Transcription
Tactical Combat Casualty Carequick reference guideFirst editionCopyright 2017
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)EDITOR:HAROLD R. MONTGOMERY, ATPMSG(RET), U.S. ARMYCONSULTANTS & REVIEWERSFRANK K. BUTLER, MDMICHAEL A. REMLEY, ATPCAPT(RET), U.S. NAVYSFC, U.S. ARMYSTEPHEN D. GIEBNER, MD, MPHTRAVIS A. SHAW, NREMT-PCAPT(RET), U.S. NAVYMSGT, U.S. AIR FORCEWIN KERR, ATPJEREMY K. TORRISISCPO, U.S. NAVYCURTIS C. CONKLIN, ATPMSG, U.S. ARMYTHOMAS A. RICH, NREMT-PCMSGT, U.S. AIR FORCEDANIEL M. MORISSETTE, ATPMSG, U.S. ARMYCopyright Statement:The copyright holder of this publication assigns unlimited royalty-freereproduction licensing exclusively to the United States Government and NATOmember governments. U.S. Government Printing Offices, specificallyDepartment of Defense installation printing services are authorized toreproduce this publication for use by military personnel.The copyright holder retains reproduction and royalty licensing for all otherindividuals or organizations except the U.S. Government. No part of thematerial protected by this copyright may be reproduced or utilized in any form,electronic or mechanical, including photography, recording, or by anyinformation storage and retrieval system, without written permission from thecopyright owner.Copyright, 2017 by HR MontgomeryISBN: 978-0-692-90697-2
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)TABLE OF CONTENTSABBREVIATED TCCC GUIDELINES .PAGE 4CARE UNDER FIRE ALGORITHM . . .PAGE 9TACTICAL FIELD CARE ALGORITHMS .PAGE 10Massive Hemorrhage11C - Fluid Resuscitation15Burns18Airway Management12Hypothermia Communications19C - Bleeding13Pain Management17CPR19C - IV Access14Antibiotics17Documentation19C - TXA14Wounds18Prep for Evacuation20TACTICAL EVACUATION CARE ALGORITHMS .PAGE 21Transition of Care21C - Fluid Resuscitation27Wounds31Massive Hemorrhage22Trauma Brain Injury28Burns31Airway Management23Hypothermia Prev29Splints31Respiration/Breathing24Eye Trauma29Communications32C - Bleeding25Monitoring29CPR32C - IV Access26Pain Management30Documentation32C - TXA26Antibiotics30DD1380 TCCC CARD . .PAGE 33TRIAGE & EVACUATION CATEGORIES .PAGE 34MEDEVAC REQUEST FORMAT. .PAGE 35CASUALTY AAR SUBMISSION . .PAGE 37COTCCC RECOMMENDED ITEMS .PAGE 40TCCC PHARMACOLOGY. . .PAGE 41PLANNING FOR CASUALTY RESPONSE. .PAGE 46KEY REFERENCES & RECOMMENDED READING .PAGE 47GLOSSARY . .PAGE 51CONVERSIONS . .PAGE 52DRUG QUICK REFERENCE . .PAGE 53
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)FORWARDTactical Combat Casualty Care (TCCC) has saved hundreds of lives during our nation's conflicts in Iraq andAfghanistan. Nearly 90% of combat fatalities occur before the casualty reaches a Medical treatment facility, itis clear that the prehospital phase of care is the focus of efforts to reduce deaths in combat. Very few militaryphysicians, however, have had training in this area. As a result, at the onset of hostilities, most combatMedics, corpsmen, and para-rescue personnel (PJs) in the US Military were trained to perform battlefieldtrauma care through the use of civilian-based trauma courses that were not designed for the prehospitalcombat environment and did not reflect contemporary knowledge in this area.This challenge was met by the Committee on TCCC (CoTCCC) voting members and its many liaison membersthat collectively comprise the TCCC Working Group. This remarkably eclectic group includes trauma surgeons,emergency medicine physicians, internists, family medicine physicians, operational physicians and physicianassistants, combat medical educators, trauma researchers, pathologists, combat medical doctrine developers,medical equipment specialists, and combat medics, corpsmen, and PJs. All of the US Armed Services are wellrepresented in the group's membership and 100% of the CoTCCC voting members have been to war. TheCoTCCC and the TCCC Working Group represents different services, disciplines, and military experiences, allbrought to bear on a single goal - reducing preventable deaths on the battlefield.No such group existed when the Twin Towers fell. The US Special Operations Command initially funded thegroup as a research effort, then ownership of the group was successively assumed by the Naval OperationalMedicine Institute, the Defense Health Board, and now the Joint Trau-ma System.This group has taken the TCCC Guidelines as they existed in 2001 and continually updated them throughoutthe 15 years of war, based on input from the Joint Trauma System Performance Improvement traumateleconferences, published case reports and case series from the war zones, breakthroughs in military Medicalresearch, and new publications from the civilian medical literature that bear on combat trauma. It hasprocessed a continual steam of input from the battlefield throughout the war years and ensured thatbattlefield trauma care lessons learned were not just noted, but acted upon.Through the ongoing volunteer efforts of this dedicated group of individuals - which met quarterly throughoutmost of the war - US Forces have had prehospital trauma care guidelines that were customized for thebattlefield and updated continuously based on real-time evaluation of outcomes from ongoing combatoperations. This is the first time in our nation's history that this has occurred.The success of TCCC effort had been well documented. It is a great tribute to all of the members of the CoTCCCand the TCCC Working Group, that it has been able to transcend service and Medical specialty differences,process new information expertly, and develop evidence-based, best-practice guidelines that have completelytransformed battlefield trauma care.It is to the Committee on TCCC and all of our valued colleagues in the TCCC Working Group that this TCCC textis dedicated. Our country and its casualties owe you all a profound measure of thanks.Frank Butler, MDCAPT (Retired), MC, USNChairman, Committee on Tactical Combat Casualty Care
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)ABBREVIATED TCCC GUIDELINES31 JAN 2017Basic Management Plan for Care Under FireReturn Fire and take coverDirect or expect casualty to remain engaged as a combatant if appropriateDirect casualty to move to cover and apply self-aid if able.Try to keep the casualty from sustaining additional wounds.Stop life-threatening external hemorrhage if tactically feasible:- Direct casualty to control hemorrhage by self-aid if able.Use a CoTCCC-recommended limb tourniquet for extremity hemorrhage- Move the casualty to coverAirway management is generally best deferred until the Tactical Field Care phase.Basic Management Plan for Tactical Field CareEstablish Security Perimeter IAW Tactical SOPs. Maintain situational awareness.Triage Casualties as required. Altered mental status is criteria to have weapons cleared/secured, communications gearsecured and sensitive items redistributed.Massive HemorrhageAssess for unrecognized hemorrhage and control all life-threatening bleeding.Use one or more CoTCCC-recommended limb tourniquets if necessary.Use a CoTCCC approved hemostatic dressing for compressible hemorrhage not amenable to limb tourniquetuse.Immediately apply a CoTCCC-recommended junctional tourniquet if the bleeding site is amenable to use of ajunctional tourniquet.Airway ManagementUnconscious casualty without airway obstruction:-Chin lift or jaw thrust maneuver-Nasopharyngeal airway-Place the casualty in the recovery positionCasualty with airway obstruction or impending airway obstruction:-Allow a conscious casualty to assume any position that best protects the airway, to include sitting up-Chin lift or jaw thrust maneuver-Nasopharyngeal airway-Place an unconscious casualty in the recovery positionIf the previous measures are unsuccessful perform a surgical cricothyroidotomy using one of the following:-CricKey technique-Bougie-aided open surgical technique-Standard open surgical technique*Use lidocaine if the casualty is conscious4
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)ABBREVIATED TCCC GUIDELINES31 JAN 2017Basic Management Plan for Tactical Field Care continuedRespiration/BreathingIn a casualty with progressive respiratory distress and known or suspected torso trauma, consider a tensionpneumothorax:-Decompress the chest on the side of the injury at the primary or alternate site.All open and/or sucking chest wounds should be treated by:-Applying a vented chest seal (preferred)-Applying a non-vented chest seal-Burp the wound if indicated for breathing difficultyInitiate pulsoximetry monitoring.Monitor for tension pneumothorax.Casualties with moderate/severe TBI should be given supplemental oxygen when available to maintain anoxygen saturation 90%.Circulation - BleedingApply a pelvic binder for suspected pelvic fracture and/or severe blunt force or blast injury.Reassess prior tourniquet application:-Expose the wound and determine if a tourniquet is needed; if bleeding is not controlled then tightentourniquet if possible.-If the first tourniquet does not control bleeding after tightening, then add a second tourniquet side-byside with the first.Convert Limb tourniquets and junctional tourniquets if the following three criteria are met:-The casualty is not in shock.-It is possible to monitor the wound closely for bleeding.-The tourniquet is not being used to control bleeding from an amputation.Convert tourniquets in less than 2 hours if bleeding can be controlled with other means.Expose and use an indelible marker to clearly mark all tourniquet sites with the time of tourniquet application,reapplication, conversion, or removal.Circulation - IV/IO AccessStart an 18-gauge IV or Saline Lock if indicated.If IV access is not obtainable, use an intraosseous (IO) needle.Circulation - TXAIf a casualty is anticipated to need a blood transfusion, then administer 1 gram of tranexamic acid (TXA) in100ml of NS or LR over 10min ASAP but NOT beyond 3 hours post injury.Circulation - Fluid ResuscitationAssess for hemorrhagic shock:-If not in shock PO fluids are permissible if casualty is conscious and can swallow.-If in shock resuscitate with:Whole blood (preferred) orPlasma, RBCs and platelets (1:1:1) orPlasma and RBCs (1:1) orPlasma or if blood products not available,Hextend or Lactated Ringers or Plasma-Lyte-AResuscitate with above fluids until a palpable radial pulse, improved mental status orsystolic BP of 80-90 mmHg is present. Discontinue fluids when one or more end points are achieved.Reassess casualty frequently to check for recurrence of shock. If shock recurs, verify all hemorrhage is undercontrol and repeat fluid resuscitation as above.5
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)ABBREVIATED TCCC GUIDELINES31 JAN 2017Basic Management Plan for Tactical Field Care continuedHypothermia PreventionMinimize casualty environmental exposure and promote heat retention.Keep personal protective gear on if feasible. Replace wet clothing if possible. Get casualty onto insulatedsurface ASAP.Use a hypothermia prevention kit with active rewarming.If none above is available, then use dry blankets, poncho liners, or sleeping bags and keep the casualty warmand dry.Warm IV fluids are preferred.Penetrating Eye Trauma - If penetrating eye injury is noted or suspected:Perform a rapid field test of visual acuity and document findings.Cover eye with a rigid eye shield (not a pressure patch).Administer Combat Wound Medication Pack if possible and/or administer IV/IM antibiotics per below.Monitoring – Initiate advanced electronic monitoring of vital signs if available.Analgesia/Pain ManagementAnalgesia on the battlefield should generally be achieved by one of three options:Mild to Moderate Pain and/or Casualty can swallow and is still able to fight:-Administer TCCC Combat Wound Medication Pack (CWMP)Moderate to Severe Pain and casualty IS NOT in Shock-Oral Transmucosal Fentanyl Citrate (OTFC) 800mcgModerate to Severe Pain and casualty is in hemorrhagic shock or respiratory distress-Administer Ketamine 50mg IM or IN repeating q30min prnOR-Administer Ketamine 20mg Slow IV or IO repeating q20min prn*Endpoint control of pain or development of nystagmus.*Consider Ondansetron 4mg ODT/IV/IO/IM q8hours prn for nausea and vomiting.AntibioticsIf able to take PO, then administer Moxifloxacin 400mg PO qDaily from CWPP.If unable to take PO, administer Ertapenem 1 gram IV/IM qDaily.WoundsInspect and dress known wounds.Check for Additional Wounds.BurnsFacial burns should be aggressively monitored for airway status and potential inhalation injury.Estimate total body surface area (TBSA) burned to nearest 10%.Cover burned areas with dry, sterile dressings. For burns 20% TBSA, consider placing casualty immediately inHPMK or other hypothermia prevention means.Fluid Resuscitation (USAISR Rule of Ten):-If burns 20% TBSA, initiate IV/IO fluids ASAP with Lactated Ringers, NS, or Hextend. If Hextend, then nomore than 1000ml followed by LR or NS as needed.-Initial IV/IO fluid rate %TBSA X 10ml/per hour for adults 40-80 kg ( 100ml/hr for every 10kg above 80kg).-If hemorrhagic shock is present then resuscitate IAW fluid resuscitation in Circulation section.All TCCC interventions may be performed on or through burned skin.6
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)ABBREVIATED TCCC GUIDELINES31 JAN 2017Basic Management Plan for Tactical Field Care continuedSplinting - Splint Fractures and Recheck Pulses.CommunicationCommunicate with the casualty if possible. Encourage, reassure, and explain care.Communicate with tactical leadership ASAP and throughout treatment. Provide casualty status and evacrequirements.Communicate with the evacuation system to arrange TACEVAC.Communicate with medical personnel on evacuation assets and relay mechanism of injury, injuries sustained,signs/symptoms and treatments rendered.DocumentationDocument clinical assessments, treatments rendered, and changes in the casualty's status on a TCCC Casualty Card (DDForm 1380) and forward this information with the casualty to the next level of care.Cardiopulmonary resuscitation (CPR)Battlefield blast or penetrating trauma casualties with no pulse, no ventilations, and no other signs of lifeshould not be resuscitated.Casualties with torso trauma or polytrauma with no pulse or respirations should have bilateral needledecompression performed to confirm/deny tension pneumothorax prior to discontinuing care.Prepare for EvacuationComplete and secure TCCC Card (DD1380) to casualty.Secure all loose ends of bandages and wraps.Secure hypothermia prevention wraps/blankets/straps.Secure litter straps and consider additional padding for long evacuations.Provide instructions to ambulatory patients as needed.Stage Casualties for evacuation.Maintain security at evacuation site.7
TACTICAL COMBAT CASUALTY CARE(TCCC / TC3)ABBREVIATED TCCC GUIDELINES31 JAN 2017Basic Management Plan for Tactical Evacuation Care (TACEVAC)In addition to the principles of Tactical Field Care consider the following for Tactical Evacuation Care:Transition of CareTactical force should establish evacuation point security and stage casualties for evacuation.Tactical force personnel/medic should communicate patient status to TACEVAC personnel to include stable/unstable, injuries identified, and treatments rendered.TACEVAC personnel stage casualties on evac platform as required.Secure casualties on evac platform IAW unit policies, platform configurations, and safety requirements.TACEVAC medical personnel reassess casualties and re-evaluate all injuries and interventions.Airway Management- Consider the following for casualty with airway obstruction or impending airway obstruction:-Supraglottic airway, or-Endotracheal intubationBreathingConsider chest tube insertion if no improvement and/or long transport is anticipated.Administer oxygen when possible for the following types of casualties:-Low oxygen saturation by pulse oximetry-Injuries associated with impaired oxygenation-Unconscious casualty-Casualty with TBI (maintain oxygen saturation 90%)-Casualty in shock-Casualty at altitudeTraumatic Brain Injury-Casualties with moderate/severe TBI should be monitored for:-Decreases in level of consciousness-Pupillary dilation-SBP should be 90 mmHg-O2 sat 90-Hypothermia-PCO2 (If capnography is available, maintain between 35-40 mmHg)-Penetrating head trauma (if present, administer antibiotics)-Assume a spinal (neck) injury until clearedIf impending herniation is suspected take the following actions:-Administer 250 cc of 3 or 5% hypertonic saline bolus-Elevate the casualty’s head 30 degrees-Hyperventilate the casualtyCommunicationCommunicate with the casualty if possible. Encourage, reassure, and explain careCommunicate with next level of care and relay mechanism of injury, injuries sustained, signs/symptoms, andtreatments rendered.8
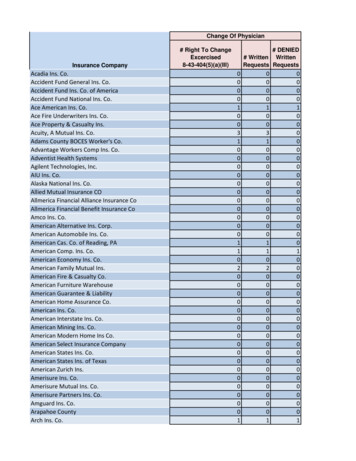
TACTICAL COMBAT CASUALTY CAREALGORITHMCARE UNDER FIREIn accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017CasualtySustainedReturn Fire and Take CoverDirect casualtyto move tocover andapply self-aidYESCasualtyConscious?NOTry to keep casualtyfrom sustainingadditional wounds.Move casualtyto cover iftacticallyfeasibleTry to keep casualtyfrom sustainingadditional wounds.Casualty moved to coveror extrication needed*STOP LIFETHREATENINGBLEEDINGUse CoTCCCRecommended LimbTourniquet appliedproximal to bleedingsiteYESLimbTourniquetIndicated?LIFE THREATENING BLEEDING:Spurting Blood or Flowing BloodBlood soaking rapidly through uniformor pooling on the groundComplete Amputation* Extrication-Casualties should be extricated fromburning vehicles or buildings and movedto relative safety. Do what is necessaryto stop burning process.NOPlace tourniquets “High &Tight” if bleeding site is noteasily identifiableAirway management isgenerally best deferred untilthe Tactical Field Care phaseContinue with Fight /MissionMove casualty to CCP orsecure area and initiateTactical Field CareCasualty Movement:- The fastest method is dragging alongthe long axis of patient’s body by tworescuers.-Spinal precautions or stabilization shouldonly be considered after a casualty isremoved from the enemy threat andindicated by mechanism of injury.Indicates All Combatantsand Combat Lifesavercapability level skillTACTICAL FIELD CARE9Indicates Combat Mediccapability level skillIndicates CombatParamedic or SOF Mediccapability level skill
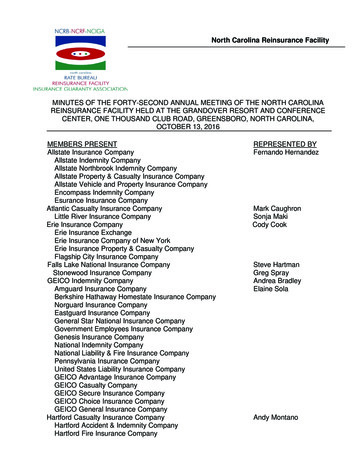
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CAREEstablish Security Perimeter.Maintain Situational Awareness.In accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Triage as required.Casualties with altered mental status should have:- Weapons cleared and secured- Communications secured- Sensitive missions items redistributedTriage multiple casualties intoCCP or secure area as requiredMASSIVEHEMORRHAGEUncontrolledMassive ExternalHemorrhage orTraumatic AmputationPresent?NOYESTighten previously applied tourniquet or apply aYESCoTCCC-recommended Limb Tourniquet. Apply and2 Tourniquet if bleeding not controlled.Amenable to LimbTourniquet?NOYESNOUse CoTCCC-recommendedHemostatic Dressing/AgentHemorrhage Controlled?YESApply CoTCCC-recommendedJunctional DeviceHead WoundsNeck WoundsJunctional WoundsAmenable to JunctionalDevice?Assess minimal bleeding after airwayand breathing managementNOYESNOHemorrhageControlled?Maintain Pressure with CoTCCCrecommended Hemostatic Dressing/Agent and Direct PressureIndicates All Combatantsand Combat Lifesavercapability level skillIndicates Combat Mediccapability level skillCONTINUE TACTICAL FIELD CARE10Indicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDAIRWAYIn accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Assess AirwayConscious with NOairway trauma orproblem identifiedUnconscious without AirwayObstructionAirway Obstruction orImpending Airway ObstructionChin Lift / Jaw Thrust ManeuverChin Lift / Jaw Thrust ManeuverInsert Nasopharyngeal AirwayInsert Nasopharyngeal AirwayIf able, allow casualty to assumeany position that best protects theairway, to include sitting up andleaning forward.Recovery PositionPerform SurgicalCricothyroidotomyUse lidocaine ifcasualty is conscious.NOPrevious AirwayProcedures Successful?CricKey Technique (preferred)ORBougie-assisted surgical techniqueYESORStandard open surgical techniqueAssess Respiration /BreathingSpinal stabilization is notnecessary for casualties withpenetrating trauma.CONTINUE TACTICAL FIELD CAREIndicates All Combatantsand Combat Lifesavercapability level skillIndicates Combat Mediccapability level skill11Indicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDIn accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017RESPIRATION / BREATHINGAssess Respiration /BreathingProgressive RespiratoryDistress and Known orSuspected Torso Trauma?NONOOpen/SuckingChest Wound?YESYESSuspect/Consider TensionPneumothoraxApply Vented Chest Seal to all open/sucking chest woundsNeedle Decompress Chest at Primaryor Alternate Site on injured side.Repeat as necessary.Vented chest seals arepreferred over non-vented.Initiate Pulse OximetryMonitoring if availableMONITOR FOR TENSIONPNEUMOTHORAXBurp or remove chest seal if applied.Repeat as necessary.YESTension PneumothoraxSuspected?Needle Decompress Chest atPrimary or Alternate Site if indicated.Repeat as necessary.TENSION PNEUMOTHORAX INDICATORS:Increasing HypoxiaRespiratory DistressHypotensionNOIf moderate or severe TBI is suspected, providesupplemental O2 if available to maintainSpO2 90%Indicates All Combatantsand Combat Lifesavercapability level skillDecompression Needle14-gauge, 3.25 inch needle/catheter unitPrimary Site:2nd Intercostal Space/Midclavicular lineCONTINUE TACTICAL FIELD CAREAlternate Site:4th or 5th Intercostal Space /Anterior Axillary Line12Indicates Combat Mediccapability level skillIndicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDCIRCULATION(BLEEDING)In accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Bleeding AssessmentPelvic Binder Indications- Severe blunt trauma orblast injury with one or more of the following:-Pelvic pain-Any major lower limb amputation/near amputation-Physical exam suggestive of pelvic fracture-Unconsciousness or ShockYESPelvic Binder indicated?Apply a Pelvic BinderNOReassess previously applied tourniquets.Reassess previously applied hemostaticdressings/agentsTourniquet not needed criteria:-Minor lacerations w/minimalbleeding-Surface Abrasions-Bleeding controlled by pressuredressingExpose wound anddetermine if tourniquet isneeded.NOEach hemostatic works differently. If onefails to control bleeding, it may beremoved and a fresh dressing of the sametype or a different type applied (Xstatcannot be removed in the field)Loosen tourniquet in 2 hours ifbleeding can be controlled byother means. Leave tourniquetloosely on limb for rapidreapplication if needed. Do notremove if TQ in place 6 hours.YESLeave previous tourniquet in placePlace second tourniquet 2-3 inchesabove wound on skin.Note time of tourniquetrelease on tourniquet and/orcasualty cardControl bleeding withhemostatic and/or pressuredressing.Loosen first tourniquet once secondtourniquet is effectively placedLeave tourniquet in place – maximum 2hours of tourniquet time untilreassessmentBefore 2 hours, reassess: if not in shock,able to monitor the wound closely forbleeding, and no amputation – controlbleeding with hemostatic and/or pressuredressing. Do not remove if TQ in place 6 hours.Note time of tourniquetrelease on tourniquet and/orcasualty cardIf needed, control bleedingwith hemostatic and/orpressure dressing.YESBleeding Controlled?NOMove original tourniquet to position nextto second tourniquet directly on skin andtighten both until bleeding stopped anddistal pulse not palpatedNote time of tourniquetreapplication on tourniquetand/or casualty cardIndicates All Combatantsand Combat Lifesavercapability level skillMonitor wound closelyfor bleedingIndicates Combat Mediccapability level skillCONTINUE TACTICAL FIELD CARE13Indicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDCIRCULATION(INTRAVENOUS ACCESS)In accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017IV/IO Indications:-In hemorrhagic shock or atsignificant risk of shock-Casualty needs IV/IOmedicationsNOIV access indicated?YESInitiate 18G IV or Saline LockIf IV is not obtainable, use IO routeCIRCULATION(TRANEXAMIC ACID)Administer 1 gm of Tranexamic Acid (TXA) in100 ml of NS or LR IV over 10minAdminister as soon as possible after injuryDo NOT administer 3hours after injuryYESTXA Needed?NOTXA Criteria:-Presents with Hemorrhagic Shock-One or more major amputations-Penetrating torso trauma-Evidence of severe bleedingAfter initial fluid resuscitation, administersecond dose of Tranexamic Acid (TXA) 1 gmin 100 ml of NS or LR IV over 10 minDo NOT administer 3 hours or more after injuryReassess frequently for presence of shockCONTINUE TACTICAL FIELD CAREIndicates All Combatantsand Combat Lifesavercapability level skillIndicates Combat Mediccapability level skill14Indicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDCIRCULATION(SHOCK / FLUID RESUSCITATION)In accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Assess for ShockShock Criteria:-Altered Mental Status (in absence of TBI)-Weak/Absent Radial PulseNOHemorrhagic shockpresent?If not in shock, NO IV fluids areimmediately necessaryYESFluid Resuscitation(in preferred order/combinations)Whole Blood TransfusionYESBlood ProductsAvailable?NOPO fluids permissible if casualty isconscious and can swallowHextend 500 ml bolusOR, if not availableOR, if not availablePlasma, RBCs, Platelets1:1:1OR, if not availableLactated Ringers 500 mlOR Plasma-Lyte A500 ml bolusPlasma and RBCs 1:1OR, if not availablePlasma (reconstituted,liquid, or thawed) orRBCsRe-assess after eachunit or 500 cc bolusadministeredContinue fluid resuscitation until:Palpable radial pulse ORImproved mental status ORSystolic BP of 80-90 mmHgFluid resuscitation and hypothermiaprevention should be executedsimultaneously if possibleIf altered mental status due to suspectedTBI and has weak/absent radial pulse,then resuscitate to restore normal radialpulse or Systolic BP 90mmHgAfter initial fluid resuscitation, administersecond dose of Tranexamic Acid (TXA) 1 gmin 100 ml of NS or LR IV over 10 minDo NOT administer 3 hours or more after injuryIf shock recurs, check allhemorrhage managementinterventions for effectiveness.Repeat fluid resuscitation.Reassess frequently for presence of shockIndicates All Combatantsand Combat Lifesavercapability level skillIndicates Combat Mediccapability level skillCONTINUE TACTICAL FIELD CARE15Indicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDHYPOTHERMIAPREVENTIONIn accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Minimize casualty environmental exposure / promote heat retentionKeep Personal Protection Equipment (PPE) on if feasible and warrantedReplace wet clothes if possibleUse CoTCCC recommended hypothermia prevention equipment if availableHypothermia prevention and fluidresuscitation should be executedsimultaneously if possibleUse dry blankets, poncho liner or sleeping bag. Keep casualty dry.Warm IV fluids are preferred if possiblePENETRATING EYETRAUMAPerform rapid field test of visualacuity and documentYESPenetrating Eye Traumanoted or suspected?Cover eye with Rigid Eye Shield(DO NOT use pressure patch)NOEnsure administration ofMoxfloxacin 400 mg from CombatWound Medication PackPatient MonitoringPatient monitoring should beinitiated as early as possiblePulse oximetry should be utilized as a minimum adjunct to clinicalmonitoring as stated in Breathing/Respiration section.Advanced non-invasive electronic monitoring and recording of vitalsigns should be initiated if possible and available.Indicates All Combatantsand Combat Lifesavercapability level skillCONTINUE TACTICAL FIELD CARE16Indicates Combat Mediccapability level skillIndicates CombatParamedic or SOF Mediccapability level skill
TACTICAL COMBAT CASUALTY CAREALGORITHMTACTICAL FIELD CARE CONTINUEDPAIN MANAGEMENT / ANALGESIAIn accordance withCoTCCC GuidelinesAs Of: 31 JAN 2017Mild to Moderate Pain(Casualty still able to fight)Assess PainModerate to Severe PainCasualties withmoderate tosevere pain arelikely not able tofight.Disarm casualtyAdminister Combat Wound Medication PackTylenol 650 mg bilayer caplet, 2 PO q8hMeloxicam 15 mg PO qdDocument Mental StatusYESAdminister Ketamine20 mg slow IV or IORepeat q20 min PRNORAdminister Ketamine50 mg IM or INRepeat q30 min PRNIs casualty in Shock orRespiratory Distress or atsignificant risk of developingeither?NOAdminister Oral Transmucosal Fentanyl Citrate(OTFC) 800 ugEND POINT:Control of pain or Nystagmus developmentMonitor Airway-Breathing-Circulationclosely. Be prepared to provideventilatory assistance.Consider Ondansetron 4 mg ODT/IV/IO/IM q8hPRN for nausea/vomitingAdd a second OTFC 800 ugin 15 min if neededEnsure Nalaxone (Narcan)available if administeringopioid analgesics.Administer 0.4 – 2 mg q 2-3min PRNReassess all pain management actions andcasualty reactionsANTIBIOTICSMoxifloxacin 400 mg PO qd(CWMP)NOYESPO Able?Ertapenem 1 gm IV/IM qdIndicates All Combatantsand Combat Lifesavercapability level skillEarly administration ofantiobiotics isrecommended for ALLopen combat woundsCONTINUE TACTICAL FIELD CARE17Indicates Com
TACTICAL COMBAT CASUALTY CARE (TCCC / TC3) ABBREVIATED TCCC GUIDELINES 31 JAN 2017 Return Fire and take cover Direct or expect casualty to remain engaged as a combatant if appropriate Direct casualty to m