Transcription
Alameda Alliance for HealthCalOptimaCalViva HealthCenCal HealthCentral CA Alliance for HealthCommunity Health GroupContra Costa Health PlanGold Coast Health PlanHealth Plan of San JoaquinHealth Plan of San MateoInland Empire Health PlanKern Health SystemsL.A. Care Health PlanPartnership HealthPlan of CASan Francisco Health PlanSanta Clara Family Health PlanCalifornia’s LocalHealth Plans:A Panoramic ViewWelcome & IntroductionsAmber McEwenDirector, Programs & Strategic ProjectsLocal Health Plans of California21
FacultyBrianna Lierman is chief executive officer of LocalHealth Plans of California and has more than a decade ofexperience in health care. Previously, she was a foundingexecutive and vice president of government affairs, andcompliance officer for a Medi-Cal Managed Care plan,where she was responsible for county and stategovernment affairs, and advocacy with the executive andlegislative branch. Prior to that, Brianna was in privatepractice as a lobbyist and advising clients in the areas ofKnox-Keene and Medi-Cal managed care. Brianna is amember of the State Bar of California.3FacultyBobbie Wunsch is a partner with the Pacific HealthConsulting Group. Ms. Wunsch has more than 30 years ofexperience in the health care industry and specializes inthe restructuring and financing of health care deliveryorganizations. She provides strategic planning services tocommunity clinics, county health and local Medicaidmanaged care organizations, and various other healthcare organizations. She focuses on a variety of issues,including restructuring through mergers or affiliations,program development, redesigns for improvedeffectiveness and efficiency, and cooperative businessventures.42
FacultyChristopher Perrone is director of the CaliforniaHealth Care Foundation’s Improving Access team,which works to improve access to coverage and carefor low-income Californians. He was previouslydirector of the foundation’s Health Reform and PublicPrograms initiative, where he led efforts to improvethe policies and practices that shape Medi-Cal andother publicly funded health care programs, and topromote greater transparency and accountabilitywithin these programs.5Agenda Overview and Context History of the Local Plan Model Role of Local Plans in Managed Care Current and Future Challenges for LocalHealth Plans63
Brianna LiermanOverview & ContextCalifornia’s Medicaid Program84
Understanding Local Plans’ RoleMedi-Cal Program Nearly 1 in 3 Californians arecovered by Medi-Cal.Medi-Cal Enrollment 83% (10.6M) beneficiaries areenrolled in Medi-Cal ManagedCare. 25 health plans contract withCA Department of Health CareServices for the Medi-CalManaged Care program.o16 plans are local plans.9More Perspectives on Local Plans All 16 community-based andnot-for-profit– First and largest of our kind inthe nation Publicly operated and governed– Largest publicly accountabledelivery system in nation Cover 70% of the 10.6Mbeneficiaries in Medi-CalManaged Care 80% of Medi-Cal beneficiariesselect the local plan whenoption available105
Bobbie WunschHistory of the Local Plan ModelOverview Who and where are the local health plans? Origins of the plans– Models and phases of Medi-Cal managed care– Definitions of local health plans– Origins: COHS– Origins: Local Initiatives– Origins: Community Health Group (CHG)– Authorizing Legislation Providing coverage beyond Medi-Cal Differences from commercial plans126
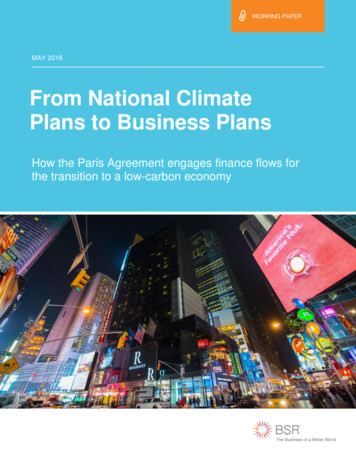
Where are the Local Plans?Local — Headquartered incommunities and Statewide — But covernearly entire state13Six Models of Medi-Cal Managed Care1.County Organized HealthSystem (COHS)2.Two-Plan Modela.One Local Initiative (LI) Planb.One Commercial Plan3.Geographic Managed Care(GMC)4.Rural Managed Care/Regional Model5.Imperial Model6.San Benito147
Phases of Medi-Cal Managed Care Prepaid Health Plans (PHPs)Primary Care Case Management (PCCM)COHSState Plan for Two-Plan Model and GMCRural Expansion — Phase 1Rural Expansion/Regional Model — Phase 2Imperial ModelSan Benito Approach15California’s Local Health Plans andWhen They BeganCOHSLocal Initiatives CalOptima (1995) Alameda Alliance for Health (1996) CenCal (1983) CalViva Health (2009) Central California Alliance for Health(1996) Community Health Group (1985) Gold Coast Health Plan (2011) Contra Costa Health Plan (1973) Health Plan of San Mateo (1987) Health Plan of San Joaquin (1996) Inland Empire Health Plan (1996) Partnership HealthPlan of California(1994) Kern Health Systems (1996) L.A. Care Health Plan (1997) San Francisco Health Plan (1996) Santa Clara Family Health Plan (1997)168
Who Are Local Health Plans: Definition6 County Organized Health Systems (COHS), 9 Local Initiatives (LIs) and1 community-based non-profit* plan are recognized as California’s local health plans.*What makes local plans “local?” Established by its community to serve the health care needs of underservedpopulations Formed pursuant to state or federal statute as a public agency, independent of theCounty (exception Contra Costa Health Plan) Formed through local ordinance(s) (or joint powers agreements) of one or moreBoard(s) of Supervisors Governed by a commission whose membership is prescribed in the ordinance(s)(or statute) Subject to California’s Fair Political Practices Law and Ralph M. Brown Open MeetingLaw (“Brown Act”) Operate a health plan that contracts principally with public payors* Community Health Group (CHG) is also a local health plan, but is not a public COHS or LI. It is a community-based, nonprofitplan started by a community health center that shares the same mission as other local plans.17Plan Origins: COHS &Local Community Control Publicly sponsored health plans came to life in theearly 1980s. County executives in Monterey and Santa Barbarasuggested a novel, local, public and private partnershipto reform Medi-Cal. San Mateo followed. The next wave was the addition of Solano, Orange andSanta Cruz counties in the 1990s. In the years that followed, several of the COHSexpanded into nearby counties.189
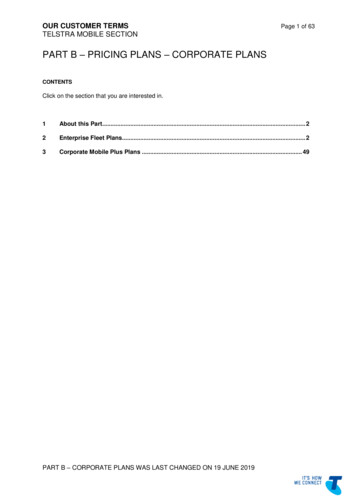
COHS: Local Control toAddress Local Issues Strategy: Take control of Medi-Cal from state and federalbureaucracies and run it like a health plan, but one that was publiclyaccountable. Santa Barbara, Monterey, Santa Cruz and Ventura had accessproblems they wanted to address. San Mateo wanted to improve access, but also bring care back intotheir county that was leaking out to neighboring counties. Solano and Orange counties’ COHS evolved from communityprojects to address indigent populations and the uninsured. Merced County got COHS designation, but instead joined CentralCalifornia Alliance for Health.19Six COHS Plans Serving 22 Counties2010
Plan Origins: Local InitiativesProtect the Safety NetState Plan for Medi-Cal Managed Care developed underDirector Molly Coye in 1992-93: Political and legislative challenges of creating more COHSplans required DHCS to develop an additional model if thestate was to move toward greater managed careenrollment. DHCS’ decision to move to mandatory enrollment inmanaged care in some counties piqued the interest ofcommercial plans, which recognized that they would havereduced marketing costs in a mandatory environment.21Plan Origins: Local InitiativesProtect the Safety NetState Plan for Medi-Cal Managed Care developed underDirector Molly Coye in 1992-93 (cont.): At the same time, county health and hospital systems, and othersafety-net providers feared that to the extent commercial plansparticipated in Medi-Cal, they would seek to enroll only thehealthier beneficiaries, putting the safety net at risk. County hospitals pressured DHCS to address these concernswith a radical new plan that attempted to both protect the safetynet and spread the cost savings anticipated from managed caremore widely by incorporating a local community plan based onthe COHS model, and having it compete with a commercial plan.This became known as the Two-Plan Model.2211
Local Initiative Creation All counties who are LIs have county hospitals, exceptStanislaus, Tulare and Fresno.–––They initially had two commercial plans.Fresno transitioned later to LI – CalViva.Stanislaus contracts with Health Plan of San Joaquin. Alameda and San Joaquin were first two LIs to go live. Later transitions to managed care suggested that Fresno,Merced, Madera and Kings become GMC instead.––Merced became COHS; eventually joined Central CaliforniaAlliance for Health.Fresno, Kings and Madera became CalViva and contracted forsome administrative services with Health Net.23Nine Local Initiatives Serving 13 Counties2412
Origin of Community Health Group (CHG) 1982: CHG was created by San Ysidro Health Center –one of three community health centers in California to createa separate health plan 1983: Obtained first contract with state as Primary Care CaseManagement (PCCM) 1984: Obtained contract with San Diego County for indigentcare 1985: Knox-Keene license 1993: Separated from San Ysidro Health Center asGMC began Only non-public local health plan25Authorizing LegislationFederal Legislation and Limits for COHS Federal statutes limit the number of COHS in California andplace a ceiling on the percentage of Medi-Cal beneficiaries inthe state that can be enrolled in COHS plans. Section9517(c)(3) of the Consolidated Omnibus Budget ReconciliationAct of 1985 (42 U.S.C. 1396 b note) and as amended.State Legislation and Local Ordinances for LIs Welfare and Institutions Code Section 14087.38 allows countiesto create a Local Initiative. The section is generic for use by anycounty. Some counties created their own unique section. To activate the LI, the County Board of Supervisors must pass acounty ordinance.2613
Providing Coverage Beyond Medi-CalLHPC plans have provided a wide variety of insurance productsand health programs to meet the needs of their communitiesbeyond Medi-Cal: Healthy FamiliesIn-Home Supportive Services Workers (IHSS)Healthy KidsAIM (Access for Infants and Mothers)County employeesCounty indigents and/or Coverage InitiativeMedicare Special Needs PlanDuals Demonstration (Cal MediConnect)Covered California27Key Differences From Commercial Plans Mission emphasis on safety net Public, nonprofit agencies Local, easy to access County ordinance enables plan creation/continuation Community-based governance Vast majority of work focused on low-income populations withMedi-Cal and health disparities Community asset2814
Chris PerroneHow Are California’s Local PlansUnique?29Overview Role of Local Plans in Medi-Cal Market Medi-Cal Enrollee Experiences: Access andQuality Local Plan Investments in the Safety Net andin Their Communities A Few Challenges Facing Medi-Cal andManaged Care3015
Most Medi-Cal Enrollees Get CareThrough Managed Care20132018Total 8.6 MTotal 13.2 MFFS18%ManagedCare59%FFS41%Managed Care82%31Most Managed Care Enrollees GetCare From a Local Plan20132018Total 5.1 MTotal 10.8 MCommercial31%Commercial29%Local71%Local69%3216
Medi-Cal Managed Care Enrollmentby Plan 24GMC1,149,478RegionalImperial/San BenitoTOTAL298,36184,54410,839,876Source: DHCS, Medi-Cal Managed Care EnrollmentReports, July 201833Local Plan Enrollment — 2018L.A. 72,213Alameda259,096Kern255,070Santa ClaraGold Coast249,439197,684CCHP180,401CenCal177,079San FranciscoSan Mateo128,613107,8103417
Local Plan Market Share — 2018CalOptima100%CenCal100%CCAH100%CCHP100%Gold Coast100%HPSM100%Partnership100%IEHP89%San Francisco87%Alameda81%HPSJ80%Kern78%Santa Clara78%CalViva71%L.A. CareCHG68%38%35Most Medi-Cal Enrollees, Public HavePositive View of Medi-CalBeneficiary Perceptions of Medi-CalPublic Perceptions of Medi-CalHow important is Medi-Cal to the state?Not too4%Not at all No response3%2%Somewhat17%Very74%Source: Berkeley IGS Poll, 201718
Access to Care For Adult Medi-Cal Enrollees is GenerallyComparable to Individual Market, Better Than UninsuredHas Usual Source of Care90%85%84%52%Employer IndividualDoctor's OfficeMedi-Cal UninsuredClinicOtherVisited Doctor Within Past Year85%77%80%56%EmployerIndividual1 visitMedi-Cal2 visits Adults with Medi-Cal are 40%more likely to receive routinecheck-ups than uninsured. Children with Medi-Cal are twiceas likely to receive routinepreventive and dental care thanuninsured children. Women with Medi-Cal are 24%more likely to receive amammogram than uninsured. 1 in 3 Californians struggling withmental health or substance abusehave Medi-Cal.UninsuredSource: California Health Interview Survey (CHIS), 2016.Higher ED Use Among Adult Medi-CalEnrollees Reflects Population DifferencesVisited ED, Fair or Poor HealthVisited ED in Past lUninsuredVisited ED, Fair or Poor Health, andNo Long-Term e: California Health Interview Survey (CHIS). Pooled 2015 and 2016 data for non-elderly adults.19
Large Majorities of Most Local Plan MembersSay They Get Care QuicklyGetting Care Quickly – Percent of Plans by Member 0-69%70-79%80-89%Source: DHCS, Medi-Cal Managed Care External Quality Review Technical Report, July 1, 2016-June 30, 2017 (April 2018).39Health Plan Total Quality ScoreIn two-plan counties, which plan performs better?LocalCommercialSource: DHCS Medi-Cal Managed Care Performance Dashboard, June 27, 2018 release.4020
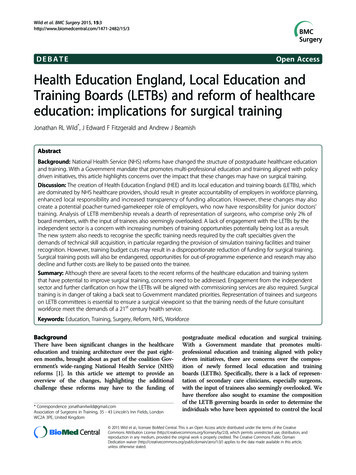
Safety Net Clinics Are Important Providers forPublic Plans, Especially in the North41Growing Role of Safety Net Clinicsin Local Plans Shared history Auto-assignment algorithm favors plans that rely moreon safety net providers for primary care. Medi-Cal payment policies have driven greaterdependence on Federally Qualified Health Centers(FQHCs) over time.4221
Public Plan Investments in the Safety Net Program grants for new services,improve chronic care, improvepatient experience, improve timelyaccess, reduce avoidableadmissions Grants to purchase equipment,recruit and retain providers, supportloan repayment Quality incentive payments targetedto meet HEDIS benchmarks insafety net“Public plans were farmore likely thancommercial plans to makeinvestments in safety netclinics and were morelikely to pair payments withtechnical assistance .Public plans provided farlarger levels of supporttargeted to expand accessand implement practiceimprovements withinsafety net clinics.”Source: Pacific Health ConsultingGroup, Medi-Cal Managed Care Plansand Safety Net Clinics Under the ACA(CHCF, 2015).Examples of Public Plan Investments Central California Alliance for Health’s Provider RecruitmentProgram made 20 million available to subsidizerecruitment-related expenses for primary care, specialty careand behavioral health professionals.1 Inland Empire Health Plan is investing in a 20 millioninitiative to integrate behavioral health care at the point ofcare with 13 entities across 34 sites.1 Partnership HealthPlan and L.A. Care are investing 25 million and 20 million, respectively, in grants to expandhousing in their communities.1ManattHealth, Moving Medi-Cal Forward on the Path to Delivery System Transformation (CHCF, 2016).4422
Current Plan Investments in SocialDeterminants of Health (SDOH)Housing Instability77%Lack of Transportation69%Food Insecurity62%Social Isolation54%Language Barriers54%Environmental Exposures46%Economic Insecurity46%Community Violence/Safety38%Adverse Childhood Experiences38%Incarceration/Justice System 38%Legal Barriers/Immigration Status31%Educational Deficits23%Intimate Partner Violence15%Racial Injustice/Discrimination15%Don't knowNo such activitiesAll plans reported investing in at leastone SDOH within the last 12 months.The majority of plans are currentlyinvesting in housing instability, lack oftransportation and food insecurity.Prepared by JSI Research & Training Institute, Inc. with support from Blue Shield of California Foundation45Physician Participation in Medi-Cal is Insufficient,Has Not Kept Pace with Enrollment GrowthSource: J. Coffman and M. Fix, Physician Participation in Medi-Cal: Is Supply Meeting Demand? (CHCF, 2017).23
Quality of Care in Medi-Cal Managed Care is Similar to NationalMedicaid Average, But Has Not Consistently Improved Over TimeCervical Cancer ScreeningDiabetes Care – 8%56%Timely Prenatal Care83%83%High Blood Pressure Control77%75%74%71%71%61%63%61%57%Well Child Visit – Ages 3-6Child Immunization Status82%56%75%70%73%73%71%74%72%Source: Managed Care Quality and Monitoring Division, Medi-Cal data reflects reporting year (RY) 2016-17. National average reflects RY 2015-16.Significant Disparities in Care RemainAmong Medi-Cal EnrolleesPreventable Hospitalizations,by Race/Ethnicity* (2011)Difficulty Finding Specialty Care,by Health Status (2016)36%1,91224%1,04616%727LatinoOther WhiteAfrican AmericanExcellentVG/Good/FairPoorDifficulty Finding Specialty Care,by Region (2015-16)Difficulty Finding Specialty Care,by Disability ilitySources: J. Watkins and J. Chen, Preventable Hospitalizations in Medi-Cal: Rates of Hospitalization for Ambulatory Care Sensitive Conditions in 2011 (DHCS,2015). Excludes children, seniors and persons with disabilities. California Health Interview Survey, 2016 and 2015-16 pooled. Non-elderly adults with Medi-Cal only.24
Current & Future Challenges forLocal Health Plans49Thank You!Local Health Plans of California 1215 K Street, Ste. 2230 Sacramento, CA 95814 (916) 448-8292 www.lhpc.org25
Services for the Medi-Cal Managed Care program. o 16plans are local plans. Understanding Local Plans’ Role Medi-Cal Enrollment 9 All 16 community-based and not-for-profit – First and largest of our kind in the nation Publicly operated and governed – Largest publicly acc