Transcription
PEDIATRIC AND ADOLESCENTGYNECOLOGYIna S. Ir abon, MD, FPOGS, FPSRM, FPSGEObstetrics and GynecologyReproductive Endocrinology and Infer tility
To download lecture deck:
Reference Comprehensive Gynecology 7th edition, 2017 (Lobo RA,Gershenson DM, Lentz GM, Valea FA editors) chapter 12,pp 219-236
Outline:1. Gynecologic exam of a child/adolescent2. Normal gynecologic findings in a prepubertalchild3. Gynecologic problems in prepubertal children
The Gynecologic consult Evaluation of young females is age dependent. the office visit and the gynecologic physical examinationare performed differently in a prepubertal child comparedwith an adolescent girl or a mature reproductive-agewoman. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
GYNECOLOGICEXAMINATION OF A CHILD
General Approach Effort should be devoted to gaining the child’s confidence andestablishing rapport. If the interaction is poor during the first visit, the negative experiencewill detract from future physician-patient interactions Gentleness and patience with the time spent and not seem to behurried or rushed. One excellent technique is for the physician to sit, not stand, duringthe initial encounter. This conveys an unhurried approach. Many gynecologic conditions in children can be diagnosed byinspection alone. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Performing gynecologic exam in a child components of a complete pediatric examination: History Inspection with visualization of the external genitalia Non-invasive visualization of the vagina and cervix Rectal examination (if necessary) Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Performing gynecologic exam in a child1. History Obtaining a history from a child is not an easy process. Much of the history must be obtained from the parents. Educate the child on vocabulary to describe the genitalarea. One way to describe genital area and breasts is to callthem “private areas” and define this term as meaningareas that are covered by a bathing suit. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Performing gynecologic exam in a child12 Pediatric and Adolescent Gynecology2. Evaluation of the externalgenitalia. An infant may be examined on hermother’s lap. Young children may be examinedin the frog leg positionA Lithotomy is generally used forgirls 4 to 5 years of ageBand older. CDC o m p re h e n sive G yn e co lo gy 7 th e d itio n , 2 0 1 7 (Lo b o R A , G e rsh e n so n D M ,exam positions for performing a gynecologic exam on a child. A, Frog legLe n tz G M , FigureV ale a12.1FA Differented ito rs)ch ap te r 1 2 , p p 2 1 9 -2 3 6position. B, Knee chest position. C, Prone position. D, Sitting on mom’s lap. (A, from McCann JJ,Kerns DL. The Anatomy of Child and Adolescent Sexual Abuse: A CD-ROM Atlas/Reference. St. Louis:InterCorp: 1999; B and C and D, from Finkel MA, Giardino AP [eds.] Medical Examination of ChildSexual Abuse: A Practical Guide, 2nd ed. Thousand Oaks, CA: Sage, 2002, pp. 46-64.).
Performing gynecologic exam in a child222Part I I I G E N E R A L G Y N E C O LO G Y2. Evaluation of the externalgenitalia.atfctruv Once the child is positioned, the vulvararea and introitus should be inspected. Many gynecologic conditions inchildren may be diagnosed byinspection. Visualization of the introitus:A Gentle Downward lateral traction on thighs Valsalva maneuverBFigure 12.2 Examination of the vulva, hymen, and anterior vagina Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, LentzGM, Valea FA editors) chapterby gentle lateral retraction (A) and gentle gripping of the labia and12, pp 219-236pulling anteriorly (B). (From Emans SJ. Office evaluation of the childand adolescent. In: Emans SJ, Laufer MR, Goldstein DP, eds. Pediatricand Adolescent Gynecology. 4th ed. Philadelphia: Lippincott-Raven;tdyibmimcsidluTmtappaetptP
Performing gynecologic exam in a child3. Non-invasive visualization of thevagina and cervix This can be accomplished without the use of anyinsertion of instruments. One method is to utilize the knee chest positionà vagina will fill with air, aiding the evaluation. an assistant pulls upward and outward on thelabia majora on one side while the examiner doesthe same with the nondominant hand on thecontralateral labia à an oto/ophthalmoscope isused as a magnifying instrument and light sourcebut is not inserted into the vagina. Comprehensive12, pp 219-236Gynecology 7thABCDedition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FigureFA editors)chapter12.1 Different exam positions for performing a gynecoposition. B, Knee chest position. C, Prone position. D, Sitting onKerns DL. The Anatomy of Child and Adolescent Sexual Abuse: A CInterCorp: 1999; B and C and D, from Finkel MA, Giardino AP [e
Performing gynecologic exam in a child3. Non-invasive visualization of thevagina and cervix While the light from theoto/ophthalmoscope is shone into thevagina, the examiner can evaluate thevaginal walls and visualize the cervix as atransverse ridge A foreign object may be visualized usingthis technique.A Following inspection of the vagina andcervix, vaginal secretions may beobtained for microscopic examinationand culture.B Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Performing gynecologic exam in a child4. Rectal Examination (when needed) Most distressing aspect of the examination and may be omitted,depending on the child’s symptoms. Common reasons to perform a rectal examination: genital tractbleeding, pelvic pain, and suspicion of a foreign body or pelvic mass. The normal prepubertal uterus and ovaries are nonpalpable on rectalexamination. The relative size ratio of cervix to uterus is 2 to 1 in a child, in contrastto the opposite ratio in an adult. Except for the cervix, any mass discovered on rectal examination in aprepubertal exam should be considered abnormal. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Performing gynecologic exam in aadolescent Many female adolescents do not want their mother,guardian, or other observers in the examining room. In many adolescent gynecology visits, a full pelvic examis unnecessary. Adolescents often come for examinations withpreconceived ideas that it will be very painful. Teens should be assured that although the exam mayinclude mild discomfort, it is not painful. Use of the “extinction phenomenon” may be helpful. àThe examiner provides pressure lateral to the introituson the perineum prior to insertion of the speculum. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
224Performing gynecologic exam in aadolescentPart III GENERAL GYNECOLOGY .Box 12.1 Common Indications for Pelvic Examination in theAdolescentDelayed pubertyPelvic painSuspicion of intraabdominal diseaseDysfunctional uterine bleedingUndiagnosed vaginal dischargeInability to place tamponsTable 12.1 Clinical Features of Children Presenting withVulvovaginitis Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236FeaturesNumberPercentage
NORMAL FINDINGS:HYMEN AND VAGINA OF APREPUBERTAL CHILD
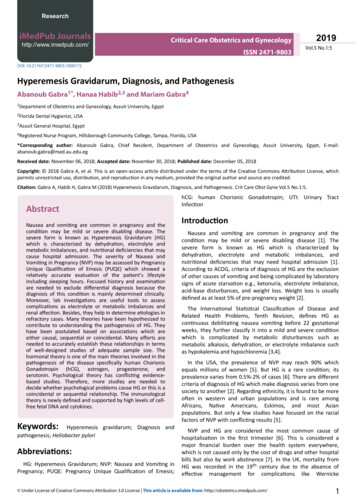
12 Pediatric and Adolescent Gynecology223Types of hymenACB A mounding of hymeneal tissue isoften called a bump.UrethraMembranouscoveropeningDF Hymens are often crescentshaped but may be annular orring-like in configuration. Bumps are usually a normalvariant and are often attached tolongitudinal ridges within thevagina.EGFigure 12.3 Types of hymens. A, Crescentic. B, Annular. C, Redundant. D, Microperforate. E, Septated. F, Imperforate. G, Hymeneal tags. (A through F, From Perlman SE, Nakajima ST, Hertweck SP.Clinical Protocols in Pediatric and Adolescent Gynecology. London: Parthenon Publishing Group; 2004;G, From McCann JJ, Kerns DL. The Anatomy of Child and Adolescent Sexual Abuse: A CD-ROM Atlas/Reference. St. Louis: InterCorp; 1999.) Hymens in newborns areestrogenized, resulting in a thickelastic redundancy. Older unestrogenized girls willhave thin nonelastic hymens. ComprehensiveGynecology7th edition,(LoboRA, Gershensonprimary care setting, nonspecificvulvovaginitis accountsforand open.There is no2017significantgeographicbarrier between DM,majority of vulvovaginitis cases.thevaginaand anus. The vulvar and vaginal epithelium lack the12, pp 219-236There are both physiologic and behavioral reasons why a childprotective effects of estrogen and thus are sensitive to irritationLentz GM, Valea FA editors) chapter
Types of hymen
Vagina The vaginal epithelium of the prepubertal child appears redderand thinner than the vagina of a woman in her reproductiveyears. The vagina is 4 to 6 cm long, and the secretions in a prepubertalchild have a neutral or slightly alkaline pH. Recurrent vulvovaginitis, persistent bleeding, suspicion of aforeign body or neoplasm, and congenital anomalies may beindications for vaginoscopy. The prepubertal vagina is narrower, thinner, and lacking in thedistensibility of the vagina of a woman in her reproductiveyears. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vagina A complete vaginal evaluationshould never be performedunder duress or by force,frequently the reason to usesedation when performing thisexamination on children. Vaginoscopy in a prepubertal childmost often requires sedation witha brief inhalation or intravenousanesthetic, but it can also beperformed in the office witholder, cooperative children Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vagina We can also use: Kelly air cystoscope,contact hysteroscopes, pediatriccystoscopes, small- diameterlaparoscopes, plastic vaginoscopes,and special virginal speculumsdesigned by Human and Pederson. The ideal pediatric endoscope is acystoscope or hysteroscope becausethe accessory channel facilitates theretrieval of foreign bodies as well asvaginal lavage. A nasal speculum or otoscope can alsobe used Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
PROBLEMS INPREPUBERTAL CHILDREN
Vulvovaginitis most common gynecologic problem in the prepubertalfemale. classic symptoms of vulvovaginitis: introital irritation(discomfort/pruritus) or dischargeNote: The prepubertal vagina is neutral or slightly alkaline. With puberty, vagina becomes acidic under the influence ofbacilli dependent on a glycogenated estrogen-dependentvagina. Breast budding is a reliable sign that the vaginal pH isshifting to an acidic environment Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
1. Vulvovaginitis Physiologic and behavioral reasons why a child is susceptible tovulvar infection: Physiologically:1. The child’s vulva and vagina are exposed to bacterialcontamination from the rectum more frequently than are theadult’s.2. Because the child lacks the labial fat pads and pubic hair of theadult, when a child squats, the lower one third of the vagina isunprotected and open.3. There is no significant geographic barrier between the vagina andanus.4. The vulvar and vaginal epithelium lack the protective effects ofestrogen and thus are sensitive to irritation or infection. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
1. Vulvovaginitis5. The vaginal epithelium of a prepubertal child has a neutral orslightly alkaline pH, which provides an excellent medium forbacterial growth.6. The vagina of a child lacks glycogen, lactobacilli, and asufficient level of antibodies to help resist infection. Note: The normal vagina of a prepubertal child is colonized byan average of nine different species of bacteria: four aerobicand facultative anaerobic species and five obligatory anaerobicspecies. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
1. VulvovaginitisBehavioral: A major factor in childhood vulvovaginitis is poor perineal hygiene. This results from the anatomic proximity of the rectum and vagina;most youngsters are unsupervised when they defecate. Many youngsters wipe their anus from posterior to anterior and thusinoculate the vulvar skin with intestinal flora. A minor vulvar irritation may result in a scratch-itch cycle, with thepossibility of secondary seeding because children wash their handsinfrequently. Children’s clothing is often tight fitting and nonabsorbent, whichkeeps the vulvar skin irritated, warm, moist, and prone tovulvovaginitis. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
4. Mononucleosis5. Scarlet tibodiesto6. Kawasaki diseaseBox 12.2 Etiologic Factors of Premenarcheal Vulvovaginitishelp resist infection. The normal vagina of a prepubertal childOther Viral IllnessesBacterial1. Molluscum contagiosum in genital areais colonized by an average of nine different species of bacteria:A. Nonspecific2. Condylomata acuminatefour aerobicand facultativeanaerobic species and five obligatory1. Poorperineal hygiene3. Herpes simplex type IIanaerobic2.species.Intestinal parasitic invasion with pruritusPhysical/Chemical AgentsA majorfactor inbodieschildhood vulvovaginitis is poor perineal3. Foreign1. Sandbox4. Urinarytractresultsinfectionsirritationproximity ofhygiene (Box12.2). Thisfrom withthe anatomic2. TraumaB. Specificthe rectumand vagina coupled with the fact that following toilet3. Bubble bathtraining, cate.4. Other1. Group A: β-hemolytic streptococciMany llergic/Skin Conditions2. Streptococcus pneumoniathus inoculatethe vulvar skinwith intestinal flora. A minor vul3. Haemophilusinfluenzae/parainfluenzae1. Seborrhea4. Staphylococcusvar irritationmay result in aaureusscratch-itch cycle, with the pos2. Lichen sclerosus5. Neisseriameningitides3. Psoriasissibility of secondaryseedingbecause children wash their hands6.Escherichiacoli4. Eczemainfrequently. Children’s clothing is often tight fitting and nonab7. Shigella flexneri/sonnei5. Contact dermatitissorbent, whichkeeps the vulvar skin irritated, warm, moist, and8. Other entericsTumorsprone to vulvovaginitis.9. Neisseria gonorrhoeaeOtherIn somenonspecificvulvovaginitis may be caused by10.cases,Chlamydiatrachomatis1. Prolapsed urethraProtozoal—Trichomonascarrying viralinfections from coughing into the hands directly to2. Ectopic ureterMycoticthe abradedvulvar epithelium. Similarly, a child with an upper1.CandidaalbicansFrom Blythe MJ, Thompson L. Premenarchal vulvovaginitis. Indiana Med.respiratory tract infectionmay autoinoculate her vulva, espe1993;86(3):236-239.2. Othercially Helminthiasis—Enterobius vermicularischildren mayalso be causedby a varietyViral/BacterialSystemicIllnessspecific pathogens suchmay be discovered by means of a flashlight or by dabbing of theas group 1.A orgroup poxB β-hemolytic streptococci, HaemophilusChicken2.andMeaslesvulvar skin with clear cellophane adhesive tape ideally before theinfluenzae,Shigella boydii; Neisseria gonorrhoeae, Trichomonas3.Pityriasisroseachild has arisen in the morning. The tape is subsequently examvaginalis, and Chlamydia trachomatis may also be responsible in4. Mononucleosisined under the microscope.cases associated with abuse but are significantly less common.5. Scarlet feverDespite common belief, mycotic (yeast) vaginal infections arePinwormsare anothercause of vulvovaginitis in prepubertal6. Kawasakidiseasenot commonprepubertalas chapterthe alkaline pH of thechildren.OtherApproximately20% Gynecologyof female childreninfectedwithRA, GershensonIllnesses ViralComprehensive7th edition,2017 (LoboDM,inLentzGM, Valeachildren,FA editors)vagina does not support fungal growth. Mycotic vaginal pvulvovaginitis.The12, pp 219-236Molluscumcontagiosumin genitalarea2.Condylomataacuminatemay be seen in immunosuppressed prepubertal girls such as HIVclassic symptom of pinworms is nocturnal vulvar and perianal3.HerpessimplextypeIIpatients, diabetic children, or patients on chronic steroid therapy. Ititching. At night the milk-white, pin-sized adult worms migrate
1. Vulvovaginitis: Pinworms Approximately 20% of female children infected withpinworms (Enterobius vermicularis) develop vulvovaginitis. The classic symptom of pinworms is nocturnal vulvar andperianal itching. At night the milk-white, pin-sized adult worms migratefrom the rectum to the skin of the vulva to deposit eggs. They may be discovered by means of a flashlight or bydabbing of the vulvar skin with clear cellophane adhesivetape ideally before the child has arisen in the morning. The tape is subsequently examined under the microscope. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
1. Vulvovaginitis: Mycotic infections Mycotic vaginal infections are not common in prepubertalchildren, as the alkaline pH of the vagina does not supportfungal growth. Mycotic vaginal infections may be seen inimmunosuppressed prepubertal girls such as HIV patientsor patients on chronic steroid therapy. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vulvovaginitis: Differential Diagnosis The differential diagnosis of persistent or recurrent vulvovaginitisnot responsive to treatment should include the followingconsiderations:1. foreign body (bloody or purulent discharge)2. primary vulvar skin disease3. ectopic ureter (rare anomaly; may only intermittently release asmall amount of urine)4. child abuse.5. systemic skin diseases, including lichen sclerosus, seborrheicdermatitis, psoriasis, and atopic dermatitis. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vulvovaginitis: Differential Diagnosis Notes: The classic perianal “figure-8” or“hourglass” rash is indicative oflichens scleroses with white patchesand in some cases blood blisters. An ectopic ureter empties into thevagina Positive identification of gonorrhea,or chlamydia in a child withpremenarcheal vulvovaginitis isconsidered diagnostic of sexualmolestation. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vulvovaginitis: Treatment The foundation of treating childhood vulvovaginitis isthe improvement of local perineal hygiene. The majority of symptoms improve with hygienicchanges and sitz baths. Relief of vulvar irritation may be facilitated by using abland cream, such as zinc oxide creams or cod liver oilcreams low-potency steroids, or oral antibiotics given for 10 to14 days, are often reserved for recalcitrant cases Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Vulvovaginitis: Treatment Vaginal cultures help to determine thechoice of an oral antibiotic. However,cultures usually will not show a specificpathogen. In recurrent cases, a broad spectrumantibiotic may be appropriate todecrease the E. coli inoculums. One method of obtaining a vaginalculture in children is to use anasopharyngeal small swab moistenedwith nonbacteriostatic saline Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
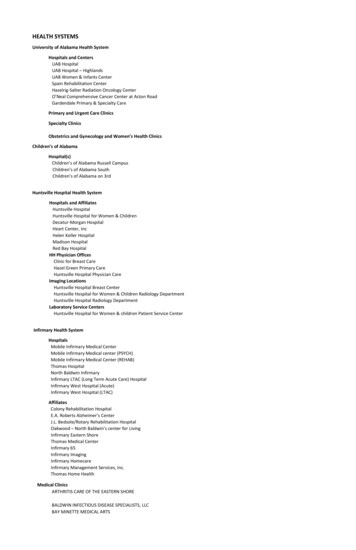
2. Labial Adhesions (Adhesive Vulvitis) Denuded epithelium of adjacent labiaminora agglutinates and fuses the twolabia together, creating a “flatappearance” of the vulvar surface. A tell-tale somewhat translucentvertical midline line is visible onphysical exam at the siteagglutination. This thin, narrow line in a verticaldirection is pathognomonic for labialadhesions Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
2. Labial Adhesions (Adhesive Vulvitis) Labial adhesions are most common in young girls between2 and 6 years of age. Estrogen reaches a nadir during this time, predisposing thenonestrogenized labia to denudation In one large study, the average age of a child withagglutination of the labia was 2½ years; 90% of casesappeared before age 6. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
2. Labial Adhesions (Adhesive Vulvitis) No treatment is absolutely necessary or mandatoryfor labial adhesions unless the child is symptomatic. Symptoms include voiding difficulties, recurrentvulvovaginitis, discomfort from the labia pulling at theline of adhesions, and in rare cases bleeding from theline of adhesion pulling apart. spontaneous separation of the adhesive vulvitis within6 to 18 months. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
2. Labial Adhesions (Adhesive Vulvitis) Attempts to separate the adhesions apart in the office bypulling on the labia minora should not be done. à verypainful, and the raw edges are likely to readhese The most commonly utilized treatment of this condition istopical estrogen cream dabbed onto the labia two timesper day at the site of fusion à usually result inspontaneous separation, usually in approximately 2 to 8weeks. caregiver should be instructed to apply the cream to theline, as the lateral pigmentation indicates the estrogen isbeing applied lateral to the actual adhesion. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
2. Labial Adhesions (Adhesive Vulvitis) Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
3. Physiologic Discharge of Puberty Gray-white coloration, may appear slightly yellow Represents desquamation of the vaginal epithelium. The estrogenic environment allows acid-producing bacilli tobecome part of the normal vaginal ecosystem. The acids the bacilli produce cause a desquamation of theprepubertal vaginal epithelium. The only treatment necessary is reassurance of both motherand child that this is a normal physiologic process that willsubside with time. Symptomatic children may be treated with sitz baths andfrequent changing of underwear. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
4. Urethral Prolapse Not a rare event in children. The most common presentation is noturinary symptomatology butprepubertal bleeding. A sharp increase in abdominalpressure, such as coughing, precedesthe urethral prolapse. The distal aspect of urethral mucosamay be prolapsed along the entire360 degrees of the urethra à reddonut-like structure. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
4. Urethral Prolapse It is critical to distinguish this from grapelike masses of sarcomabotryoides that originate from the vagina. Treatment is conservative and noninteventional à application ofvarious medications including estrogen creams and antibioticointments. Surgery is only necessary where necrosis is obviously present. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
5. Lichen Sclerosus (LS)/ lichen sclerosusatrophicus Skin dystrophy most commonly seen inpostmenopausal women andprepubertal children. The cause is unclear, but may beassociated with autoimmunephenomena. Histologically there is thinning of thevulvar epithelium with loss of the retepegs. The most common symptoms arepruritus and vulvar discomfort. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
5. Lichen Sclerosus (LS)/ lichen sclerosusatrophicus lesions are always limited by the labiamajora. If lesions go beyond the labiamajora, the condition is unlikely to be LS. The lesion often appears in an hourglassor figure-8 formation involving the genitaland perianal area. The skin may belichenified with a parchment- likeappearance. Parents may note that the genital areaappears whitened. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
5. Lichen Sclerosus (LS)/ lichensclerosus atrophicus
5. Lichen Sclerosus (LS)/ lichensclerosus atrophicus In cases where the diagnosis is unclear, a small punchbiopsy may confirm the diagnosis. The treatment of LS in children should always start withavoiding irritation or trauma to the genital epithelium.LS is a skin disorder in which lesions are most likely tooccur in epithelium that is irritated. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
5. Lichen Sclerosus (LS)/ lichensclerosus atrophicus high-potency steroids such as clobetasol is the initial step intreatment of this condition. Tapering the steroid level should be considered as soon as aresponse is seen or within a 4- to 6-week interval. Tapering can be achieved by following the initial treatmentwith a 2- to 3-week of midpotency steroid such asbetamethasone and conclude with 1% hydrocortisone foranother 2 weeks the use of ointments is preferred over creams given there isless irritation compared with creams and the petroleum baseof ointments appear to help it stay in place longer. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
6. Vaginal Bleedingsyndrome (polyosentation of isolaThe differentiForeign objecttal developmentGenital traumalichen sclerosus,Sexual abusesions, trauma (abLichen sclerosusable genital wartInfectious vaginitis (especially from Shigella)tumors (sarcomaUrethral prolapsevagina) and an uBreakdown of labial adhesionsdrome. Lists ofFriable genital warts or vulvar lesionsVaginal tumoring often also incRare presentation of McCune-Albright syndrome (typically havefrom ingestion ofbreast development)of estrogen topicIsolated menarche (controversial)would rarely proDermatologic conditions with secondary excoriationduce a withdrawNongenital bleeding; mistaken as genital: rectal and urinarydevelop a whiteComprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chaptervaginal spotting12, pp 219-236gens. The discharBox 12.3 Differential Diagnosis of Prepubertal Bleedingwithout Any Breast Development 1
7. Foreign Bodies The majority of foreign bodies arefound in girls between 3 and 9years of age Most common are small wads oftoilet paper. The classic symptom is a foul,bloody vaginal discharge. However,the discharge is often purulent andwithout blood. The presence of unexplainedvaginal bleeding is an indication fora vaginoscopy. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
8. Shigella Vaginitis Cultures for Shigella should be strongly consideredin any child with no obvious cause for prepubertalbleeding. Rarely, vaginitis caused by other organisms canalso present with prepubertal bleeding. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
9. VULVAR TRAUMA: LACERATIONSAND STRADDLE INJURY One of the most common causes of genital trauma in achild is a straddle injury Common straddle injuries in children occur on playgroundclimbing structures, such as a monkey bar, or fence rails. A straddle injury generally results in unilateral andsuperficial injury and very rarely involves the hymen. The lack of the mature reproductive woman’s fat pad inthe vulvar area predisposes a young child to bleeding fromtrauma. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
THE OVARY AND ADNEXA INPEDIATRIC AND ADOLESCENTGYNECOLOGY: CYSTS,TUMORS, AND TORSION
functional ovarian cysts – most common physiologicovarian mass in this age group Teratoma (dermoid) – most common benign tumor(pathologic) The appropriate management may depend on the ageand on the appearance of the cyst on ultrasound Cysts in neonates can generally be observed withresolution. Small follicular cysts in preadolescent females areusually self-limiting Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Prenatal ovarian cysts Before a diagnosis of an ovarian cyst is made, it iscritical to exclude urinary or gastrointestinalanomalies. Fetal malignancy is quite rare. Comprehensive Gynecology 7th edition, 2017 (Lobo RA, Gershenson DM, Lentz GM, Valea FA editors) chapter12, pp 219-236
Neonatal Ovarian Cysts Simple cystic ovarian masses in newborns andneonates can be followed expectantly. Parents should be given ovarian torsion warnings, andif the infant presents with acute vomiting orabdominal pain, she should be immediately evaluatedfor ovar
12 Pediatric and Adolescent Gynecology 221 they are usually too short for older girls and less optimal. Local anesthesia of the vestibule may be obtained with 2% topical vis-cous lidocaine (Xylocaine)