Transcription
AcknowledgmentsThis publication was prepared by Kate M.Brett and Yinong Chong, under the generaldirection of Elsie Pamuk and Jennifer H.Madans. Computer assistance was obtainedfrom Yelena Gorina. General guidance on thecontent was obtained from Vivian Pinn andLoretta Finnegan of the Office for Research onWomen’s Health, National Institutes of Health.This publication was funded in part by the Officefor Research on Women’s Health, NIH.Copyright InformationAll materials appearing in this report are inthe public domain and may be reproducedor copied without permission. Citation as tosource, however, is appreciated.Suggested CitationBrett, KM, Chong Y. Hormone ReplacementTherapy: Knowledge and Use in the UnitedStates. Hyattsville, Maryland: National Centerfor Health Statistics. 2001.
In this ChartbookSummary.1of HighlightsOverviewWhy This Chartbook?.2Brief history of HRT use .2Chartbook methodology .3Patterns of HRT UseWhat percent of postmenopausal women use HRT, and in what forms?.4When do women begin HRT? .5For how long do women use HRT? .6Factors Associated with HRT UseHow does HRT use differ by menopausal type? .8How does a woman’s age and menopausal type relate to her HRT use?.9Which racial and ethnic groups are more likely to use HRT? . 10How does a woman’s educational level correlate with her HRT use?.11How does HRT use relate to family income? .12Characteristics of HRT UsersDo HRT users have healthier lifestyles and better health than non-HRT users? .14How do HRT users and nonusers differ in their rates of hypertension,high cholesterol, and diabetes?.15The Physician’s Role in HRT UseHow commonly and when do physicians counsel women about using HRT?.16How does education, race, and ethnicity affect a woman’s likelihood ofreceiving HRT counseling? .17Are women who receive preventive treatment more likely toreceive HRT counseling?.18What proportion of office or clinic visits include HRT prescriptions, bypatient’s age and race? .19What proportion of office or clinic visits include HRT prescriptions, bytype of physician and reason for visit? .20Technical NotesSources of data .22Definitions of terms used throughout this chartbook .24
Summary of HighlightsAlmost half of all postmenopausalwomen in the U.S. reported havingever used hormone replacement therapy(HRT). Pills were the most often usedHRT preparation (Figure 1).There are no substantial differencesbetween HRT users and nonusers in termsof risky health behaviors and self-reportedhealth (Figure 9).The prevalence of diabetes was twice ashigh among nonusers and past HRT usersthan among current users (Chart 10).Although most women started usingHRT around the time of menopause, 25%started taking it 5 or more years aftermenopause (Figure 2).Approximately 45% of women 40-60years of age reported receiving counselingfrom a physician about the pros and consassociated with using HRT after menopause (Figure 11).Among women who were at least 10years post-menopause, 14% had takenHRT pills at least 10 years (Figure 3).Women with surgical menopause weremuch more likely to have used HRT andwere more likely to be currently usingit compared to women with natural menopause (Figure 4).There was no difference in HRT usebetween age groups for women withnatural menopause. Ever use of HRTincreased with age through the 55-64year age group among women with surgical menopause (Figure 5).Non-Hispanic white women weremore likely to use HRT than either nonHispanic black or Mexican Americanwomen (Chart 6).Women with more than a highschool education or whose householdincome was above the poverty levelwere more likely to use HRT thanwomen with less education or lowerfamily income (Charts 7 and 8).White women were more likely toreceive HRT counseling than black or Hispanic women with the same level of education; women with higher levels of educationwere more likely to receive counseling thanwomen with less education, regardless ofrace or ethnicity (Figure 12).Women who had received recent preventive health services such as mammograms, Pap smears, and general examinations were much more likely to havereceived HRT counseling than those whohad not. The more recent the services,the greater the likelihood the women hadreceived HRT counseling (Figure 13).Of all ambulatory medical care visits bywomen 40 years of age and over, 7.5%included an HRT prescription (Figure 14).Obstetric/gynecology visits were 1.9times more likely to include an HRT prescription than visits to primary care physicians (Figure 15).Hormone Replacement Therapy: Summary of Highlights1
OverviewWhy This Chartbook?Brief history of HRT useWhile much has been written about therisks and benefits of hormone replacementtherapy (HRT), there is much less documentation of its actual use in the U.S.This chartbook offers researchers, healthcare professionals, and policy makers aninventory of information available aboutHRT use from recent nationally representative data collected by NCHS. The topicsinclude:The decrease in estrogen levels in womengoing through menopause has interesteddoctors and patients for many years. Synthetic estrogen was developed in the1920's, and by the mid-1930's it was beingused to relieve menopausal symptoms. Inthe mid-1960's, the book Feminine Forevertouted the use of synthetic estrogen as away to maintain youth and femininity. Thisbook became a hit in the lay press andgreatly increased the demand for HRT.The patterns of HRT useFactors associated with HRT useCharacteristics of HRT usersThe physician’s role in HRT useEach of the NCHS surveys used includedifferent information regarding HRTusage. Thus, the content of the survey dictated which data source to use to addressa particular question. Because one of thesurveys used collected data periodicallyrather than annually, use of the mostrecent data for each question did not resultin answers that all came from the sametime period.This chartbook is not intended to be aguide on whether or not to use HRT, sincethat decision must be made by each individual women with help from her physician. However, this overview of HRTprescription and use in the United Stateswill be helpful to researchers and policymakers working in the arena of women’shealth.2Hormone Replacement Therapy: OverviewHRT use decreased sharply when the connection between use of synthetic estrogenand elevated risk of endometrial cancer wasrecognized in the 1970’s. Use of HRT hasslowly gone up since the 1980’s, whenlong-term research established the protective effects of HRT against osteoporosisand possibly heart disease.Improved treatment schedules and deliverysystems have increased HRT use in theU.S. To minimize the risk of endometrialcancer, physicians are much more likely togive lower doses of estrogen and to combine it with progesterone for women whoseuteruses are intact. Furthermore, many different formulations and dosing schedulesnow permit physicians to better tailor HRTto each patient.Although we know much more about HRTtoday, controversy still surround its risksand benefits. Those who caution againstusing HRT use often cite the increasedrisk of endometrial and breast cancerassociated with using estrogen, especiallyfor extended lengths of time, and its
common side effects such as breast tenderness, nausea, unpredictable bleeding,bloating, and mood fluctuations. Thosewho advocate using HRT frequentlypoint out that HRT appears not only toalleviate menopausal symptoms, but alsoto reduce the risk of osteoporosis, andpossibly heart disease and Alzheimer’sdisease, all of which could have muchgreater impact than cancers on the healthof postmenopausal women.Until we have more definitive information about HRT’s effects on diseases,each woman must, with the help of herphysician, weigh the risks and benefitsof use. Whether or not a woman usesHRT depends on many factors: how sheperceives the risks and benefits of HRTvs. the risks and potential harm of menopausal symptoms and various diseasesaffected by HRT; the information sheobtains from her physician about HRT;and her access to health care.Chartbook methodologyThe data in this chartbook came fromnationally-representative surveys:The Third National Health andNutrition Examination Survey(NHANES III), 1988-1994;The National Health InterviewSurvey (NHIS), 1998; andThe National AmbulatoryMedical Care Survey (NAMCS)and National Hospital AmbulatoryMedical Care Survey(NHAMCS),1997-1998.Details about each of these surveys arein the Technical Notes section of thischartbook. Some of the terms used inthis report have specific technical definitions. The definitions are also listed inthe technical information section.Statistical tests have been made to assesswhether observed differences are dueto the random variation introduced byobtaining information on a sample ratherthan the total population. If a differenceis described in the text of this chartbook,it has been found to be statistically significant.Hormone Replacement Therapy: Overview3
Patterns of HRT UseThis section focuses on patterns of HRT use among postmenopausal women. Topicsexplored include the proportion of women who currently and previously used HRT, whenHRT was initiated relative to age at menopause, and for how long women have used HRT.The data used was obtained between 1988 and 1994 from the Third National Health andNutrition Examination Survey (NHANES III).Peri-menopausal women, even if they used HRT, are not included in these analysesdue to the way HRT information was collected in the NHANES survey. As a result, theestimates of total use might be lower than those found in other studies.What percent of postmenapausal women use HRT, and in what forms?NHANES III (1988-94) data indicatethat overall, 44% of postmenopausalwomen reported having ever used femalehormone pills, vaginal cream, suppository,injection, or skin patches, and some womenused more than one form of hormone preparation simultaneously or sequentially1.Pills were the most popular type of hormone preparation (40% of postmenopausalwomen), followed by cream/suppository/injection2 (10%), and then by patches (4%).Among women who ever used pills,4Hormone Replacement Therapy: Patterns of HRT Useabout 50% were still using them at thetime of interview. Among women whoever used hormone cream, injections orsuppositories, 32% were still using thoseforms of HRT. Among women who everused HRT patches, 30% remained currents users.Among current users, 93% were usingpills, 26% were using hormone cream,injections or suppositories, and 15% wereusing patches. Thirty one percent (31%)were using two or more forms of HRTconcurrently (data not shown).
When do women begin using HRT?Among postmenopausal women whohad ever used HRT: 17% started this therapy beforethey experienced naturalorsurgical menopause, 48% started this therapy withina year after menopause, 10% started 2-4 years aftermenopause, and 25% started 5 or more years aftermenopause.Hormone Replacement Therapy: Patterns of HRT Use5
For how long do women use HRT?To better investigate duration ofuse, the analysis was limited to womenwho are at least 10 years beyond menopause. Some women started to useHRT during the perimenopausal period,and thus use before the actual onset ofmenopause is included when calculating duration of use.Among women who were 10 or moreyears beyond menopause, 39% had everused HRT in pill form3 (data not shown).6Hormone Replacement Therapy: Patterns of HRT UseIn this population: 24% took HRT pills for less thanone year, 34% took HRT pills for 1-5 years, 6% took it for 6-9 years, and 37% took it at least 10 years.The sooner women start to take HRTsafter menopause, the more likely they areto use for a longer period. For example,of the 56% of women who were 10or more years beyond menopause andwho started taking HRT either before orwithin 2 years of menopause, 50% took itfor at least 10 years (data not shown).
Footnotes for this section:Since women can take more than one preparation, the sum of the different formulations will be greater than thepercent of women using any formulation.1While these methods of hormone administration are distinct, thet were combined into a single question in theNHANES III interview, and thus are reported together.2Because the survey did not collect information on the exact dates when each different form of HRT was begunand stopped, we cannot differentiate women who has used several forms of hormones at the time and those whohad used different forms at different times. Thus, we focus on pill use here, which was the form used by themajority of women.3Hormone Replacement Therapy: Patterns of HRT Use7
Factors Associated with HRT UseIt is currently recommended that each individual woman should decide whether touse HRT after considering, in concert with her health care provider, such factors asfamily history of breast cancer, osteoporosis, heart disease, and the potential benefitsof HRT against these diseases, as well as her willingness to accept the risks and sideeffects of HRT.The charts in this section examine individual characteristics associated with HRT,including menopausal type, age, race and ethnicity, education, and income.How does HRT use differ by menopausal type?Women with surgical menopausewere much more likely to use HRT thanwomen with natural menopause. Amongwomen with surgical menopause, 75% ofwomen who had both ovaries removedhad used HRT at some time, while 50%of those with a hysterectomy only hadever used HRT. Only 30% of womenwith natural menopause had used HRT.8Women with surgical menopause werenot only more likely than women withnatural menopause to have ever usedHRT, but also were more likely to be current HRT users. Of those who had bothovaries removed, 50% were still usingHRT (two thirds of the ever users). Ofthe women who had a hysterectomy buthad at least one remaining ovary, 24%were still using HRT (one half of theever users). Among naturally menopausalwomen, 11% were still using HRT (onethird of ever users).Hormone Replacement Therapy: Factors Associated with HRT Use
How does a woman’s age and menopausal status relate to her HRT use?Differences in the use of HRT byage were highly related to type ofmenopause.Among women who had a naturalmenopause, there was almost no difference by age in ever use of HRT. Women65 years of age and over were less likelyto be currently using HRT than youngerwomen, but they were more likely tohave formerly used HRT.Among women who had undergone asurgical menopause, ever use increasedwith age until the oldest age group. Compared to women less than 45 years ofage, women 45-54 were 34% more likelyto have used HRT, and women 55-64were 45% more likely to have used HRT.There was no significant difference in useof HRT among surgically menopausalwomen less than 45 years of age compared to women 65 years of age and over.Patterns in HRT use by age reflectwomen’s age at menopause, their currentage relative to their age at menopause,and the year during which they underwent menopause. It is not possible to discern which of these effects are influencing HRT use as seen in this chart.Hormone Replacement Therapy: Factors Associated with HRT Use9
Which racial and ethnic groups are more likely to use HRT?Non-Hispanic white women weremore likely to have ever used HRT thannon-Hispanic black or Mexican-American women, with the largest disparitybetween whites and blacks. HRT use fornaturally menopausal white women was80% higher than that for naturally menopausal blacks, and 69% higher than thatfor naturally menopausal Mexican-Americans. Surgically menopausal whites were83% more likely than surgically menopausal blacks, and 46% more likely thansurgically menopausal Mexican-Americans to have ever used HRT.10Current use of HRT was also highestamong non-Hispanic white women compared with either non-Hispanic blacksor Mexican-Americans. Naturally menopausal whites were 1.3 time more likelythan naturally menopausal blacks, and 2.6times more likely than naturally menopausal Mexican-Americans to be currentHRT users. White women with surgicalmenopause was 1.6 times more likelythan surgically menopausal blacks, and43% more likely than surgical menopausalMexican-Americans to be current HRTusers.Hormone Replacement Therapy: Factors Associated with HRT Use
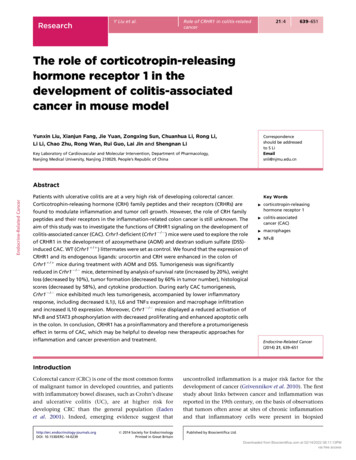
How does a woman’s educational level correlate with her HRT use?The more educated a menopausalwoman, the more likely she was tohave ever used HRT. HRT use for naturally menopausal women with beyondhigh school education was 35% higherthan naturally menopausal women with12 years education, and 44% higherthan naturally menopausal women withfewer than 12 years of education. HRTuse for surgically menopausal womenwith beyond high school education was36% higher than surgically menopausalwomen with fewer than 12 years ofeducation.Education was also related to current use of HRT, especially for womenwith natural menopause. Among naturally menopausal women, current HRTuse for women with beyond highschool education was 23% higher thanthat for women with high school education, and 180% higher than that forwomen with below a high school education. For women with surgical menopause, current HRT use for those withbeyond high school education was 30%higher than for those with only a highschool education and 83% higher thanfor those who had not completed highschool.Hormone Replacement Therapy: Factors Associated with HRT Use11
How does HRT use relate to family income?Menopausal women whose familyincome was above the poverty levelwere much more likely to have everused HRT. Naturally menopausalwomen above the poverty level were33% more likely to have ever usedHRT than those living at or below thepoverty level. Surgically menopausalwomen above the poverty level were67% more likely to have ever usedHRT than those living at or below poverty level.12Current HRT use was strongly correlated with income level. Naturallymenopausal women above the povertylevel were 4.5 times more likely to becurrent users than women below thepoverty level. Surgically menopausalwomen above the poverty level werealmost twice as likely to be currentHRT users than those below the poverty level.Hormone Replacement Therapy: Factors Associated with HRT Use
Hormone Replacement Therapy: Factors Associated with HRT Use13
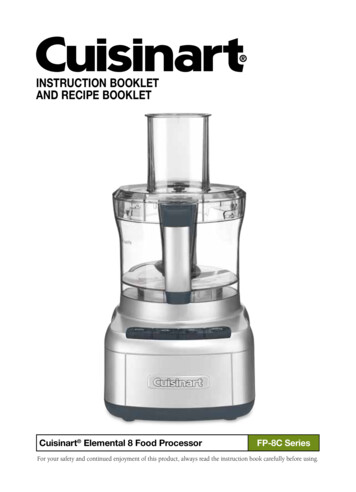
Characteristics of HRT UsersThis section compares HRT users and never users on selected characteristics. Theattributes analyzed are selected health risk behavior and perceived health status, andrates of hypertension, elevated cholesterol, and diabetes. The objective is to see whetherHRT users have healthier lifestyles and better health.Do HRT users have healthier lifestyles and better health than nonusers?Current HRT users were just aslikely to be a current or former smokeras nonusers, but former HRT users(55%) were more likely to be current orformer smokers than nonusers (46%).Current HRT users (22%) were lesslikely to report sedentary lifestyle thannonusers (37%), but past HRT users(38%) showed no difference from nonusers.Both current (82%) and formerusers (82%) were more likely toreported moderate or heavy drinkingthan nonusers (72%).Current HRT users (19%) were lesslikely to report fair or poor health thannonusers (27%), but past users (28%)show no difference from nonusers inperceived health status.14Hormone Replacement Therapy: Characteristics of HRT Use
How do HRT users and nonusers differ in their rates of hypertension,high cholesterol, and diabetes?HRT users and nonusers did notdiffer substantially in their rates ofhypertension.Elevated serum cholesterol was morecommon among former HRT users (42%)than among current HRT users (35%) andnonusers (36%).Diabetes was more than twice asprevalent among former HRT users(14%) and nonusers (15%) as it wasamong current HRT users (6%).Hormone Replacement Therapy: Characteristics of HRT Use15
The Physician’s Role in HRT UseMany women receive information about HRT from their physicians. How and whetherphysicians discuss HRT with their patients is an important determinant of whether womenuse HRT.In 1992, the American College of Physicians recommended that physicians discuss HRTwith all women around the time of menopause. The first three figures in this section describefactors related to counseling among women 40-60 years of age, the years when menopause ismost likely to occur. It is not limited to postmenopausal women, as that information was notavailable. These data were collected in the National Health Interview Survey from interviewswith women rather than with their physicians. Therefore, responses of not receiving HRTcounseling could mean women did not receive this counseling or it could mean that they didnot remember being counseled.How commonly and when do physicians counsel women about using HRT?In 1998, approximately 45% ofwomen 40-60 years of age reportedreceiving counseling from a physicianabout the pros and cons associated withusing HRT after menopause.Age was a factor in who received HRTcounseling. Only 19% of women 40-44had ever received physician counseling on16HRT use, compared with 41% of women45-49 years of age, 63% of women 50-54,and 67% of women 55-60.Information about preventing boneloss was included in a significant proportion of HRT counseling. Of the womenwho received HRT counseling, 89% hadreceived information about the effect ofHRT on bone loss during the counseling.Hormone Replacement Therapy: The Physician’s Role in HRT Use
How does education, race, and ethnicity affect a woman’s likelihood of receivingHRT counseling?The higher a woman’s educational level,the more likely she was to have been counseled about HRT. In 1998, 47% of women40-60 years of age who had finished atleast one year of college were counseledby a physician about using HRT after menopause. In contrast, among women with lessthan a high school education, only 34% werecounseled about HRT.Non-Hispanic white women were 54%more likely than non-Hispanic black womento receive HRT counseling at some point inthe past. Non-Hispanic white women werealso 62% more likely than Hispanic womento have received HRT counseling.The disparity of HRT physician counseling by race is consistent with findings inFigure 6 that race affects the probability ofusing HRT; white women are much morelikely to take HRT than black women.Use of HRT varies by socioeconomicstatus, with the most educated and wealthiest women having the highest probability ofuse. The differences in HRT use by incomeand education may be due partly to differences in the information women receivefrom their physicians.Hormone Replacement Therapy: The Physician’s Role in HRT Use17
Are women who receive recent preventive treatments more likely toreceive HRT counseling?Women 40-60 years of age who hadreceived a mammogram within the last twoyears were 2.3 times more likely to havebeen counseled about HRT by a physicianthan women who had never had a mammogram and 45% time more likely to becounseled about HRT than women whohad received a mammogram more than twoyears ago.18A similar association was foundbetween the time since the last Pap smeartest and HRT counseling. Women whoreceived a Pap test within the last yearwere almost 3 times more likely to havereceived HRT counseling than women whohad never had a Pap test. Women whoselast Pap test was 1-3 years ago were 2.0times more likely and women who whoselast test was more than 3 years prior were1.3 times more likely to have received HRTcounseling than women who had never hada Pap test.Hormone Replacement Therapy: The Physician’s Role in HRT Use
Another way to look at national HRT use patterns is to investigate the proportion of medicalcare visits during which HRT is ordered, administered, or provided by the physician. Suchan analysis does not measure use, but does describe the types of visits associated with HRTprescriptions and the types of physicians who are more likely to prescribe HRT.In the following two figures, the unit of analysis is the physician visit rather than thewoman. A woman may have more than one visit to a physician or may visit more thanone physician. The analysis can only tell what proportion of total visits will include HRTprescriptions. Women 40 years of age and over are included.What proportion of of ce or clinic visits include HRT prescriptions, by patient’s ageand race?Overall, 7.5% of all visits by women 40years of age and over to office-based physicians and hospital out-patient departmentsincluded a prescription for HRT.The proportion of physician or clinicvisits that included an HRT prescriptionwas strongly associated with age. About5% of all visits by women 40-49 yearsof age included HRT prescriptions, while12% of visits by women 50-59 years of ageand 9% of visits by women 60-69 yearsof age included an HRT prescription. Only2% of all visits by women 80 years of ageand over included an HRT prescription.Visits to physicians and hospital outpatient clinics by white women were 40%more like to include an HRT prescriptionas visits by black women, after age-adjustment.Hormone Replacement Therapy: The Physician’s Role in HRT Use19
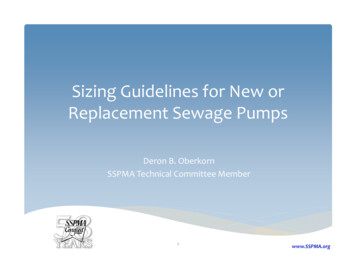
What proportion of of ce or clinic visits include HRT prescriptions, by type of physician and reason for visit?Physician or clinic specialty wasstrongly associated with whether HRT wasprescribed. Visits by women 40 years ofage and over to obstetric and gynecologyphysicians and clinics were 1.9 times morelikely to include an HRT prescription thanvisits to primary care physicians and clinics.Only 8.8% of visits to primary carephysicians and clinics (general, family, andinternal medicine) included an HRT prescription, compared with 25.6% of visits toobstetrics/gynecology physicians and clinics, and 2.7% of visits to all other typesof physicians and clinics (e.g., surgery andcardiology).Although visits to primary care physi-20cians and clinics were less likely to includean HRT prescription than visits to obstetricor gynecology physicians and clinics, visitsto primary care physicians and clinicsaccounted for 57% of all visits in whichHRT was prescribed. This is because primary care physicians and clinics accountedfor a much larger total number of visitsthan did obstetrician and gynecologist physicians and clinics.HRT was more likely to be prescribedduring visits that were initiated by thepatient at least partly because of menopausal complaints or that involved a diagnosis of menopausal or post-menopausalsymptoms. Just over one half of all suchvisits to primary care physicians andobstetric/gynecology specialists and clinicsincluded HRT prescriptions.Hormone Replacement Therapy: The Physician’s Role in HRT Use
Hormone Replacement Therapy: The Physician’s Role in HRT Use21
Technical NotesSources of dataNational Health and Nutrition Examination Survey (NHANES III)The third National Health and NutritionExamination Survey (NHANES III) wasa cross-sectional survey conductedbetween 1988 and 1994 by the NationalCenter for Health Statistics. It selecteda representative sample of the noninstitutionalized U.S. population ages 2months and older. The data were collected through both face-to-face interviews and standardized physical examinations. Mexican Americans, AfricanAmericans, and persons 60 years of ageand older were over sampled to providemore reliable estimates for these subpopulations. NHANES III collected information from women aged 17 years andolder on use of non-contraceptive femalehormones without differentiating whetherthe hormones contained estrogen or progesterone. The response rate for the questionnaire in which HRT information wascollected was 78%.Information on women’s use of HRTbegan to be collected again in NHANES1999. The questions included in the newsurvey will provide more detail regardingthe formulation used and the time of initiation. This data will not be available forpublication until at least 2003, due to precision considerations.For more information on the NHANES22Hormone Replacement Therapy: Technical NotesNational Health Interview Survey(NHIS)The National Health Interview Survey(NHIS) is a continuing nationwide samplesurvey in which data are collected throughpersonal household interviews. Informationis obtained on personal and demographiccharacteristics including race and ethnicityby self-report or as reported by an informant. Information on HRT was obtained ina special section regarding health prevention in adults included during the 1998 calendar year.The response rate for household selectedto participate in the 1998 NHIS was 90%.When taking into account t
way to maintain youth and femininity. This book became a hit in the lay press and greatly increased the demand for HRT. HRT use decreased sharply when the con-nection between use of synthetic estrogen and elevated risk of endometrial cancer was recognized in the 1970’s. Use of HRT h