Transcription
Babesiosis: An Underdiagnosed Disease of ChildrenPeter J. Krause, Sam R. Telford, III, Richard J. Pollack, Raymond Ryan, Peter Brassard,Lawrence Zemel and Andrew SpielmanPediatrics 1992;89;1045-1048The online version of this article, along with updated information and services, is located onthe World Wide Web at:http://www.pediatrics.orgPEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly publication, ithas been published continuously since 1948. PEDIATRICS is owned, published, and trademarked by theAmerican Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.Copyright 1992 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 0031-4005.Online ISSN: 1098-4275.Downloaded from www.pediatrics.org. Provided by UNIV OF DELAWARE on July 30, 2009
Babesiosis:PeterRaymondJ.An UnderdiagnosedKrause,Ryan,MD*;PhD;Diseaseof ChildrenJ. Pollack,PhD;Zemel,MD5; andSam R. TelfordIII, an,ScDgABSTRACT.Babesiosisis a malaria-likeillnesscausedby the intraerythrocyticparasiteBabesiamicrotiand istransmittedby the sametick that transmitsBorreliaburgdorferi,the causativeagent of Lyme disease.Babesiosis is well recognizedin adult residentsof southernNew Englandand New York but has been describedinonlyfivechildren.To determinewhetherchildrenareinfectedwithB microtiless oftenthan are adults,aprospectiveserosurveywas carried out on Block Island,RI, wherebabesiosisis endemic.Randomlyrecruitedsubjectscompleteda questionnaireand provideda bloodsample.AntibodiesagainstB microtiand B burgdorferiwere measuredusinga standardindirectimmunofluorescenceassayand enzyme-linkedimmunosorbentassay, respectively.Of 574 subjects,9% testedpositiveforB microti,including12% of the 52 children(7 monthsthrough16 years) and 8% of the 522 adults(not significant, P .6). Althoughbabesiosishad not been diagnosedin any of the Babesia-seropositivesubjects,25% of thechildrenand 20% of the adults reportedsymptomscompatiblewith this infectionduringthe previousyear. Ofthe 6 childrenand 45 adultsseropositivefor B burgdorferi, 17% and 14%, respectively,were also seropositivefor B microti.It is concludedthat childrenare infectedwith B microtino less frequentlythan are adultsandthat this infectionis underdiagnosedin all age groups.Physicianswho practicewhereLyme diseaseis endemicshouldbecomefamiliarwith the clinicalpresentationand diagnosisof babesiosis,both in adults and besiamicroti,Lyme disease.pearedwith increasingfrequencyin variouspartsofEuropeandthe UnitedStatesincludingCalifornia,Wisconsin,New York, and southernNewEngland.’Babesiosisappearsmainlyto affectolderadults;ofthe hundredsof casesthat havebeendescribed,onlyfive involvedchildren.58It seemsparadoxicalthat sofewchildrenhavebeenaffectedin spiteof theirrelativeintenseexposureto deerticks.Indeed,chilthenseemto acquireLymediseaseevenmorefrequentlythan do adults.This asymmetricalage distributionof humanbabesiosismayderivefroma tendencyof B microtitoproduceasymptomaticinfectionin childrenmorefrequentlythanin adults.To examinethis hypothesis,we conducteda prospectiveserosurveyfor babesialinfectionin residentsof BlockIsland,RI, a site inwhichthe infectionis endemic,and revieweddatafrom a large-scaleretrospectivebabesiosisserosurveyin Connecticut.In particular,we comparedserologicand parasitologicevidenceof infectionin thesesubjects with any clinicalhistoryof babesialdisease.castingover a say;PBS,phos-From the Departmentsof Pediaincsand LaboratoryMedicine,The University of ConnecticutSchoolof Medicine,Farmington;HartfordHospital,Hartford,CT; The Universityof en’sHospital.Newington,CT; §Departmentof TropicalPublicHealth,The HarvardSchoolof PublicHealth,Boston,MA; ublicationJulto (P.J.K.)25,DeptBrown1991;acceptedof Pediatrics,UniversitySchoolofSep 27, 1991.HartfordHospital,Medicine,Hartford,emyof Pediatrics.(ISSN00314005).Copyright 1992bytheAmericanAcad-of BlockIslandResidentsfrom the full-timeresidentsof Block Island, RI, werefor evidence of babesiosis as well as Lyme disease betweenSeptemberparticipate1990 andby postinganda bloodRetrospectiveFebruary1991. We invitedthese subjectstonotices in the local newspaperand by broadtelevisionrespondents,network.Aftera questionnairedrawn.wereandThosesubjectslater ncorn-weresero-they wereexaminedsamplewas obtained.of ConnecticutResidentsIn a previousserosurveysera reactedwith antigenof 735 Connecticutresidentswhoseof the agent of Lyme diseasebetween1986 and 1989,70 also reactedwith Babesia antigen.9 We contactedas many of these seroreactivesubjectsas possibleand inquiredabouttheir age and any previousillnessthat mightrelatetobabesiosisand Lyme disease.Because these blood samplesgenerally had beenobtainedfrommailedthemto the Universityvariousprivateof Connecticutmation about many of the patients,was unavailable.ImmunofluorescenceA standardto detectfromthein femalealternatingat leastCT 06115.PEDIATRICSSerascreenedSerosurveypositivefor babesiosisby a physician(P.J.K.),NS, not significant.Humanbabesiosisis a malaria-likeillnesscausedby an abesiamicroti)thatis transmittedin thenortheasternUnitedStatesby the samedeerticks(Ixodesdammini)thattransmitthe agentof n aresidentof Yugoslaviain SProspectivecollectedAssaytheir age and address,for Antibodyto B microtiimmunofluorescenceassay (IFA) was usedto B microti.’#{176}Antigenfor the IFA was derivedof B microti that was kept in continuouspassageof erythrocytesin a syringeing halothaneincludingindirectantibodyGI straingoldenhamsterswithpassage40%laboratoriesthat hadHealthCenter,infor-by monthlyintraperitonealinoculation,througha vectorevery4 sia.Thebybloodwas1 mL of bloodcardiacpuncturecentrifugedDownloaded from www.pediatrics.org. Provided by UNIV OFPEDIATRICSDELAWAREVol.on July89 30,No. 20096 June1992wasfollow-at 500X1045g
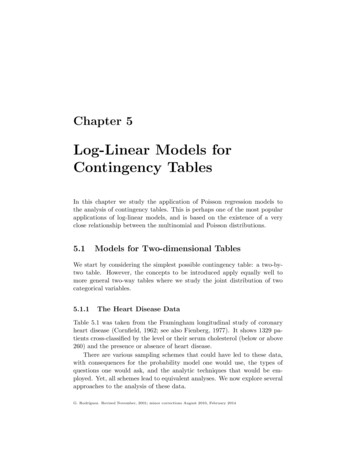
for 5 minutes,the plasmawas removed,dilutedin 10 mL of phosphate-bufferedcellswerewashedthatthicksmearsA he packedsaline(PBS,and resuspendedPBS100 to 500drop of cell suspensionglassandpiroplasms7.6). Thein PBS soper fieldwas addedat 23#{176}C,andcells werepHwereperformedeveryfilmswere10 daystakenfrom bloodwellingfrom a cutexaminedas described.Freshsmearsfor 3 months.(400to eachwellin a desiccatorstoredmonitoredby thin bloodon the tip of the tail andof aat-20#{176}Cfor up to 1 month.For IFA testing,slides were warmedtoroom temperature,test sera were diluted1:32 in PBS, and 20 tL ofdilutionwas addedto a slidewell.Eachslidewas incubated30 minutesat 35#{176}C,washedthreetimeswith agitationin PBS,and air dried.A 20-saLdropof or 1gM ilutedin PBS andEvansblue(finalconcentrationof 0.0005%)was addedto eachwell and incubatedfor 30 minutesat 35#{176}C.The slidewas samongt test as appropriate.groupswereexaminedA P valueof .05waswith aconsideredx2analysisorsignificant.theforwith agitationin PBS, air dried, and the coverslipmountedwithbufferedglycerin.Slides were examinedat 630x, using a 63x oilimmersionobjective.For comparison,each series of tests includedseruma patientcontrol’),control’),and PBS.All specimenswith(afromwith babesiosisconfirmedwitha bloodsmearserumfroma normalpatient(a ‘negativeReactionsweregradedon a scaleof 0 to 4 .a 1 to 2 reactionwereretested.positiveA positiveinitial studyconservativecutoffserumwas definedas one reactingof babesiosisin Connecticutresidents,positivecutoff value of nd specificityvariabilitysera,(n 8) andfoundthe sensitivitythan 95%. No day-to-dayweredilutedto endpoint.wehaveof this assay to be greaterof thetestEnzyme-LinkedB burgdorferiwasnoted.All seraImmunosorbentSeroreactivityusingan assayspirocheteantibody-positive8) test to thepreviouslyat 1:32. In anwe adoptedaa 1:32 ,50 Lwasdeterminedof a standardizedsuspension(strain259 1 , ConnecticutAgriculturalExNew Haven,CT) was added to alternatewells ntStation,flat-bottomRochester,NY). In thecontrol for ng.andaL ofPlatesstoredPBSwerewasdriedaddedas aovernightat -20#{176}C.At the timeatof testing,200 ML of PBS containing5% horseserumand0.01%dextransulfatewas addedto eachwell and incubatedat 37#{176}Cfor 1 hourto blockunusedproteinbindingsites. Plateswere washedsix timeswithPBS-Tween20, and 60 L of patientsera diluted1:160and1 :320 was addedto differentwells.Plateswerethen incubatedfor1 hourat 37#{176}Cin a humidchamber,thenwashedsix timeswithPBS-Tween20 followedby the additionof 60 Lof peroxidase-labeledanti-humanIgG (1:5000)or anti-human1gM (1:5000).Followingan incubationfor I hour in a 37#{176}Chumid chamber,theplateswere washedagain six times with PBS-Tween20. Sixtymicrolitersof the jKirkegaardandPerry)wason a spectrophotometerof the 1 : 160 dilutiondensityreadingof theor 0.5 for 1gM.absorbancethreethestandardBabesiaThinto eachvolumeshydrogenwell.of 2,2’peroxide,Plateswerereadminusconsideredtheor morepositivenonspecificabovewhenbindingthe waswelldeviationscontroladded(equalandat 414 nm whenthe opticaldensityreadingof the positivecontrolminusthe opticalnonspecificbindingwell equaled1 .0 for IgGA sample(antigennegativechromagensmearsin preparedcetate-anticoagulatedblood samples,fixed in absolutemethanol,and stainedfor 1 hour in 5% Giemsaat pH 7.0. The slides werewashed,dried, and coverslipped.Each was viewed microscopicallyat 400xmagnificationsusing a high-dryobjective.At least 100such fields were examinedbeforedeclaringthe samplefree vewas establishedby 5 g te-anticoagulated1046to Detectofof anpiroplasmsoil-immersionwereseen,objectiveB ng50withI mL of ethylenedi-DuplicatehamsterstowereRESULTSFirst, we describedthe age and sex distributionofBlockIslandresidentswhosesera inedfrom72%of the 800 permanentislandresidents,including52 children(median10 years,range7 monthsthrough16 years)and 522 adults(median48 years,range17through83 years).Of the 52 children,29 (56%)weremaleand 23 (44%)femalewhileof the 522 adults,260 (50%)weremaleand262 (50%)werefemale.The sera of 9% of these574 subjectscontainedIgGantibodythatreactedwithB microtiantigen;nonecontainedreactive1gM antibody(Table1). Sera of 6(12%)of the 52 childrencontainedreactiveantibody,a prevalenceestimatethat doesnot differfromthatof adults(not significant[NS], x2 0.25,P .6). Thegeometricmeantiter was greaterin children(144 5) than in adults(86 3, NS, P .3). The percentageof maleswhosesera containedantibodythat reactedwithB microtiantigen(14%in childrenand 9% inadults)wasnot significantlydifferentthanthatoffemales(9% in childrenand 8% in adults;NS, x2 0.3 and 0.1, respectively,P .6 and .8, respectively).The potentialeffectof bias in this bodyof dataisminimizedbecauseour studysampleincludedall butaboutone quarterof the total populationof the island.We concludedthatBlockIslandchildrenwereexposedto babesialinfectionaboutas frequentlyaswere adults.We recordedthe prevalenceof antibabesialantibodyin a sampleof residentsof Connecticutwhosesera reactedwiththe agentof Lymedisease.In all,the sera of 735 peoplewerestudied.Informationonage was availablefrom 227 of these subjects.The seraof 46 of these227 subjectsreactedwithB microtiantigen.As in the Block Islandstudy,the proportionof apparentlyinfectedchildrendid not differfromthat of adults(Table1).The age distributionof BlockIslandsubjectsseropositivefor B microtiwas thenanalyzedin gh59, 60 through83 years)(Figure).Althoughtheproportionof seropositivechildrenmayhavemarginallyexceededthat of adultsin any of the agedivisionsanalyzed,no differencesbetweenage incrementscouldbe demonstrated.A similarage distributionof seropositivitywas evidentwhenB burgdorf en antigenwas used.In bothgroups,childrenwereas likelyto be seropositiveas wereadults.Overall,the sera of about9% of Block Islandsubjectsreactedwith B microtiantigen.Noneof the bloodsmearsobtainedfromsubjectsseropositivefor B microticontainedpiroplasms.ViableB microtiorganismsweredetectedin hamstersinjectedwith bloodfrom 1 of 23 seropositiveadultsandfrom none of 3 seropositivechildren.The adult whoseBABESIOSISDownloaded from www.pediatrics.org. Provided by UNIV OF DELAWARE on July 30, 2009
TABLESampled1.onPrevalenBlock Islance of Antibodyd (RI) and SelectedLocationComparisonWithBabesiaof Connecticut*ChildrenBlock IslandConnecticut*ReactingAreasof datawithinmicrotiAntigenin SeraAdultsof SubjectsTotalNo.% PosNo.% onnecticutgroupsindicatedthat% Postheseraof childrenreactedwithB microti antigenaboutas frequentlyas did thoseof adults.Connecticutresultscouldnotbe comparedwiththosefromBlockIslandbecauseof differencesin samplingtechnique.MoreConnecticutsubjectswhosesera werereactiveagainstB microtiantigen(46 of 74) werecontactedthanwerenonreactivesubjects(181 of 661).Althoughan antibodytiter of 1:32 againstBabesiaantigenwasfoundto correlatewith babesialinfectionin the presentstudy(see text), a titer of I :64 was usedas thecutofffor seropositivesubjectsin a previouspublication.9DISCUSSIONWe have demonstratedthat B microtiinfectionis atleastas prevalentin childrenresidingwherethiszoonosisis intenseas in adults.AlthoughLymediseaseis moreprevalent,the age distributionof the ears)Figure.Agedistributionof BlockreactedwithBabesiamicrotiantigensera loodinfectedhamsterswasa 64-year-oldwomanwitha B microtiantibodytiter of 1:1024.Althoughthis findingof an activeinfectionsupportsthe validityof our serologictest, seropositivitygenerallyappearsto reflecta remoteepisodeof past infection.We thenconsideredthe hypothesisthatbabesialinfectionsare underdiagnosedin childrenbecausepediatricinfectionsmaybe less symptomaticthanthoseof adults.We comparedthe percentageof childrenand adultsseropositivefor B toms.Subjects were consideredto have had an illnessconsistentwith babesiosisif they wereill for morethan1 weekandhadfeverandchillsandone or moreof a,orevidenceof hemolysis.Subjectswitha historyofLymediseasewereexcludedfromthe lyhavebeendue to Lymedisease.Althoughbabesiosishad not beendiagnosedin any of the seropositivesubjects,1 (33%)of 3 childrenand5 (15%)of 34adultsreportedan illnesscompatiblewith babesiosisduringthe previousyear. We did not ask seronegativesubjectswhetherthey may haveexperiencedsimilarepisodesof illness.On physicalexamination,noneofthe 6 seropositivechildrenor 45 seropositiveadultshad splenomegalyor onssuggestthat babesiosisgenerallyproducesan episodeof milddiseaseinchildrenbut do not permitrigorouscorrelationofseveritywith age.is similar.Thiscommonalityis consistentwiththe modeof transmissionof omyscusleucopus)and subadultdeer ticks,and bothkindsof hostfrequentlyare coinfected.The paucityof casesreportedin children,thus,doesnot appearto resultfroma lesserlevelof infectionin childrenthaninadults.Theproportionof B microti-infectedadultresidentsof the nearbyislandof Nantucketwhoexpressrelevantsymptoms(30%)is similarto thatobservedin the besialinfectionis underreportedinchildren,but not becausepediatricinfectionis nonexistentor unapparent.Althoughbabesialinfectionin childrenis not silent,the intensityof the illnessin adulthostsappearstobe greaterin thoseolderthan 40 yearsof age than inyoungeradults.’2Interestingly,the publishedreportsof pediatricbabesiosisassembledin Table2 indicatethat this conditionmay resultin debilitatingepisodesof disease.58Additionalworkis neededto clarifytheclinicalspectrumof babesialillnessin childrenas wellas adults.The scarcityof reportedpediatricdiagnosisof babesiosismayderivefromthe generalconceptthat babesiosisis a geriatricratherthana pediatricdisease.Indeed,a greaternumberof febrileillnessesaffectchildrenthanadults,and any febrileillnessinan adulttendsto be more aggressivelyevaluatedthana similarproblemin a child.Our studyindicatesthatbabesiosisis underreportedin all age groups.Practicing physicianscommonlyfail to considera diagnosisof babesiosis.Diagnosisof babesiosisdependson recognitionofan arrayof megaly,and anemia.Aloneand in combinationtheyresemblethoseof a varietyof moreprevalentinfections.’3Specificdiagnosiscan be renderedby (1) directobservationof stainedthin-filmspreparedfrompatient’sblood,(2) amplificationofinfectionby injectingpatient’sbloodinto hamsters,or (3) observinga fourfoldrise in antibodytiter.Babesiosisshouldbe consideredin any residentof scause.A reportedbite by a smalltick or ofDownloaded from www.pediatrics.org. Provided by UNIV OF DELAWARE on July 30, 2009ARTICLES1047
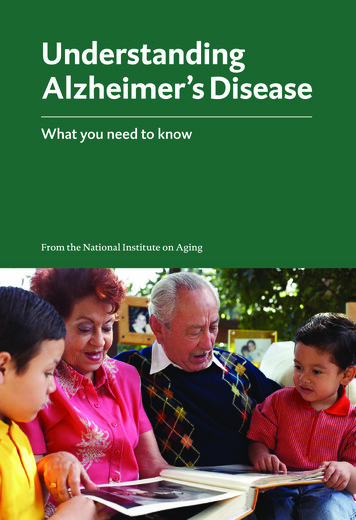
TABLE2.ClinicalAgeSummaryIllnessof PreviouslySeverityReportedIllnessDuration,2 moPediatricCasesof BabesiosisErythrocytesdAb TiterInfected,to BabesiamicrotiAntibiotic*No. of%ReferenceTransfusionsSevere38Moderate4210243 wkModerate5610242moMild2114 17amp0718gentclindaI mo*chloro,Moderatechlor oquine;5quin, quinineclinda,;5clindamicm; amp,512ampicilliinfectionby the agentof Lymediseaseshouldalertmedicalpractitionersto considerbabesiosisin thedifferentialdiagnosis,regardlessof age of the patient.Althoughbabesiosisbecamea reportablediseaseinRhodeIslandin 1989,no indigenouscaseshaveyetbeen reportedin spite of our evidencedemonstratinginfectionin at least50 BlockIslandresidents.Theinfectionis widespread,affectingresidentsof Connecticutas well as otherpartsof the region.CONCLUSIONSn; gent,CALLIf youhavein a researchFORPATIENTSIa erman,Burke,Felicianoand witzCRIGLER-NAJJARwhoHB,et nn Intern Med. 1982;96:601-604MathewsonHO, AndersonAE, HazardGW. Self-limitedbabesiosisin asplenectomizedchild. Pediatr Infect Dis. 1984;3:148-149ScimecaPG. WeinblattME, SchonfeldG, et al. Babesiosisin two infantsfrom EasternLong Island, NY. AJDC. 1986;140:971Esernio-JenssenD, SciemcaPG. BenachJL, et al. Transplacental/perinatal babesiosis.I Pediatr. 1987;110:570-572KrausePJ, TelfordSR. Ryan R, et al. Geographicaland temporaldistribution of babesialinfectionin Connecticut.J Clin Microbiol.1991;29:14ChisholmES, RuebushTK, Sulzer AJ, Healy GR. Babesia microti infectionin man:evaluationof an indirectimmunofluorescentantibodytest. AmI Trop Med Hyg. 1978;27:14-19MagnarelliLA, MeeganJM, AndersonJF, ChappellWA. Comparisonofan indirectfluorescent-antibodytest with an enzyme-linke
12-well glass IFA slide, dried at 23#{176}C,and stored in a desiccator at-20#{176}Cfor up to 1 month. For IFA testing, slides were warmed to room temperature, test sera were diluted 1:32 in PBS, and 20 tL of the dilution was added to a slide well. Each slide was incubated for 30 minutes at 35