Transcription
IMMEDIATELIFE SUPPORTPRE-COURSEHANDBOOKIn accordance with the Resuscitation Guidelines, 2015Sarah HopeProduced by ECG Ltd, December2019
ContentsIntroduction . 3Non-Technical Skills . 3Leadership. 3Teamwork . 4Situational Awareness . 4Communication Skills . 4Debrief . 5Reporting Incidents . 5Signs of Deterioration . 6Chain of Prevention . 6National Early Warning Score . 7Causes of patient deterioration . 8The A-E Assessment . 9Airway (A) . 10Breathing (B) . 11Circulation (C). 12Disability (D). 14Exposure (E) . 15Basic Life Support . 17Chain of Survival . 17Recovery position . 23Choking . 24Advanced Life Support . 26Cardiac Arrest Rhythms . 26Cardiac Arrest Drugs. 28Causes of Cardiac Arrest and their reversal . 28Ending a Resuscitation Attempt . 30Opening the Airway . 30Head Tilt & Chin Lift . 30Jaw Thrust . 30Oropharyngeal Airways (OPA) . 31ILS Pre-course HandbookECG Training Ltd 2020Page 1
Nasopharyngeal Airways (NPA) . 32i-gels . 33Pocket Mask . 34Bag-Valve-Mask (two-person technique) . 34Suction. 35Oxygen . 36Oxygen and Pulse Oximetry . 36Cardiac Rhythms . 37Normal cardiac conduction . 37Cardiac Arrest Rhythms . 37Ventricular Fibrillation . 38Ventricular Tachycardia. 38Asystole . 39Pulseless Electrical Activity . 39Defibrillation . 39Automated External Defibrillators (AED) . 40Safety . 40Manual Defibrillation . 41Post Resuscitation Care . 42If the patient regains consciousness . 42If the patient remains unconscious. 42Anaphylaxis . 43Fainting . 43Seizures . 44Asthma. 45Hypoglycaemia . 45Summary of Drugs for Medical Emergencies . 46Do Not Attempt CPR . 47ReSPECT . 47References. 49ILS Pre-course HandbookECG Training Ltd 2020Page 2
IntroductionThe need for clinicians to be trained in high-quality resuscitation is essential. The term ‘HealthcareProfessional’ is now considered to have a much wider scope and the expectations that are placedon a wider variety of healthcare professionals have undoubtedly increased.Patients are increasingly seen for both consultation and diagnostic services in non-acute hospitallocations that do not always have access to rapid emergency response teams. Our ageing population has an ever-expanding list of existing medical problems and public awareness of health,wellbeing and illness has become more prevalent. As such, the likelihood of Health Care Professionals seeing unwell patients and being involved in cardiac arrests is higher than ever.This course has been aligned to the Resuscitation Council UK (RCUK) guidelines on ImmediateLife Support. The RCUK develop and publish guidelines on resuscitation based on scientific evidence, which is reviewed every five years. This pre-course handbook is based upon the mostrecent guidelines published in January 2015. The primary objective of the RCUK is to promotehigh-quality practice in all aspects of cardiopulmonary resuscitation to improve survival rates.Non-Technical SkillsBefore we learn about the life-saving technical skills of Immediate Life Support (ILS) such asairway management and defibrillation, it is essential to consider the significance of non-technicalskills.Non-technical skills are of a huge importance in an emergency. Three of the most important nontechnical skills are: LeadershipTeamworkAwareness of the situationLeadershipA leader is someone who gives instruction and takes control of the situation.The roles of a team leader are: To make clinical decisions according to RCUK guidelines, including the initial decisionsof calling the resuscitation team, starting CPR and using a defibrillatorIdeally know team members by nameCommunicate information clearly to both the team and any relatives presentEnsure all necessary equipment is availableDelegate tasks playing to the strengths of team members individual skillsRemain calm and potentially manage conflictTake control of the situation/ be authoritative when neededShow understanding and patience towards team members who may be nervousEnsure a post incident debrief takes place to support the teamILS Pre-course HandbookECG Training Ltd 2020Page 3
TeamworkTeamwork is one of the most important non-technical skills.The qualities of a good team member are: Works up to their level of competency, asking for help when neededPerforms to the best of their abilityCommunicates confidently and listens to othersAre supportive to other team membersRaises any concerns about safety or the clinical situationAre accountable for their actionsSituational AwarenessSituational awareness is an understanding of what is happening and how your actions canimpact the situation and outcome. There are various ways to increase awareness of the situation: Ensure personal safety and the safety of those around you is a priorityObserve the surroundings – could this help to identify a cause of the emergency?Know who is present (team members, relatives, bystanders etc.)Gather information from team members, relatives, bystanders etc.Prioritise the various needs the emergency demandsGather equipment that is neededCommunication SkillsProblems with communication contribute to 80% of adverse incidents in hospitalsYou should communicate any concerns about a patient using SBAR(1).(2).Situation – introduce yourself, confirm who you are speaking with and who about, and saywhat you need advice about.“I am (name) calling about (name) and I am concerned that (observations, NEWS score)”Background – brief background information about the patient (past medical history, reasonfor admission)“Patient was admitted with ( ) their last set of observations were ( )”Assessment – include current observations using A-E assessment“He is speaking but his respiratory rate is ( ) his oxygen saturation is ( ), his pulse ( ) BP( ), he has new confusion and on exposure his skin is ( ). I think the problem is ( )”Recommendation – what action is requested/recommended“I have given ( ) but I need you to come and see the patient within ( ) minutes and can I doanything in the meantime?”ILS Pre-course HandbookECG Training Ltd 2020Page 4
SBAR enables an individual to communicate all relevant information and the urgency of the situation in a concise way. It is also important to remember to delegate tasks to specific teammembers (using name where possible) to avoid confusion.DebriefIt is essential to debrief after an emergency event. It has been found that debriefing staff is aneffective strategy in helping them deal with such stressful events and is a useful strategy to improve resuscitation performance. Ideally this should be soon after the event has occurred, butwhere this is not possible it is acceptable to have this any time after the event. It is most important that the debrief is facilitated at some point following the event. This gives individualsthe opportunity to offer support to team members and discuss any concerns that may havearisen during the event.Reporting IncidentsIt is essential to report all emergency incidents and any potential safety incidents according tolocal policy.Remember you have a professional duty of candour(4).Every healthcare professional must be open and honest with patients (or where appropriate,the patient’s advocate) when something goes wrong with their care which has the potential tocause harm or distress. A healthcare professional must inform the patient when something hasgone wrong, apologise, offer a remedy or support to put matters right (if possible) and explainany effects of what has happened. Healthcare professionals must be honest and open with theircolleagues and employers. They must support and encourage each other to be open and honest,and not prevent others from raising concerns.All in-hospital cardiac arrests are reviewed and audited. The National Cardiac Arrest Audit (NCAA)is a UK-wide database of in-hospital cardiac arrests and is supported by the Resuscitation Council(UK) and the Intensive Care National Audit & Research Centre (ICNARC).For out-of-hospital cardiac arrests, data is collected by the UK Ambulance Services.Information you should gather: Patient's detailsDate, time and location of cardiac arrestWho attendedInterventions such as CPR, rescue breaths, use of pocket mask/bag valve maskTime of AED arrival, analysis and shock (if advised), any subsequent shocksILS Pre-course HandbookECG Training Ltd 2020Page 5
Signs of DeteriorationAt ILS training level it is expected that you will not just respond to a cardiac arrest but have thecapability to recognise and respond to signs of deterioration in order to potentially prevent acardiac arrest occurring. Up to 80% of in-hospital cardiac arrests have signs of deterioration priorto the event. Where cardiac arrest is sudden, it is usually due to a catastrophic event such as amyocardial infarction (heart attack), sudden lethal dysrhythmia or major trauma.Chain of PreventionThe chain of prevention is a tool from the RCUK to help ensure deterioration is identified in orderto prevent progression into a cardiac arrest. EducationEducating staff in the assessment and identification of signs of deterioration and how toescalate any concerns about the patient appropriately. MonitoringHealthcare staff should perform patient monitoring and assessment using the A-E approach to assessment. RecognitionHealthcare staff must be able to put their training into practice in order to identify deterioration or any ‘red flags’. One way to assist with staff recognition is through the use ofsystems such as the National Early Warning Score. Call for helpHealthcare staff must understand how to appropriately escalate any concerns to seniorclinicians and relay the relevant information required (for example using SBAR to effectively communicate the urgency of the situation). ResponseThe appropriate clinicians/medical teams must respond to the situation within a reasonable time frame depending on the urgency of the situation. They must be sufficientlytrained to provide an effective response and have appropriate equipment available.ILS Pre-course HandbookECG Training Ltd 2020Page 6
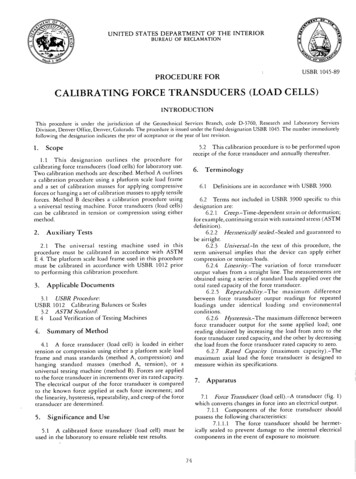
National Early Warning Score(5)The National Early Warning Score (NEWS) is a system to assist in the identification of signs ofpatient deterioration. The patient receives a score based on their observations (Figure 1) whichwill advise on the appropriate action to take (escalation and increased frequency of monitoringthe patient) (Figure 2). The higher the NEW score, the higher the risk of deterioration.Figure 1. The National Early Warning Score System (RCUK, 2016)Figure 2. The recommended response to a patient based on their NEW scorelege of Physicians, 2017)ILS Pre-course HandbookECG Training Ltd 2020(5)(Royal Col-Page 7
Causes of patient deteriorationPatient deterioration can be caused by problems with the airway, breathing and/or circulation.Table 1. Causes of patient deterioration and cardiac arrest relating to airway, breathingand circulation.AirwayBreathingCirculationObstruction may cause arapid deterioration inrespiratory function. Causesof obstruction include:Respiratory inadequacymay be due to an acuteor chronic problem. Thesecauses include:Primary and secondarycauses of cardiacabnormalities include:InfectionMyocardial infarctionAsthmaIschaemiaBlood, vomit and othersecretionsAspirationHypovolaemia (can be associates with blood loss, sepsis,metabolic conditions, anaphylaxis, other fluid loss)Maxillo-facial traumaPneumothoraxHypertensive heart diseaseLocal swelling due to infectionExacerbation of ChronicObstructive Pulmonary DiseaseDrugsLaryngospasm or bronchospasmPulmonary embolusAcidosisTraumaElectrolyte abnormalitiesHaemothoraxHypothermia associated withdrowningPulmonary oedemaElectrocutionCentral Nervous SystemdepressionForeign bodyThe end outcome of cardiac arrest is undoubtedly influenced by the quality of resuscitative carethat is provided. In the peri-arrest period, the aim is to identify the deteriorating patient andinstigate treatments with the aim of preventing the person deteriorating further. In cardiacarrest, the provision of high-quality basic life support and prompt defibrillation coupled withearly mobilisation of emergency resources all contribute to survival and ongoing quality of life.ILS Pre-course HandbookECG Training Ltd 2020Page 8
The A-E AssessmentEarly identification of the deteriorating patient and prevention of cardiorespiratory arrest is thefirst link in the chain of survival. Once cardiac arrest occurs, fewer than 20% of in-hospitalcardiac arrests will survive to go home. In approximately 80% of cases, clinical signs deteriorateover the few hours before arrest. These patients often have slow, progressive physiologicaldeterioration; often hypoxia and hypotension are either not noticed or are treated poorly. Ingeneral, the clinical signs of critical illness are similar whatever the underlying process becausethey reflect failing respiratory, cardiovascular and neurological systems. We use the A to Eassessment as it is a systematic way to ensure we don’t miss anything and eliminate anythinglife threatening before moving on to the next most important section. We prioritise from A to Etreating as we go – for example, if someone has an obstructed airway and cannot breath, wemust treat this immediately – we would not move on to assessing their circulation.ABCDE assessment looks at the Table 2. A normal A-E assessment.AirwayClearNo stridorBreathingRespiratory rate 12-20 min ¹No wheezeNo use of accessory musclesSp02 94-98% (or 88-92% in individuals with COPD)CirculationHeart rate 60-100bpmBlood pressure 120/80Capillary refill time 2 secondsDisabilityAlert on AVPUPEARL (pupils equal and reactive to light)Blood sugar levels normalExposureNo bleedingNo injuryNo swelling, rashes etc.ILS Pre-course HandbookECG Training Ltd 2020Page 9
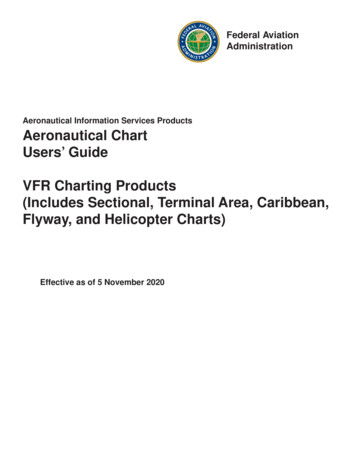
Airway (A)The main airway complication is obstruction. Noisy breathing efforts indicate a partial obstruction, whilst silence indicates a complete obstruction. Noisy sounds include snoring (tongue obstructing the pharynx) and stridor (laryngeal oedema – i.e. anaphylaxis). Strenuous respiratorymovements may be observed such as the use of accessory muscles or see-saw respirations;where the chest and abdomen move in opposite directions. Other signs of an airway probleminclude patient distress and swelling to the lips and tongue. We must also consider any deformities or injuries affecting the upper airway/jaw.There are multiple potential causes of an obstructed airway: The tongueBloodVomitFoodTraumaEpiglottitisSwelling of the pharynxLaryngospasmDepression of the central nervous systemBronchospasmBronchial secretionsInfectionFor the immediate treatment of an obstructed airway use the recognised guidance for the treatment of choking. We will look at this later in the pre-course book.Figure 3. Images of airway problems – jaw injury, deformity of the jaw, obesity andswelling of the tongue.Treatment to prevent an obstructed airway includes:Identifying signs of airway obstruction:-What sound can you hear?Is there increased respiratory effort?Is there any cyanosis (such as blue lips)?Treatments for airway obstruction: Opening the airway with a head tilt chin lift or jaw thrust (we will cover this in moredetail in the airway management chapter)ILS Pre-course HandbookECG Training Ltd 2020Page 10
Suction (if trained) Various airway adjuncts can be used to support the airway (we will cover this in moredetail in the airway management chapter) Putting the patient into the recovery position to protect their airway Give oxygen at high concentration: Give high concentration oxygen using a mask with an oxygen reservoir bag toensure higher inspired oxygen concentrations. High flow oxygen (at 15Lmin ¹) should avoid collapse of the reservoir bag during inspiration.Use pulse oximetry to guide oxygen therapy.Aim for an oxygen saturation of 94-98%. In patients with chronic obstructive pulmonarydisease (COPD) we aim for an Sp02 of 88-92% to prevent hypercapnic respiratory failure. Breathing (B)Breathing problems can be acute or a result of a long-term condition. Respiratory arrest or insufficient respiration will lead to inadequate oxygenation of the blood which will affect vital organs. This will result in a loss of consciousness and ultimately a cardiac arrest.Problems with the lungs (such as chronic obstructive pulmonary disease, asthma, pulmonaryembolus, pulmonary oedema and pneumothorax) can restrict gas exchange.Other causes of breathing problems include depression of the central nervous system, spinalcord injury, muscle weakness/nerve damage (e.g. Guillain-Barre syndrome) and kyphoscoliosis (which can restrict the chest movements).Assessing breathing problemsTo assess breathing problems, look, listen and feel for breathing to identify signs of respiratorydistress. You may notice the patient is sweating, using accessory muscles and has central cyanosis. Count the respiratory rate. The normal adult rate is 12 -20 breaths min-1. A high respiratory rate is a strong indicator of deterioration which may occur rapidly. Assess breathing for the depth of each breath, the rhythm/regularity of respiration andlook for equal chest expansion on both sides. Note the inspired oxygen concentration given to the patient (ideally 15L min-1) and theoxygen saturation reading of the pulse oximeter (if SpO2 monitor unavailable observefor evidence of peripheral or central cyanosis). Remember that a patient receiving highflow oxygen may have a normal Sp02 even if they have insufficient ventilation. Listen to the patient’s breath sounds (by listening close to their face). If a patient isunable to cough/take a deep breath, they may have airway secretions which can beheard as rattling noises. A partial airway obstruction may be heard as a stridor, andconstriction of the bronchial tree may be heard as a wheeze. Continue with the highest possible concentration of inspired oxygen using a mask withan oxygen reservoir. Ensure high flow oxygen (15L min-1) to prevent collapse of thereservoir bag during inspiration. It is important to note that individuals with COPD areILS Pre-course HandbookECG Training Ltd 2020Page 11
at risk of hypercapnic respiratory failure – so giving high concentrations of O2 cancause respiratory depression. It is advised these patients are given 4L min-1 and theirtarget range kept to 88-92% O2.If the patient’s depth or rate of breathing is inadequate or the patient has stoppedbreathing, use a pocket mask or two-person bag-mask ventilation while calling urgently for expert help.Hyperventilation and panic attacks may happen. In most cases, these will resolve withsimple reassurance.Summary of breathing problems: Patient has shortness of breathBreath soundFast respiratory rate ( 25 min-1)Use of accessory muscles/see-saw breathingSp02 94%ConfusionCyanosis (i.e. blue lips or tongue)Chest deformitiesCirculation (C)Causes of circulatory problems include problems with the heart itself or heart abnormalitiessecondary to other conditions.Cardiac problems include: Arrhythmia Acute coronary syndrome i.e. myocardial infarction Hypertensive heart disease Valve disease Cardiomyopathies/Long QT syndromeIn the case of acute coronary syndromes (ACS), they usually present as central chest pain,although atypical presentations can be seen. ACS can be divided into categories based on theresult of a 12-lead ECG and the troponin concentration in their blood.- ST-segment-elevation myocardial infarction (STEMI)- Non ST-segment-elevation myocardial infarction (NSTEMI) (where troponin levels areraised but we do not see ST elevation on the ECG)- Unstable Angina (a lack of ECG or troponin level changes in the presence of chest pain).Initial treatment for suspected ACS includes: 300mg aspirin chewed Sublingual glyceryl trinitrate (unless patient hypotensive) Oxygen if patient Sp02 94% (or 88-92% with COPD) Immediate escalation to cardiology for percutaneous coronary interventionSecondary heart problems occur when changes elsewhere in the body affect the heart. Theheart can be affected by the following: Electrolyte imbalancesDrugsHypervolemiaSeptic shockHypothermiaILS Pre-course HandbookECG Training Ltd 2020Page 12
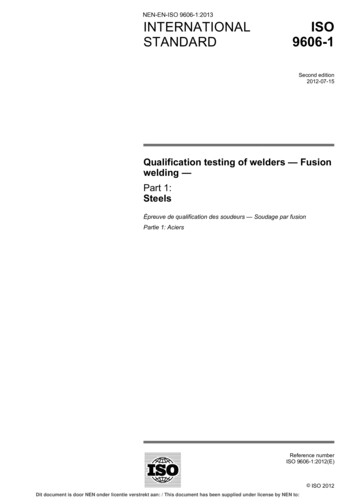
Assessing a patient for circulatory problems: Touch/hold and observe the patient’s hand and feel for the radial pulse (located in thewrist at the base of the thumb). A warm hand with a present pulse will suggest theylikely have an acceptable blood pressure. A cool or pale/mottled hand with a weak orabsent radial pulse will suggest inadequate organ perfusion. Measure the capillary refill time. Apply gentle pressure for five seconds on a fingertipheld at the level of the heart. Time how long it takes for the blanched skin to return tothe colour of the surrounding skin after releasing the pressure. The normal refill time isless than two seconds. A prolonged time suggests poor peripheral perfusion. Other factors (e.g. age of the patient and surrounding temperature) can prolong the time. Count the rate and feel the character of the radial and carotid pulse (is it regular, strong,equal). A normal adult heart rate is 60-100 per min with a good volume. Fast, slow,weak or thready pulses are abnormal in most people. Measure the patient’s blood pressure (comparing this to their usual if known). Note thata patient in shock may have a normal blood pressure due to the compensatory mechanisms of the body increasing peripheral resistance. Note the patient’s urine output if they have a catheter, a low urine output known asoliguria is a urine volume of less than 0.5mL kg-1h-1. Look for signs of bleeding or injury. Insert a cannula if trained to enable fast delivery of fluids where fluid replacement isrequired. This should be given in the form of a 500mL rapid bolus of warmed crystalloidsolution over less than 15 minutes. Reassess the pulse rate and blood pressure every 5 minutes, aiming for the patient‘snormal blood pressure. If this is unknown, in adults aim for a systolic blood pressuregreater than 100 mmHg. If ACS is suspected (e.g. the patient has central chest pain) perform a 12-lead ECG andtreat with aspirin, GTN and oxygen as described previously.Figure 4. A demonstration of assessing Capillary Refill TimeILS Pre-course HandbookECG Training Ltd 2020Page 13
Summary of circulatory problemsCirculatory problems can be identified from a range of features, including: Chest pain Pale complexion Cyanosis Slow capillary refill time (CRT) Abnormal blood pressure (high or low) Anormal heart rate (tachycardia or bradycardia) Increased respiratory rate Oliguria (low urine output)No circulation: Call for help Commence CPR Send for defibrillator Consider IV accessDisability (D)Disability refers to the level of consciousness and neurological condition of the patient. Possiblecauses of reduced levels of consciousness include: HypoxiaLow blood pressureDrugsHypoglycaemiaStrokeThe AVPU scale can be used to identify reduced levels of consciousness. Alert Vocal Stimuli (responds to voice) Painful stimuli (responds to pain) Unresponsive to all stimuli*The painful stimuli should be administered by squeezing the trapezius muscle between theneck and shoulder.We can also consider signs of neurological injury: Stroke (FAST – face arm speech time) PEARL – pupils equal and reactive to lightThere are several potential causes of a reduced level of consciousness.HypoglycaemiaSuspected stroke – call 999Hypoxia – give oxygen at 15L min ¹Cerebral hypoperfusion – i.e. faint – lie patient on floor and raise their legs.Treating causes of disability Always review and treat problems with airway, breathing and circulation. Examine the pupils using a pen torch for their si
ILS Pre-course Handbook ECG Training Ltd 2020 Page 3 Introduction The need for clinicians to be trained in high-quality resuscitation is essential. The term ‘Healthcare Professional’ is now considered to have a much wider scope and the expectations that are placed on a wider variet