aberrant canal (fig 11a-b).Isthmus houses pulp tissue (12a-c). If the isthmus existsonly in the coronal third, it should be eliminated toremove the pulp tissue. If the isthmus extends from thecoronal to the middle/apical third, it should beFigure 10a: Roof of the chamber not unroofedin the original treatment.Figure 11a: Isthmus explored between Mb andML canals in a mandibular molar.Figure 10b: Complete removal of the roof reveals asecond distal canal in a mandibular molar.Pulpal Floor: When access preparations are made,coronal dentin is removed to make entry into the pulpchamber space. Often times the pulp chamber spaceis reduced in size or completely filled with eithersecondary dentin or tertiary dentin.Figure 11b: Three mesial canals and two distal canals.5350 - 62 Sasidhar Nallapati.pmd5312/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A ReviewUltrasonics (www.eie2.com) (fig 14-16)CKT D1CKT D2Ball tipThe idea is to use a flat/round ended bur/ ultrasonic tipto trough the surface to remove the calcifications. Muncediscovery burs are used in a low speed hand piece.They offer a significant advantage over the other bursbeing long, stiff and a thin shank. This allows betterFigure 12a: Isthmus between the DB and DL canalsin a mandibular molar housing tissue.Figure 13: Munce discovery burs.Figure 12b: Ophthalmic dye stains the tissue.Figure 14: CKT1D ultrasonic tip.Figure 12c: Tissue removed.considered as a separate canal and cleaned, shapedand obturated like any other canal.Some of the instruments used for the purpose of carvingthe pulpal floor calcifications and troughing an isthmusare the following.Burs¼,1/2, #1, #2 Round bursLN BursComposite finishing bursMunce discovery burs(www.cjmengineering.com) (fig 13)Figure 15: Ball shaped tip.5450 - 62 Sasidhar Nallapati.pmd5412/5/2007, 12:50 PM
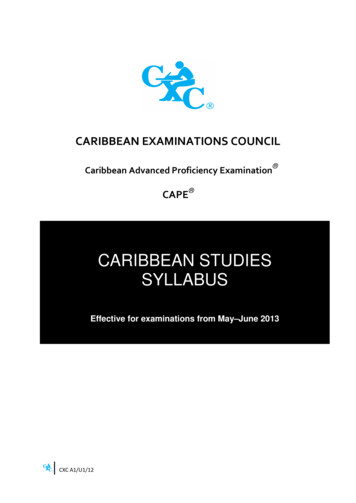
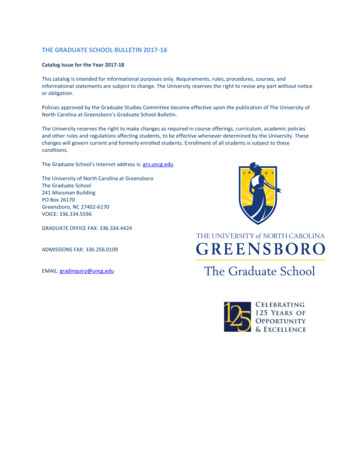
Aberrant Root Canal Anatomy: A ReviewFigure 17a: Initial access in a maxillary molarrevealing four canals.Figure 16: CKT 2D ultrasonic tip.visualization when working deep in the chamber or root.Some of the limitations of this series of burs are inposterior teeth in patients with limited mouth opening.CKT series ultrasonic tips from Eie2 are excellent forboth chamber and deep root troughing. They areespecially useful in posterior teeth and in patients withlimited mouth opening.Canal Relocation:All canals in multirooted teeth, exit the pulp chamber atan angle. Once a canal is located, this exit curvatureshall be minimized or eliminated. This will create astraight line access to the mid root (fig 17a-b). This inturn facilitates negotiation of the canal to the apex. Thefollowing instruments can be used for this purpose.Burs¼, 1/2, #1, #2 Round bursLN BursComposite finishing bursMunce discovery burs(www.cjmengineering.com)Figure 17b: Final access after the canals are relocated.Similarly, transillumination the pulp chamber with anexternal fiber-optic light source allows differentiation ofsclerotic dentin from normal dentin. This in turn allowsprecise removal of the sclerotic dentin to locate rootcanal orifices (fig 18).Ultrasonics (www.eie2.com)CKT D1CKT D2Ball tipSub chamber bifurcations. In mesial roots ofmandibular second molars, buccal roots of maxillarysecond molars and buccal roots of maxillary premolars,only one canal is seen on making the access. Uponcareful troughing of the canal orifice, this single canalis found dividing into two canals apical to the chamberlevel (fig 19a-b).Gates Glidden drills4, 3, 2 (sizes 90,70,50)Niti filesAccess shapersApical bifurcations on the other hand can be seen inany root of any tooth. Adequate coronal flaring and usingpre-bent hand files in an exploratory fashion to scoutthe walls of the root canal often help in the location ofthe apical bifurcations. Subsequently a straight lineaccess (with in the limits of safety) to the apicalbifurcation will help clean, shape and obturate thesplitting canals (20a-b).Dyes can help locating pulp tissue in pulp chamber.Sable seek (www.ultradent.com), methylene blue(www.vista-dental.com) or fluorescein sodium(www.haag-streit.com) are the appropriate choices (33).Dyes stain any vital or dystrophic pulp tissue in thechamber or root canal space. Under magnification thisstaining guides the operator to the pathway to the pulpcanals.5550 - 62 Sasidhar Nallapati.pmd5512/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A ReviewFigure 18: Transillumination reveals dystrophic calcificationsin the pulp chamber.Figure 19a: Initial access in a mandibular molarreveals only one canal in the mesial root.Figure 19b: Final access reveals two canalsin the mesial root.Figure 20a: Mandibular premolar withfailing root canal treatment.Figure 20b: Apical split located and treated.5650 - 62 Sasidhar Nallapati.pmd5612/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A Review‘C’ shaped canals are frequently seen in mandibularsecond molars and less frequently in maxillary secondmolars and mandibular premolars (fig 21a-c). The canalshape resembles the letter ‘C’. There are three differentvariations to this entity.1.All canals are joined in the ‘C’2.Two canals are joined in the ‘C’ and one canalstays separate.3.All canals stay separate with in the ‘C’molar with the radix shall have three roots with 4 canals,not be confused with a mandibular molar with two rootsand four canals (fig. 23a-d).One of the most difficult aspects of treating this anatomyis the predictable removal of pulp tissue in the isthmusthat connects all canals. Ultrasonic debridement, specialirrigation techniques and intra-canal medicaments havea better chance in debriding and disinfecting thesecanals (fig 22a-b).Radix Entomolaris is separate root that exists usuallyto the distolingual in a mandibular molar. A mandibularFigure 21c: Post op radiograph of the ‘C’ shapedmaxillary molar.Figure 21a: Maxillary molar with a ‘c’ shaped anatomy.Figure 21b: DB and palatal canals are in ‘C’ shape.Notice the two Mb canals.Figure 22a,b: Pre and Post op radiographs of retreatmentof ‘C’ shaped mandibular second molar.5750 - 62 Sasidhar Nallapati.pmd5712/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A ReviewFigure 23a: Radix entomolaris successfullytreated in the mandibular first molar.Figure 24a: Access of radix entomolaris showingthe off centre DL canal.Figure 23b: Mandibular molar with two rootsand four canals.Figure 24b: Access of mandibular molar with two rootsand four canals.in the developmental line connecting the DB1 andpalatal canals. Most times the two canals merge to exitapically as one canal. Occasionally two separate canalsmay be seen (27a-c).Access preparation in a radix shall be different as theorifice to the distolingual root is far more lingual thanthe distolingual canal orifice in a two rooted mandibularmolar (fig 24a-b). Another very important feature of thisroot is the sharp coronal curvature to the lingual andequally abrupt apical curvature to the buccal.Three canal maxillary and mandibular premolars arefar more common than reported in the literature (fig 28ab). When three canals exist in premolars they are usuallytwo in the buccal root and one in the lingual root (29ab). Occasionally the three canals in a mandibularpremolar can exist in a ‘C’ shaped anatomy.Middle mesial canals in the mesial root of mandibularmolars are far more common than reported in theliterature. When they exist they are located in the isthmusconnecting the mesiobuccal and mesiolingual canals.More often than not they join either the mesiobuccal ormesiolingual canals. However, it is not uncommon tosee them exit the root as a separate canal (fig 25a-b).Conclusions:Three mesiobuccal canals in a maxillary molar (Mb1,Mb2, Mb3) is a less frequent phenomenon. Nonethelessthe clinician shall be on the look out for this anatomy.When an Mb3 exists it usually is palatal to the Mb2 (fig26a-d).Aberrant anatomy is far more common in today’sendodontic specialist practice. Clinicians shall beconstantly on the look out for ‘occult’ anatomy assuccessful outcome of any case depends on thecomplete debridement and disinfection of all canals.Thorough knowledge of the root canal anatomy andthe consistent use of Surgical Operating Microscopefacilitate the location and treatment of aberrant anatomy.Two Distobuccal canals in maxillary molars is afrequent phenomenon. Db2 exists palatal to Db1 orifice5850 - 62 Sasidhar Nallapati.pmd5812/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A ReviewFigure 25a: Mandibular molar with three mesial canals.Figure 25b: Middle mesial canal with aseparate portal of exit.abcdFigure 26a-d: Maxillary molar retreatment reveals three Mb canals. All three canals merged apically.5950 - 62 Sasidhar Nallapati.pmd5912/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A ReviewabcdFigure 27a-d: A rare occurrence of two separate Db canals in a maxillary molar. Also notice three Mb canals.baFigure 28a,b: Maxillary first premolar with three canals.6050 - 62 Sasidhar Nallapati.pmd6012/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A Review7.Kasahara E, Yasuda E, Yamamoto A, Anzai M. Rootcanal system of the maxillary central incisor. JEndod. 1990 Apr; 16(4): 158-61.8.Benjamin KA, Dowson J. Incidence of two rootcanals in human mandibular incisor teeth. Oral SurgOral Med Oral Pathol. 1974 Jul; 38(1): 122-69.Vertucci FJ Root canal anatomy of the humanpermanent teeth. Oral Surg Oral Med Oral Pathol.1984 Nov; 58(5): 589-99.10. Vertucci FJ.Root canal morphology of mandibularpremolars J Am Dent Assoc. 1978 Jul; 97(1): 4750.11. Carns, Skidmore, Configurations and deviations ofroot canals of maxillary first premolars. Oral SurgOral Med Oral Pathol. 1973 Dec; 36(6): 880-6.12. Nallapati S, Three canal maxillary premolars: Acommon clinical reality, Endodontic Practice, 2003.13. Barrett MT ,1925 Internal Anatomy of the teeth withspecial reference to the pulp with its branches.Dental Cosmos 67: 581.14. Rodig T, Hulsmann M. Diagnosis and root canaltreatment of a mandibular second premolar withthree root canals Int Endod J. 2003 Dec; 36(12):912-9.15. Nallapati S. Three canal mandibular first and secondpremolars: a treatment approach.J Endod. 2005Jun; 31(6): 474-6.Figure 29a,b: Mandibular premolar with three separate canals.16. Kulild, Peters, Incidence and configuration of canalsystems in the mesiobuccal root of maxillary firstand second molars 1997 Jul; 16(7): 311-7.Keep in mind, no aspect of clinical endodontics is moreimportant in locating aberrant anatomy than the attitudeand desire of the clinician.17. Wolcott, Ishley, Kennedy, Johnson, Minnich, MeyersA 5 Yr Clinical Investigation of Second MesiobuccalCanals in Endodontically Treated and RetreatedMaxillary Molars. Journal of Endodontics. 31(4):262-264, April 2005.Bibliography:1.2.Swartz DB, Skidmore AE, Griffin JA. Twenty yearsof endodontic success and failure. J Endodon 1983;9: 198-20218. Stropko JJ. Canal morphology of maxillary molars:clinical observations of canal configurations. JEndod. 1999 Jun; 25(6): 446-50.Seltzer S, Bender IB, Smith J, Freedman I, NazimovH. Endodontic failures-an analysis based on clinical,roentgenographic, and histologic findings. II. OralSurg Oral Med Oral Pathol. 1967 Apr; 23(4): 51730.19. Christie WH,Peikoff MD,Fogel HM.Maxillary molarswith two palatal roots: a retrospective clinical study.JEndod. 1991 Feb; 17(2): 80-4.3.Vire DE, Failure of endodontically treated teeth:classification and evaluation. JEndod. 1991Jul;17(7): 338-42.20. Al-Nazhan S Incidence of four canals in root-canaltreated mandibular first molars in a Saudi Arabiansub-population. Int Endod J. 1999 Jan; 32(1): 4952.4.Hoen M, Pink, F. Contemporary endodonticretreatments: an analysis based on clinicaltreatment findings.J Endod. 2002 Dec; 28(12): 834621. Pomeranz HH, Eidelman DL, Goldberg MG.Treatment considerations of the middle mesial canalof mandibular first and second molars. J Endod.1981 Dec; 7(12): 565-8.5.Neaverth EJ, Kotler LM, Kaltenbach RF. Clinicalinvestigation (in vivo) of endodontically treatedmaxillary first molars.J Endod.1987 Oct; 13(10):506-1222. Seo MS, Park DS. C-shaped root canals ofmandibular second molars in a Korean population:clinical observation and in vitro analysis. Int EndodJ. 2004 Feb; 37(2): 139-44.6.Sempira HN, Hartwell GR. Frequency of secondmesiobuccal canals in maxillary molars asdetermined by use of an operating microscope: aclinical study. J Endod. 2000 Nov; 26(11): 673-4.23. Demoor, Deroose, Calberson. The radixentomolaris in mandibular first molars: anendodontic challenge. Int Endod J. 2004 Nov;37(11): 789-99.6150 - 62 Sasidhar Nallapati.pmd6112/5/2007, 12:50 PM
Aberrant Root Canal Anatomy: A Review29. Weller NR, Niemczyk SP, Kim S (1995) Incidenceand Position of the canal Isthmus. Par t 1.Mesiobuccal root of the maxillary first molar. Journalof Endodontics.24. Fabra-Campos H.Three canals in the mesial rootof mandibular first permanent molars: a clinicalstudy. Int Endod J. 1989 Jan; 22(1): 39-43.25. Ng YL, Aung TH, Alavi A, Gulabivala K. Root andcanal morphology of Burmese maxillary,mandibular molars. Int Endod J. 2001 Dec; 34(8):620-30.30. Yang ZP, Yang SF, Lee G (1988) The root and rootcanal anatomy of maxillary molars in a Chinesepopulation. Endodontics and Dental Traumatology4, 215-8.26. Chopra P, Bal CS. Study of root canals and theirconfiguration in buccal roots of maxillary firstpermanent molar. Indian J Dent Res. 1989 Jan-Mar;1(1): 3-14.31. Carr GB. Microscopes in endodontics.J Calif DentAssoc. 1992 Nov; 20(11): 55-61.32. Krasner P, Rankow HJ. Anatomy of the pulpchamber floor. J Endod. 2004 Jan; 30(1): 5-16.27. Trope M, Elfenbein L, Tronstad L. Mandibularpremolars with more than one root canal in differentrace groups J Endod. 1986 Aug; 12(8): 343-5.33. Nallapati S, Glassman G. Use of ophthalmic dye inroot canal location, Endodontic practice 2004.28. Sabala CL,Benenati FW,Neas BR. Bilateral root orroot canal aberrations in a dental school patientpopulation. J Endod. 1994 Jan; 20(1): 38-42.6250 - 62 Sasidhar Nallapati.pmd6212/5/2007, 12:50 PM
maxillary first molar. On the other hand Sempira et al (6) have used the presence of “two canals to at least 4 mm from the apex” in the mesiobuccal root of maxillary first molar to determine the percentage of Mb2 canal. These differences in criteria dictate the great variation seen in